
Fluorescence in situ hybridization-based confirmation of acute graftvshost disease diagnosis following liver transplantation:A case report
2021-10-09 05:55:10JingJingXiaoJinYuMaJunLiaoDiWuChaoLvHaiYangLiShiZuoHaiTaoZhuHuaJianGu
Jing-Jing Xiao,Jin-Yu Ma,Jun Liao,Di Wu,Chao Lv,Hai-Yang Li,Shi Zuo,Hai-Tao Zhu,Hua-Jian Gu
Jing-Jing Xiao,Jin-Yu Ma,Jun Liao,Di Wu,Chao Lv,School of Clinical Medicine,Guizhou Medical University,Guiyang 550004,Guizhou Province,China
Hai-Yang Li,Shi Zuo,Hai-Tao Zhu,Department of Hepatobiliary Surgery,The Affiliated Hospital of Guizhou Medical University,Guiyang 550004,Guizhou Province,China
Hua-Jian Gu,Department of Pediatric Surgery,The Affiliated Hospital of Guizhou Medical University,Guiyang 550004,Guizhou Province,China
Abstract BACKGROUND Although acute graft-vs-host disease (aGvHD) is a rare complication of liver transplantation,it is poorly understood and has an extremely high mortality rate.No standardized diagnostic criteria or treatment regimens currently exist.CASE SUMMARY The present study investigated the etiology,diagnosis,and treatment of aGvHD following liver transplantation.Presentation,diagnosis,disease course,histology,and treatment of an aGvHD case are reported,and associated literature is reviewed.A 64-year-old female required LTx due to primary biliary cirrhosis.The donor was a 12-year-old male.Three weeks following liver transplantation,the recipient developed pyrexia,diarrhea,rashes,and antibiotic-unresponsive pancytopenia.Clinical symptoms together with laboratory investigations suggested a diagnosis of aGvHD,which was confirmed via peripheral blood fluorescent in situ hybridization.Donor XY chromosome fluorescent in situ hybridization indicating early chimerism achieved 93% sensitivity in the detection of GvHD.Existing immunosuppressants were discontinued,and high-dose intravenous methylprednisolone was initiated along with antibiotics.While diarrhea resolved,the patient’s general condition continued to deteriorate until demise due to multi-system organ failure at 37 d post-liver transplantation.This case illustrates the life-threatening nature of aGvHD.CONCLUSION Herein,we have summarized a post-LTx aGvHD case and reviewed associated literature in order to increase awareness and provide potentially risk-mitigating recommendations.
Key Words:Liver transplantation;Graft-vs-host disease;Fluorescence in situ hybridization cytogenetics;Chimerism;Diagnosis;Case report
INTRODUCTION
Acute graft-vs-host disease (aGvHD) is one of the most dangerous complications following liver transplantation (LTx)[1].It involves overactivation of donor helper T lymphocytes by recipient antigen-presenting cells,leading to a local inflammatory reaction against recipient tissue.Although the rate of aGvHD incidence after LTx is low (1%-2%),the mortality rate is extremely high (85%-90%)[2].Skin rash and pyrexia are the most frequently noted early signs,followed by leukopenia.Although aGvHD was first proposed as a clinical entity in 1988,its mechanisms and optimal treatment strategies remain controversial[3].Modification of the post-transplant treatment plan,including incorporation of more effective immunosuppressants,has a limited effect on the course of aGvHD[4,5].In most cases,death results from overwhelming sepsis or gastrointestinal hemorrhage as a consequence of bone marrow involvement[6].Due to the low incidence (but high mortality) of aGvHD following LTx,analysis of the present case with respect to existing literature is worthwhile in order to raise awareness regarding the condition,which may assist in the early diagnosis of suspected cases.It will also help improve diagnostic criteria and establish standardized evidence-based treatment regimens.Moreover,we wish to draw attention to the diagnostic utility of sex chromosome fluorescentin situhybridization(FISH) when the donor and recipient are of different chromosomal sexes.
CASE PRESENTATION
Chief complaints
The patient was a 64-year-old female with primary biliary cirrhosis,esophageal-fundal variceal hemo-rrhages,and decompensated hepatocirrhosis in September 2017.
History of present illness
A 64-year-old female received a liver from an ABO-matched (A-positive) 12-year-old male cadaveric donor.The donor and recipient details are shown in Table 1.The donor was a 12-year-old male.Three weeks following liver transplantation,the recipient developed pyrexia,diarrhea,rashes,and antibiotic-unresponsive pancytopenia.
Table 1 Recipient and donor demographic,clinical,and typing data
History of past illness
A 64-year-old female with primary biliary cirrhosis,esophageal-fundal variceal hemorrhages,and decompensated hepatocirrhosis.
