
lncreased macrophage inflammation response in pancreatic cancer patients with a diagnosis of Shi-Re
2021-11-04 02:53YawenGengShulinYuLingQianKunChenYaleiZhangYeLiPengWang
TMR Modern Herbal Medicine 2021年4期
Yawen Geng , Shulin Yu , Ling Qian, Kun Chen , Yalei Zhang, Ye Li*, Peng Wang*
1 Department of Integrative Oncology, Fudan University Shanghai Cancer Center, Shanghai 200032, China.
2 Department of Oncology, Shanghai Medical College, Fudan University, Shanghai 2000332, China.
Abstract Objective:Traditional Chinese medicine (TCM) is a comprehensive system of medical practice.ZHENG (also known as syndrome differentiation) is the essence of TCM; however, its molecular basis remains unknown.This study evaluated the molecular basis of Shi-Re ZHENG in patients with pancreatic cancer.Methods: A total of 144 patients with pathologically-confirmed locally advanced or metastatic pancreatic ductal adenocarcinoma (PDAC) were retrospectively recruited between June 2015 and February 2016.Two cohorts, including the discovery cohort (n = 60) and validation cohort (n = 84), were included in this study.QPlex multiplex array and an enzyme-linked immunosorbent assay were used to evaluate serum inflammatory cytokine levels of pancreatic cancer patients with different TCM ZHENG.Receiver operating characteristic (ROC) curve analysis was used to evaluate the importance of the systemic inflammation response index (SIRI) in the detection of Shi-Re ZHENG.Results:Shi-Re ZHENG patients exhibited a different expression pattern of cytokines, including interleukin (IL)-6, IL-8, chemokine (C-C motif) ligand 18 (CCL18), and C-reactive protein, than patients with other ZHENG diagnoses.M2-like macrophage-related inflammatory cytokines, such as IL-10, CCL17, and CCL22, were increased in Shi-Re ZHENG compared with non-Shi-Re ZHENGpatients.The SIRI score was significantly increased in Shi-Re ZHENG compared with non-Shi-Re ZHENG patients (P < 0.001).ROC analysis revealed that SIRI had a diagnostic value for Shi-Re ZHENG both in the discovery cohort (area under the curve [AUC] = 0.833, 95% confidence interval [CI] = 0.709–0.957) and validation cohort (AUC = 0.810, 95% CI = 0.716–0.905).Additionally, pancreatic cancer patients with Shi-Re ZHENG had a significantly shorter survival time than non-Shi-Re ZHENG (P = 0.002).Conclusion:Shi-Re pancreatic cancer patients are characterized by an increased macrophage inflammation response, which may contribute to a poorer prognosis when compared to those with other ZHENG diagnoses.
Keywords:Pancreatic cancer, Shi-Re ZHENG, Inflammation
Background
Pancreatic ductal adenocarcinoma (PDAC) is the fourth leading cause of cancer-related deaths globally, with a five-year survival rate of only 5% [1].Despite extensive research efforts, it is still associated with low survival rates, with more than 80% of patients presenting with end-stage disease or diagnosed with metastases [2].Many studies investigating new drugs have failed to demonstrate benefits.Moreover, there is also a lack of effective treatment for advanced pancreatic cancer, and the median survival time of patients with advanced disease is around 5–6 months [3].
Traditional Chinese medicine (TCM) is a comprehensive system of medical practice that has contributed to disease management in Chinese populations and throughout Asia for thousands of years [4].The concept of ZHENG (also known as “syndrome”) remains the essence of the TCM system.ZHENG reflects pathological changes of the microenvironment inside the human body and reveals the intrinsic character of disease more accurately, completely, and profoundly than symptoms alone [5].It is collected through four diagnostic methods, inspection, listening and smelling, questioning, and palpation, to recognize the condition of patients and develop effective, individualized treatment strategies [6].Under the conceptual frame of TCM ZHENG diagnosis, patients with the same disease might exhibit different ZHENGs and therefore should receive different treatment strategies.Conversely, patients with different diseases might exhibit the same ZHENG and therefore should receive the same treatment strategy [7].
A ZHENG diagnosis depends on the intuition and experience of the physician trained in TCM theory, which makes it difficult to have a standard for ZHENG differentiation and further complicates the perception of the utility and validity of the method.Therefore, an understanding of the biological process underlying TCM ZHENG is important in human disease, including pancreatic cancer.In this study, we analyzed the association between different ZHENG types and the inflammatory microenvironment of patients with pancreatic cancer.Furthermore, we also attempted to better understand how ZHENG influences the clinical outcome of PDAC with changes in the microenvironment.
