
Patients’ time in therapeutic range on warfarin among atrial fibrillation patients in Warfarin Medication Therapy Adherence Clinic
2021-10-09 03:03:06SiewLingLeeThienJianOngWardatiMazlanKepliAnnuysiaMageswaranKaiHsinTanAbdulMuizzAbdMalekRobertCronshaw
World Journal of Cardiology 2021年9期
Siew Ling Lee,Thien Jian Ong,Wardati Mazlan-Kepli,Annuysia Mageswaran,Kai Hsin Tan,Abdul-Muizz Abd-Malek,Robert Cronshaw
Siew Ling Lee,Thien Jian Ong,Wardati Mazlan-Kepli,Annuysia Mageswaran,Kai Hsin Tan,Department of Pharmacy,Hospital Serdang,Ministry of Health Malaysia,Kajang 43000,Selangor,Malaysia
Abdul-Muizz Abd-Malek,Department of Cardiology,Hospital Serdang,Ministry of Health Malaysia,Kajang 43000,Selangor,Malaysia
Robert Cronshaw,College of Medical,Veterinary and Life Sciences,University of Glasgow,Glasgow G128QQ,United Kingdom
Abstract BACKGROUND The quality of warfarin therapy can be determined by the time in the therapeutic range (TTR) of international normalized ratio (INR).The estimated minimum TTR needed to achieve a benefit from warfarin therapy is ≥ 60%.AIM To determine TTR and the predictors of poor TTR among atrial fibrillation patients who receive warfarin therapy.METHODS A retrospective observational study was conducted at a cardiology referral center in Selangor,Malaysia.A total of 420 patients with atrial fibrillation and under follow-up at the pharmacist led Warfarin Medication Therapeutic Adherence Clinic between January 2014 and December 2018 were included.Patients’ clinical data,information related to warfarin therapy,and INR readings were traced through electronic Hospital Information system.A data collection form was used for data collection.The percentage of days when INR was within range was calculated using the Rosendaal method.The poor INR control category was defined as a TTR <60%.Predictors for poor TTR were further determined by using logistic regression.RESULTS A total of 420 patients [54.0% male;mean age 65.7 (10.9) years] were included.The calculated mean and median TTR were 60.6% ± 20.6% and 64% (interquartile range 48%-75%),respectively.Of the included patients,57.6% (n=242) were in the good control category and 42.4% (n=178) were in the poor control category.The annual calculated mean TTR between the year 2014 and 2018 ranged from 59.7% and 67.3%.A high HAS-BLED score of ≥ 3 was associated with poor TTR(adjusted odds ratio,2.525;95% confidence interval:1.6-3.9,P <0.001).CONCLUSION In our population,a high HAS-BLED score was associated with poor TTR.This could provide an important insight when initiating an oral anticoagulant for these patients.Patients with a high HAS-BLED score may obtain less benefit from warfarin therapy and should be considered for other available oral anticoagulants for maximum benefit.
Key Words:Atrial fibrillation;Time in therapeutic range;International normalized ratio;HAS-BLED score;Oral anticoagulants;Warfarin Medication Therapeutic Adherence Clinic
INTRODUCTION
Atrial fibrillation (AF) is usually asymptomatic and is associated with an increased risk of major adverse cardiovascular events (MACE) and mortality in patients with coronary artery disease (CAD)[1].The prevalence of AF in the Malaysian population is low at 0.54%,compared to the global average of 1%[2].
Warfarin is the most widely used anticoagulant in the world[3-5].Although novel oral anticoagulants are available,warfarin remains a viable oral anticoagulant for many patients because of its availability and cost[4,6,7].The time in therapeutic range(TTR) estimates the percentage of time a patient’s international normalized ratio (INR)is within the desired treatment range or goal and is widely used as an indicator of anticoagulation control[4,9-12].TTR is commonly used to evaluate the quality of warfarin therapy and is an essential tool for assessing the risksvsbenefits of warfarin therapy[4,8,13,14].A 10% increase in time spent out of TTR is associated with a 29%increase in the risk of mortality and a 10%-12% increase in the risk of an ischemic stroke and other thromboembolic events[13,15-17].
The aim of this study is to determine the percentage of time a patient’s INR is within the desired treatment range and the predictors of poor TTR among patients with AF who receive warfarin therapy.