Personal and family history
The patient grew up in her locality,denies any contact with contaminated water or radiation exposure,and denies smoking and alcohol consumption.
Physical examination
On physical examination,we found her poor nutritional status,the abdomen was moderately distended with mild tenderness,and there was moderately yellow staining of the skin and mucous membranes.The rest of the physical examination revealed no abnormal findings.
Laboratory examinations
The following timeline of events refers to post-operative days.On day 22,the patient developed pyrexia of unknown origin,fluctuating between 38.2 °C and 39.3 °C.On day 26,sex chromosome FISH was performed on peripheral venous blood samples.No gastrointestinal tract lesions were apparent,and no evidence of aGvHD was noted on gastrointestinal endoscopic biopsy (histologically normal esophagus,stomach,and ileum).On day 31,the presumptive diagnosis of GvHD was made based on the following clinical ground observations:Generalized maculopapular eruption (largely involving the back,neck,and face),pyrexia,pancytopenia,low blood pressure,and watery diarrhea (Figure 1 and Table 2).FISH revealed chimerism (presence of the fluorescently stained donor XY chromosome) consistent with aGvHD (Figure 2).
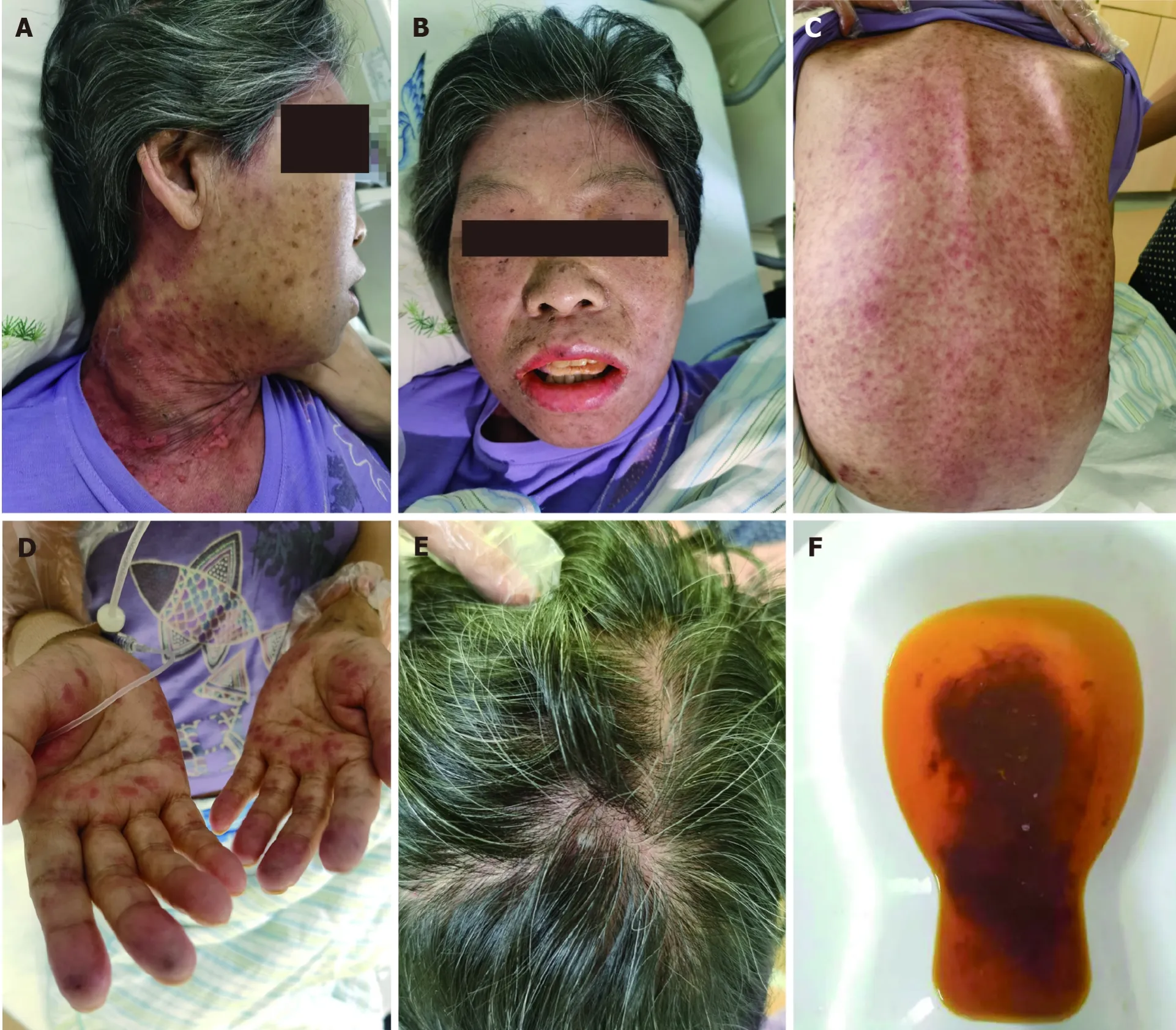
Figure 1 Clinical ground observations of graft-vs-host disease.