Materials and methods
Patients
Ethical approval for this study was obtained from the Ethics Committee of the Fudan University Shanghai Cancer Center, Shanghai, China (Ethical approval no.050432-4-1212B).All patients provided written informed consent for study participation according to institutional guidelines.A total of 144 patients diagnosed with locally advanced or metastatic pancreatic cancer were retrospectively recruited from June 2015 to February 2016.The criteria of advanced pancreatic cancer were based on the 6th edition of the International Union Against Cancer, and included tumors invading the superior mesenteric artery and/or celiac axis, similar to stage III pancreatic cancer.
Patients underwent radiological examinations such as contrast-enhanced abdominal computerized tomography scanning, magnetic resonance imaging, and/or magnetic resonance cholangiopancreatography.Patients with acute infections such as acute pancreatitis and cholangitis were excluded from this study because acute infectious disease has been shown to affect blood cell counts.A total of 144 patients were grouped into two cohorts according to their time of enrollment, with 60 recruited into the discovery cohort and the remaining 84 enrolled in the validation cohort.
Classification of TCM ZHENG
TCM diagnostic information was collected from a uniform questionnaire completed by the participants, including demographic factors such as age and sex, and typical symptoms for different TCM ZHENGs.Standard symptom criteria used for TCM ZHENG classification were as described previously [8].Photographs of participant tongues were also taken to enable a more accurate classification.To ensure a standard and uniform ZHENG, the classification of every patient was performed concurrently by three TCM clinical experts.
Blood sample collection
Fasting venous blood samples were collected in heparinized tubes prior to conducting the cancer diagnostic interventions or treatments.Samples of serum were purified by centrifuging blood at 3000 rpm for 15 min, then the serum was collected as supernatant and cryopreserved at –80°C for further analysis.
Detection of cytokines using Q-Plex multiplex array
Cytokine detection was performed using the Q-Plex multiplex array (Quansys Biosciences, Logan, UT, USA) on a Q-View Imager (Quansys Biosciences), in accordance with the manufacturer’s protocol, as we reported previously [9].Briefly, a series of 1:2 dilutions with known concentrations of various cytokines were performed to generate calibration curves.Fifty microliters of calibrator and samples from each well were added to the Q-Plex™ Array 96-well plates and incubated at room temperature for 1 hour; the plateswere then washed and incubated with the test mixture at room temperature for 1 hour.Next, the plate was incubated with streptavidin-HRP and substrate mix at room temperature for 15 minutes.Finally, an exposure time of 270 seconds was used to image on the QView™ Imager LS.The concentration of cytokines was analyzed by Q-View™ software.
Enzyme-linked immunosorbent assay (ELISA)
The levels of interleukin (IL)-10, C-C motif chemokine ligand 17 (CCL17), and CCL22 were measured using a sandwich ELISA kit (DuoSet; R&D Systems, Minneapolis, MN) according to the manufacturer’s instructions.
Laboratory measurements
Routine laboratory measurements, including counts of neutrophils (N), lymphocytes (L), and monocytes (M) were carried out prior to conducting cancer diagnostic interventions or treatments.Subsequently, the systemic inflammation response index (SIRI) was calculated as follows: SIRI = N*M/L.The SIRI cutoff value for predicting Shi-Re ZHENG in the discovery cohort was calculated via receiver operating characteristic (ROC) analysis.
Statistical analyses
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 15.0 (SPSS, Inc.).All data are presented as means ± standard deviation.Differences between two groups were compared using the Student’s t-test.Overall survival (OS) was determined as the time interval from initial diagnosis until death.The OS of patients in different groups was analyzed by the Kaplan–Meier curve, and survival differences were estimated using the log-rank test.P< 0.05 were regarded as statistically significant.
Results
Clinical–pathological features
A total of 144 patients with pancreatic cancer were included in the present study.Of these, 96 (66.7%) were aged ≥60 years old, and 93 (64.6%) were male.Most of the tumors were located in the body-tail of the pancreas (n = 83, 57.6%), with the remainder located in the head of the pancreas (n = 61, 42.4%).