MATERIALS AND METHODS
Study design
This is a retrospective observational study that was conducted in Hospital Serdang located in Kajang,Selangor.Hospital Serdang is a cardiology reference center that covers patients from Serdang,Bangi,Putrajaya,Kajang,Dengkil,and Puchong area in the state of Selangor,Malaysia.Ethical approval for this study was obtained from the Medical Research and Ethics Committee,Ministry of Health Malaysia (NMRR-19-839-46462).The study was carried out in accordance with the Declaration of Helsinki.
Study setting and study population
All AF patients under Warfarin Medication Therapeutic Adherence Clinic follow-up between 2014 to 2018 were included.The electronic Hospital Information System(eHIS) was used to extract patients’ demographics,comorbidities,information related to warfarin therapy,and INR readings.Baseline comorbidities were retrospectively retrieved according to available medical records in eHIS.The consecutive sampling method was used.A case report form was used for data collection.Each patient was allocated a patient identifier number that matched their patient registration number,in order to protect confidentiality.Patients were excluded if they discontinued warfarin therapy,died,or had less than three INR readings.
TTR
For patients with AF,the target INR range was between 2.0 to 3.0.TTR is defined as an estimate of the average time that a medication is dosed with optimal efficacy and safety[4].From previous literature,the estimate of the minimum TTR needed to achieve a benefit from warfarin therapy is between 58% and 65%[18].The percentage of days that INR was within range was calculated using the Rosendaal method[8].Thus,based on these references,we defined the “poor” TTR category as TTR <60%and the “good” TTR category as TTR >60%.
Statistical analysis
This study aimed to determine to what extent the following factors are associated with poor TTR:Age,gender,ethnicity,diabetes mellitus,hypertension,previous ischemic heart disease,chronic kidney disease,peripheral vascular disease,stroke/transient ischemic attack,deep vein thrombosis/pulmonary embolism,heart failure,chronic obstructive pulmonary disease/asthma,chronic kidney disease,dyslipidaemia,chronic rheumatic heart disease,CHA2DS2-VASc score,and HAS-BLED score.A study by Peduzziet al[19] on sample size for logistic regression suggests using a minimum event per variable value of ten.Since our study was interested in studying 17 risk factors,a minimum sample of 170 patients in the poor TTR category group was required.The study planned to recruit at least 400 samples in order to exceed the minimum sample size,as the prevalence of poor TTR was estimated at 38%[19].
Categorical variables were summarized using frequencies and proportions while continuous variables were summarized using mean ± standard deviation or median(inter-quartile range) values.Logistic regression analysis was used to calculate odds ratios (OR) and 95% confidence intervals (CI) to model the predictors of poor TTR.This analysis was repeated and adjusted to variables that were significant from the previous studies:Heart failure,chronic kidney disease,CHA2DS2-VASc score,and HAS-BLED score[20].AP<0.05 was considered significant.Point estimates and 95%CI are presented for all results.Statistical analyses were performed using IBM SPSS Statistics for Windows,version 20 (Armonk,NY,United States).
RESULTS
A total of 420 patients with AF were included in this study (Figure 1).Baseline characteristics are shown in Table 1.The mean age of the study population was 65.7 (10.9)years.There were slightly more male patients (54%,n=227) than female patients(46%,n=193).The largest ethnic population was Malay,followed by Chinese and Indian.Hypertension accounted for the highest percentage of comorbidities among patients with AF,followed by diabetes mellitus,dyslipidaemia,and ischemic heart diseases.Median CHA2DS2-VASc score was 3 (moderate risk of stroke),and median HAS-BLED score was 2 (low bleeding risk).
Time in therapeutic range
Over 5 years,the mean (standard deviation) TTR was 60.6% (20.6%) with a median of 64% (interquartile range 27%).Of the included patients,57.6% (n=242) were in the good control category,and 42.4% (n=178) were in the poor control category (Table 2).The annual calculated mean TTR between the year 2014 and 2018 ranged between 59.7% and 67.3%.The highest percentage was in 2018,with 67.3% of days within therapeutic range in AF patients.Figure 2 shows the mean TTR for AF patients from 2014 to 2018.Patient with a high HAS-BLED (score ≥ 3) had a median TTR of 55%compared to patients with a low HAS-BLED score,who had a median TTR of 68%(Figure 3).
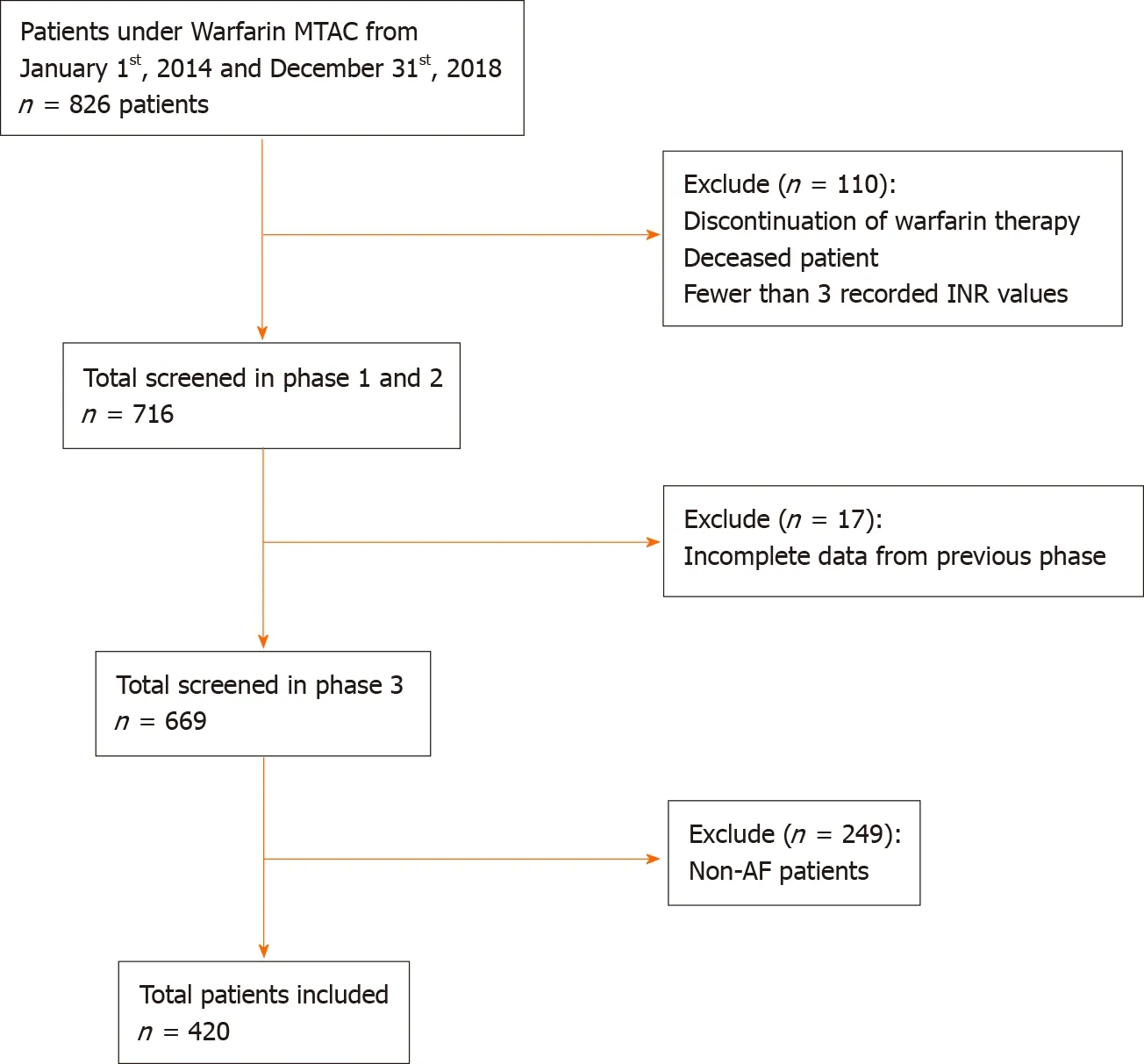
Figure 1 Flow diagram describing the selection of data for the analysis reported.

Figure 2 Mean percentage of the time in therapeutic range among atrial fibrillation patients.