According to the American Joint Committee on Cancer staging system, 34.7% (n = 50) of patients had stage III cancer and 65.3% (n = 94) had stage IV.CA 19-9 levels were ≥ 1,000 IU/ml in 59.0% (n = 85) of patients and < 1,000 IU/ml in 41% (n = 59) of patients.We divided all patients into four TCM ZHENGs: 47 (32.6%) patients in Shi-Re ZHENG, 39 (27.1%) in Pi-Xu ZHENG, 30 (20.8%) in Xue-Yu ZHENG, and 28 (19.4%) patients who could not be grouped into the other three ZHENG categories as Other ZHENG.Detailed clinicopathological characteristics are summarized in Table 1.
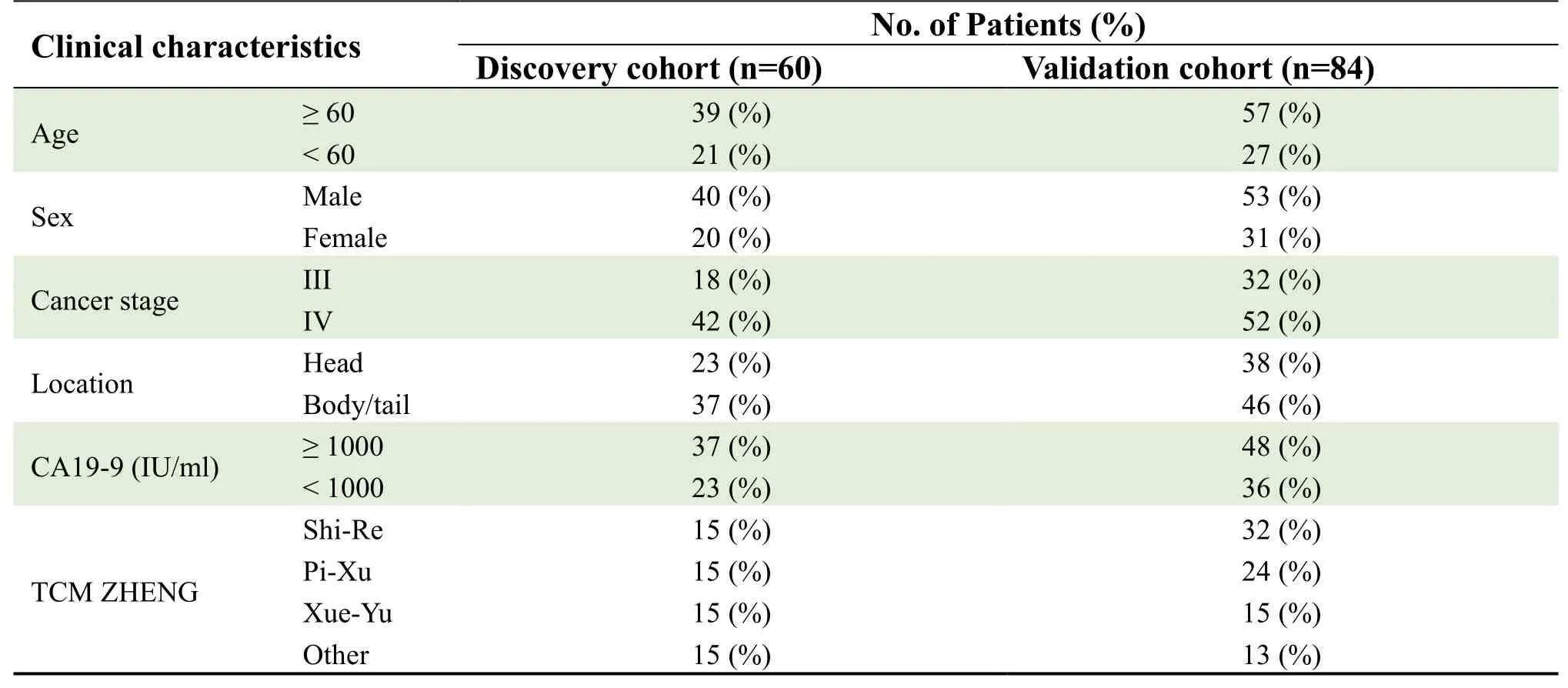
Table 1.Clinicopathological characteristics of pancreatic cancer patients.
Inflammatory cytokine levels
Inflammatory cytokine levels were evaluated in 60 pancreatic cancer patients in the discovery cohort, including 15 patients of each TCM ZHENG group.Cytokines CXCL13, CCL5, and EGF showed increased expression in the Pi-Xu group and GM-CSF was increased in the Xue-Yu group (Figure 1A).The Shi-Re group showed the greatest difference in the expression of cytokines, including IL-6, IL-8, CCL18, and CRP (Figure 1A, B).These findings indicated that TCM ZHENG was associated with an altered tumor inflammatory microenvironment in pancreatic cancer patients.
Macrophage-derived inflammatory cytokine levels
Cytokines showing increased expression in Shi-Re ZHENG patients were mainly M2-like macrophagederived.Indeed, we observed a significant increase in the expression of M2 macrophage-derived cytokines IL-10, CCL17, and CCL22 in Shi-Re ZHENG patients compared with non-Shi-Re ZHENG patients (P< 0.001,P= 0.003, andP= 0.040, respectively; Figure 2A–C).
We previously developed a systemic inflammation response index, SIRI, to reflect the status of the local immune response and systemic inflammation.[10]Here, we evaluated the correlation between SIRI and Shi-Re ZHENG, and found that SIRI significantly increased in Shi-Re ZHENG patients compared with non-Shi-Re ZHENG patients (P< 0.001; Figure 2D).ROC analysis showed that SIRI had a diagnostic value for Shi-Re ZHENG in advanced pancreatic cancer patients at a cutoff of 3.25 (AUC = 0.833, 95% CI = 0.709–0.957; Figure 2E).
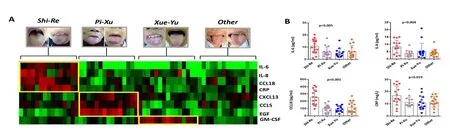
Figure 1.The expression of inflammatory cytokine levels in advanced pancreatic cancer patients with different ZHENGs.
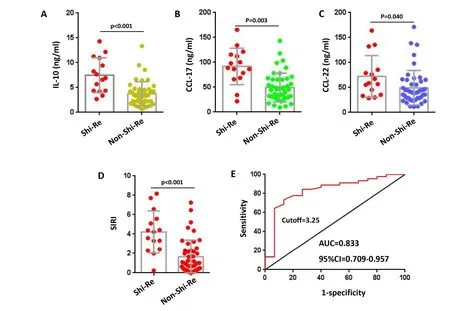
Figure 2.The macrophage inflammation response in pancreatic cancer patients with Shi-Re ZHENG and non-Shi-Re ZHENG.

Figure 3.The clinical value of SIRI in the detection of Shi-Re ZHENG.
SIRI clinical value
We further evaluated the value of SIRI in the detection of Shi-Re ZHENG in the validation cohort, in which Shi-Re ZHENG accounted for 38.1%, Pi-Xu ZHENG for 28.6%, Xue-Yu ZHENG for 17.9%, and Other for 15.5% of patients (Figure 3A).SIRI was found to be significantly higher in Shi-Re ZHENG compared with other ZHENG patients (P< 0.001; Figure 3B).Comparing the sensitivity and specificity of ROC analysis in the discovery cohort, SIRI was shown to predict Shi-Re ZHENG at a cutoff of 3.25.Using ROC analysis at a cutoff of 3.25 revealed that SIRI also had a diagnostic value for Shi-Re ZHENG in the validation cohort (AUC = 0.810, 95% CI = 0.716–0.905; Figure 3C).
Shi-Re ZHENG and prognosis
We next examined the correlation between SIRI and OS in the validation cohort of 84 patients.The median OS for patients in this cohort was 3.5 months for those with SIRI scores ≥ 3.5 and 7.6 months for those with SIRI scores <3.5 (P< 0.001; Figure 4A), indicating a significantly shorter survival time in the former group.Kaplan–Meier analyses further demonstrated the association between Shi-Re ZHENG and OS, with the median OS being significantly shorter (4.5 months) in Shi-Re ZHENG pancreatic cancer patients compared with those in other ZHENG groups (8.8 months for Pi-Xu ZHENG, 6.7 months for Xue-Yu ZHENG, and 7.2 months for Other) (P= 0.002; Figure 4B).