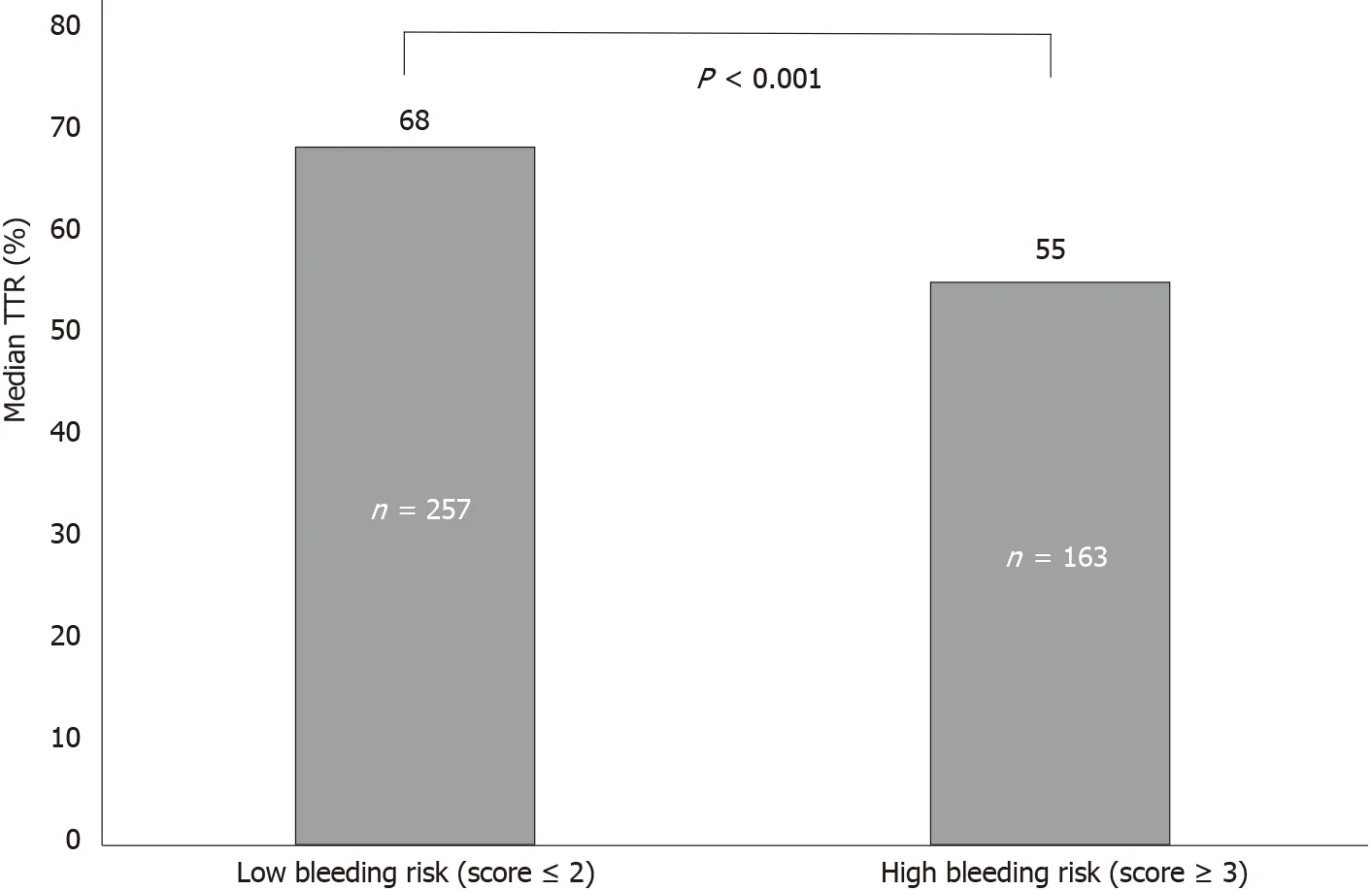
Figure 3 HAS-BLED score vs median time in therapeutic range (%).
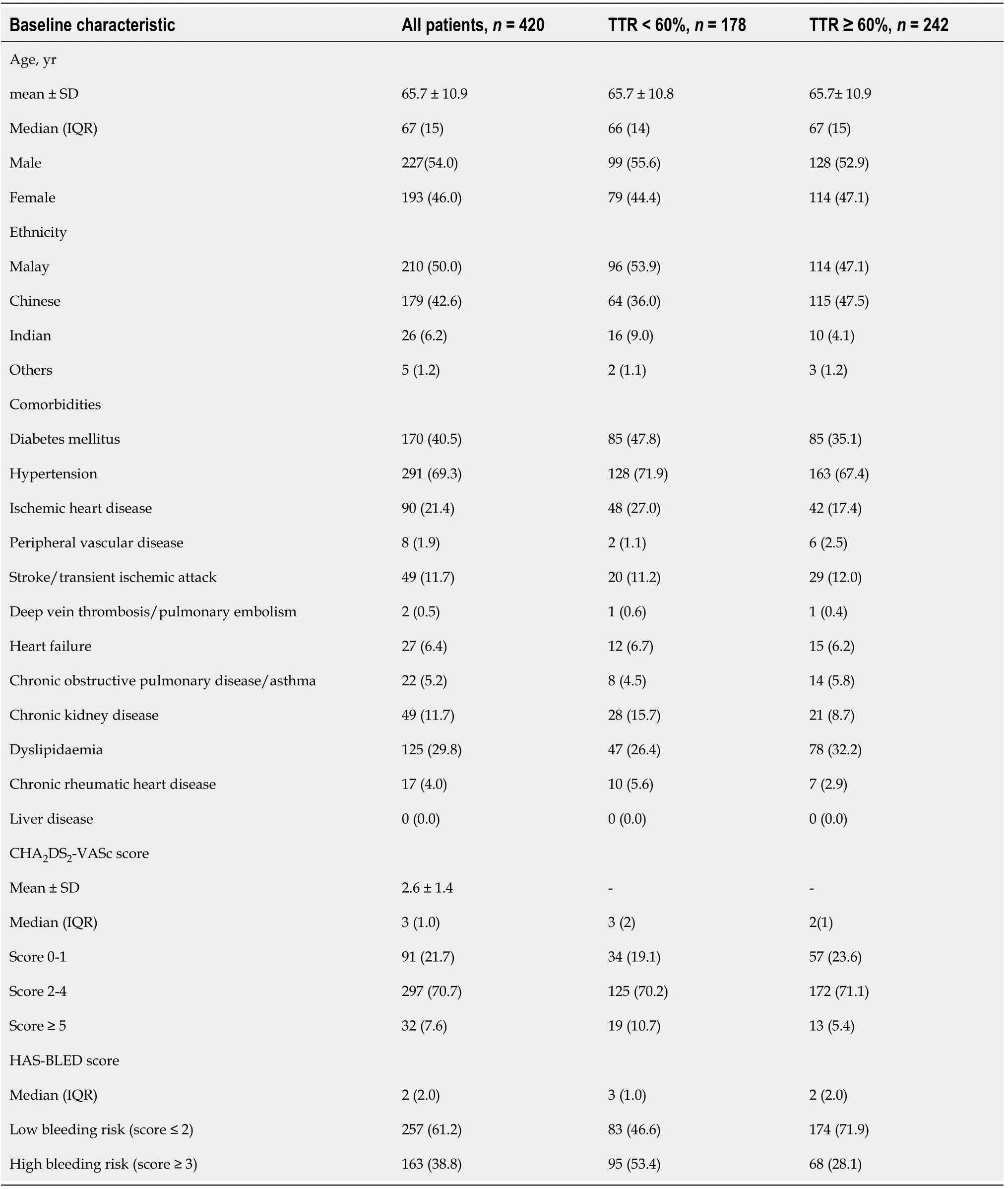
Table 1 Baseline characteristics
Predictors of poor TTR
From the multivariate analysis,a high HAS-BLED score (score ≥ 3) was significantly associated with a poor TTR (<60%) (adjusted OR,2.5;1.6-3.9,P<0.001) compared to a low HAS-BLED score (score ≤ 2).Similarly,in the model adjusted for predictors previously described in previous reports[20] (model 2),only HAS-BLED score was found to be a significant predictor of poor TTR (adjusted OR,2.9;1.8-4.7,P<0.001)(Table 3).

Table 2 Time in the therapeutic range of the study population

Table 3 Univariate and multivariate logistic regression analysis for predictors of poor time in therapeutic range <60% among atrial fibrillation patients
DISCUSSION
This study assessed the percentage of time a patient’s INR is within the desired treatment range or TTR and explored the predictors of poor TTR.Overall,the study population had a majority of men and people of Malay ethnicity.This could be explained by the Malaysian population distribution,whereby more than half of the population are of Malay ethnicity,and there are more men than women with the ratio of 107:100[21].Our results showed similarity with other international studies,with a majority of warfarin users being male[22,23].