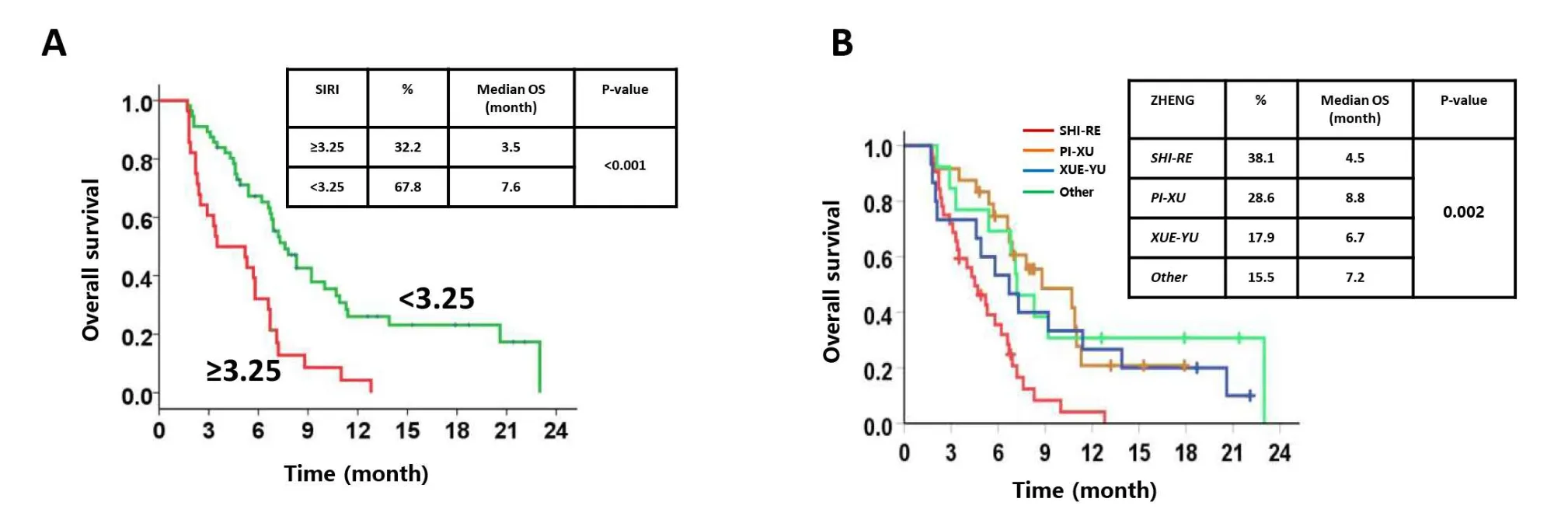
Figure 4.Shi-Re ZHENG was associated with poor prognosis.
Discussion
ZHENG, also known as the TCM pattern or TCM syndrome, is an essential and integral component of the TCM theory.A recent study demonstrated that Shi-Re ZHENG patients with colorectal cancer expressed higher levels of inflammatory cytokines (IL-1a, cyclooxygenase-2, and CCL-2) and proliferationassociated transcription factors (Ki-67 and proliferating cell nuclear antigen) than Pi-Xu ZHENG patients and had a worse survival [11].Moreover, Yinet alestablished a pancreatic cancer xenograft mouse model and demonstrated altered tumor-associated macrophage infiltration and cancer-associated myofibroblast proliferative activities in Shi-Re ZHENG mice.[12]The application of ZHENG in cancer patients could not only enhance the efficacy of treatment but also affect the clinical outcome.[13]In our study, we found that Shi-Re is the most common ZHENG in pancreatic cancer patients, and that these patients have a poor prognosis compared with those with other ZHENG types.
Cancer-related inflammation has been proposed as the seventh hallmark of cancer.[14]Several pieces of evidence have shown that the tumor microenvironment (TME) engages in cancer initiation and the promotion of tumor growth.The PDAC microenvironment is characterized by a dense desmoplastic stroma [15] which accounts for up to 50%–80% of the tumor volume [16].Tumor-associated macrophages (TAMs) are the most dominant stromal cell population in the TME of many tumors, including PDAC.TAMs were first described in the early 1980s, and their importance in promoting tumor initiation and development has been increasingly recognized, with their infiltration into tumors recently being correlated with poor prognosis [17-19].TAM-expressed CCL18 induces cancer cell epithelial–mesenchymal transition (EMT) via a feedback loop in breast cancer [20],while TAMs also promote EMT in pancreatic cancer by activating the Toll-like receptor 4/IL-10 signaling pathway [21, 22].Several TAM-secreted cytokines (including IL-4, IL-10, hepatocyte growth factor, vascular endothelial growth factor, and transforming growth factor-β) and chemokines (such as CCL17, CCL18, CCL22, CCL2, and CCL5) function in immunosuppression, proinflammation, angiogenesis, and metastasis [23, 24].In our research, we demonstrated that Shi-Re ZHENG patients exhibited higher serum levels of TAM-derived cytokines including IL-10, CCL17, CCL18, and CCL22.We also observed differences in cytokine expression among pancreatic cancer patients with different TCM ZHENG.In particular, those in the Shi-Re ZHENG group showed differences in the expression of cytokines associated with an M2-like macrophage inflammation response.