Hypertension had the highest prevalence,followed by diabetes mellitus,hyperlipidemia,and ischemic heart disease.The higher prevalence of cardiac-related comorbidities could be explained by Hospital Serdang’s status as a cardiology center,therefore catering towards patients with cardiovascular disease in the region.Additionally,these are the main risk factors for AF,which is the study population in question[24].
Interestingly,when compared to other Asian studies,the mean TTR of patients obtained in the study was 60.6%.In comparison,a study from Korea recorded a mean TTR of 49.1%[23],and a study from Singapore recorded a mean TTR of 58%[25].Possible reasons for the higher mean TTR percentage may be due to the involvement of pharmacists in the pharmacist-led warfarin therapy.This translates to improved patient counselling,dosage adjustment,and identification of possible food-drug and drug-drug interactions.
This study found that patients with a high HAS-BLED score (≥ 3) had a lower median TTR of 55%,compared to patients with a low HAS-BLED score (score <2) who had a higher median TTR of 68%.Previous reports have suggested that heart failure,chronic kidney disease,and CHA2DS2-VASc score in addition to high bleeding risk may also contribute to poor TTR[20].After adjusting for these variables,we found only high HAS-BLED (score ≥ 3) was associated with poor TTR.This is supported by the study from Urbonaset al[15],which found median TTR was significantly lower in patients with high bleeding risk (36.4%) as compared to low-risk patients (55.6%).They suggested that the poor TTR in these patients may be due to biological variation in clotting factors[15].
Strength and limitations
Our patients’ data were derived from the eHIS database,an electronic storage system of patient records,enabling straightforward access to patient records.The INR results collected in the study were obtained either through point-of-care testing (POC) or clinical laboratory INR.There may be bias in INR measurements calculated using POC compared with laboratory INR,as POC measurements tend to be higher[10],which may affect subsequent INR readings.We were unable to measure objectively patient compliance to warfarin as a risk factor for poor TTR.Since it was a retrospective study,possible missed documentation may have occurred.
CONCLUSION
This study found the mean TTR was 60.6% in patients with AF and that a high HASBLED score (≥ 3) was associated with poor TTR.This could provide an important insight during the initiation of oral anticoagulant for patients with a high HAS-BLED score,who may obtain less benefit from warfarin therapy.They should therefore be considered for other available oral anticoagulants for maximum benefit.
ARTICLE HIGHLIGHTS
Research background
The time in therapeutic range (TTR) is a quality measure for anticoagulation therapy with warfarin.
Research motivation
TTR of international normalized ratio (INR) needs to be achieved with a percentage of≥ 60% for patient to receive a maximal benefit from warfarin such as preventing stroke,major bleeding,and even death.
Research objectives
TTR and the predictors of poor TTR need to be evaluated among atrial fibrillation (AF)patients that received warfarin therapy.
Research methods
Eligible patients with AF from January 2014 to December 2018 for INR monitoring were included in this study.Demographic data,indication of warfarin therapy,INR target,and percentage of INR within range were collected using a data collection form.TTR was assessed using Rosendaal method.
Research results
In patients with AF,the mean TTR was 60.6% with the highest TTR score achieved in 2018,with a percentage of 67.3%.
Research conclusions
This study showed that high HAS-BLED score was associated to poor TTR.
Research perspectives
Patients with AF and high HAS-BLED score may have less benefit from warfarin therapy.Thus,other alternative oral anticoagulants should be considered for maximum benefit.
ACKNOWLEDGEMENTS
The authors would like to thank the Director-General of Health Malaysia for the permission to publish this paper and to those who contributed directly or indirectly in this study.Further on,the authors would also like to thank the colleagues Siaw SH,Tam AS,Mohamad RIA,Wong KY,Noor Hisham NA,So SH,Lim SY,Tee CY,and Tang MH for their contribution in data collection.
 World Journal of Cardiology2021年9期
World Journal of Cardiology2021年9期
- World Journal of Cardiology的其它文章
- Effects of exercise training on diastolic and systolic dysfunction in patients with chronic heart failure
- Red blood cell distribution width in elderly hospitalized patients with cardiovascular disease
- Percutaneous coronary intervention of totally occluded coronary venous bypass grafts:An exercise in futility?
- Intensive lipid-lowering therapy,time to think beyond low-density lipoprotein cholesterol
- Sodium glucose cotransporter 2 inhibitors:New horizon of the heart failure pharmacotherapy
- Coronary vasospasm:A narrative review