We previously developed a novel systemic inflammation response index, SIRI, based on the counts of monocytes, lymphocytes, and peripheral neutrophils, which can be applied to predict the survival of pancreatic cancer patients treated with chemotherapy, and improve the efficacy of individualized treatments [10].Its prediction ability is stronger than that of other inflammatory indexes, including the neutrophil: lymphocyte ratio and platelet: lymphocyte ratio, and is related to higher serum levels of inflammatory cytokines/chemokines IL-10, CCL17, CCL18, and CCL22.High SIRI scores are indicative of poor outcomes, and their value in assessing the prognosis of patients was also demonstrated in other carcinomas such as nasopharyngeal carcinoma and esophageal squamous cell carcinoma [25, 26].SIRI could be used to predict treatment responses to chemotherapy as an “immunologic signature” in different types of cancers, which would help clinicians identify those patients who would most benefit most therapy [27].Here, we demonstrated a correlation between SIRI and Shi-Re ZHENG, with Shi-Re ZHENG patients having higher SIRI values associated with increased serum levels of inflammatory cytokines/chemokines, and significantly shorter outcomes than other patients with advanced pancreatic cancer.
A main strength of this study lies in our attempt to elucidate TCM ZHENG within the perspective of an inflammatory microenvironment.We demonstrated that different types of cytokines are expressed in different TCM ZHENGs, suggesting a molecular basis for ZHENG.TAMs have been confirmed to suppress immune responses and believed to contribute to tumor invasion and progression [28].TAM-related inflammatory cytokines, like IL-6, IL-10, IL-17 and IL-22 are also involved in process [29, 30].An imbalanced adjustment in TAM-related inflammatory cytokines has been regarded as an important pro-inflammatory regulator in the tumor microenvironment.We previously showed that the infiltration of TAMs and the activity of cancer-associated fibroblasts (CAFs) were altered under different ZHENGs condition.Accordingly, the expression levels of TAM-derived cytokines and CAF-derived chemokines were altered, such as TAM-related CCL5/CCR5 and CAF-related SDF-1/CXCR4 [31].Based on the roles of TAMs and related inflammatory factors in cancer, we proposed that the TAM infiltration and TAM-related inflammatory cytokines might be the key to influencing ZHENGs.
We further explained the relationship between Shi-Re ZHENG and the inflammatory microenvironment using the previously established inflammatory index, SIRI, to show that SIRI could be used for the diagnosis of Shi-Re ZHENG.Most importantly, ZHENG was found not only to exist as a concept, but also to have potential clinical value for the outcome of pancreatic cancer.A study limitation is that the research is a preliminary exploratory study.However, the future application of multi-omics technology will help explain the biological basis of ZHENG more systematically and comprehensively.
Conclusion
Shi-Re pancreatic cancer patients are characterized by an increased macrophage inflammation response, which may contribute to a poorer prognosis when compared to those with other ZHENG diagnoses.
 TMR Modern Herbal Medicine2021年4期
TMR Modern Herbal Medicine2021年4期
- TMR Modern Herbal Medicine的其它文章
- Research progress on mechanism of Chinese material medica in preventing and treating insulin resistance and type 2 diabetes mellitus
- Experimental study on the effect of Huangqi and Danshen ultramicro gel on vascular healing of wound in rats based on network pharmacology
- The clinical efficacy of traditional Chinese medicine in the auxiliary treatment of grade 1 hypertension: A systematic review and metaanalysis
- Network pharmacology-based analysis on bioactive compounds and mechanisms in Yiqifumai formula in the treatment of heart failure
- Application of Chinese Herbal Medicine in the lnhibition of Salmonella and its virulence
- Differential expression of exosomal circRNAs and regulatory framework genes in myocardial infarction patients with cardiac remodeling in response to Tongguan Capsules