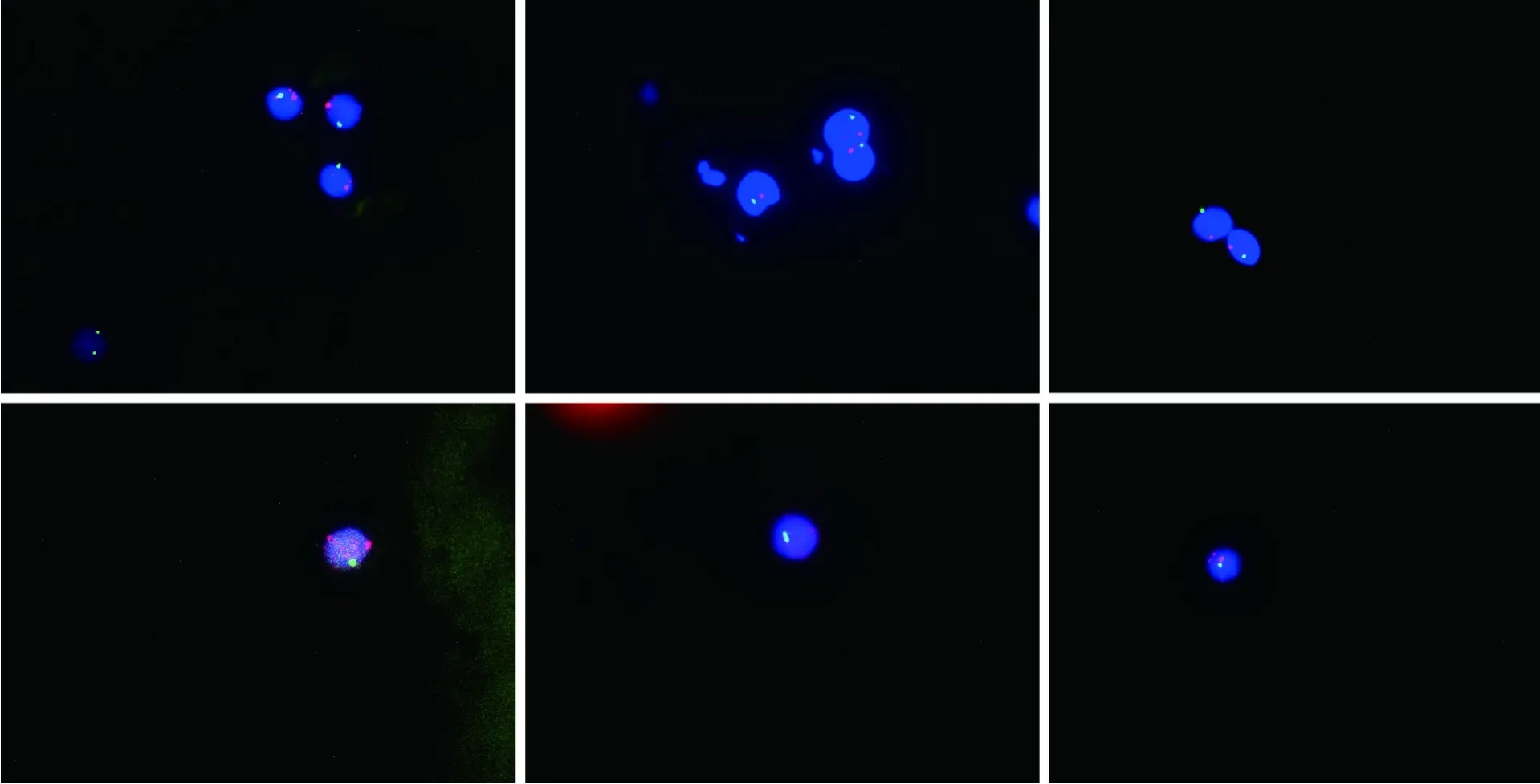
Figure 2 Twelve erythrocytes analyzed,11 showed an XY signal pattern,while one showed an XX signal pattern (91.7% showed one X and one Y signal,and 8.3% showed two X signals).
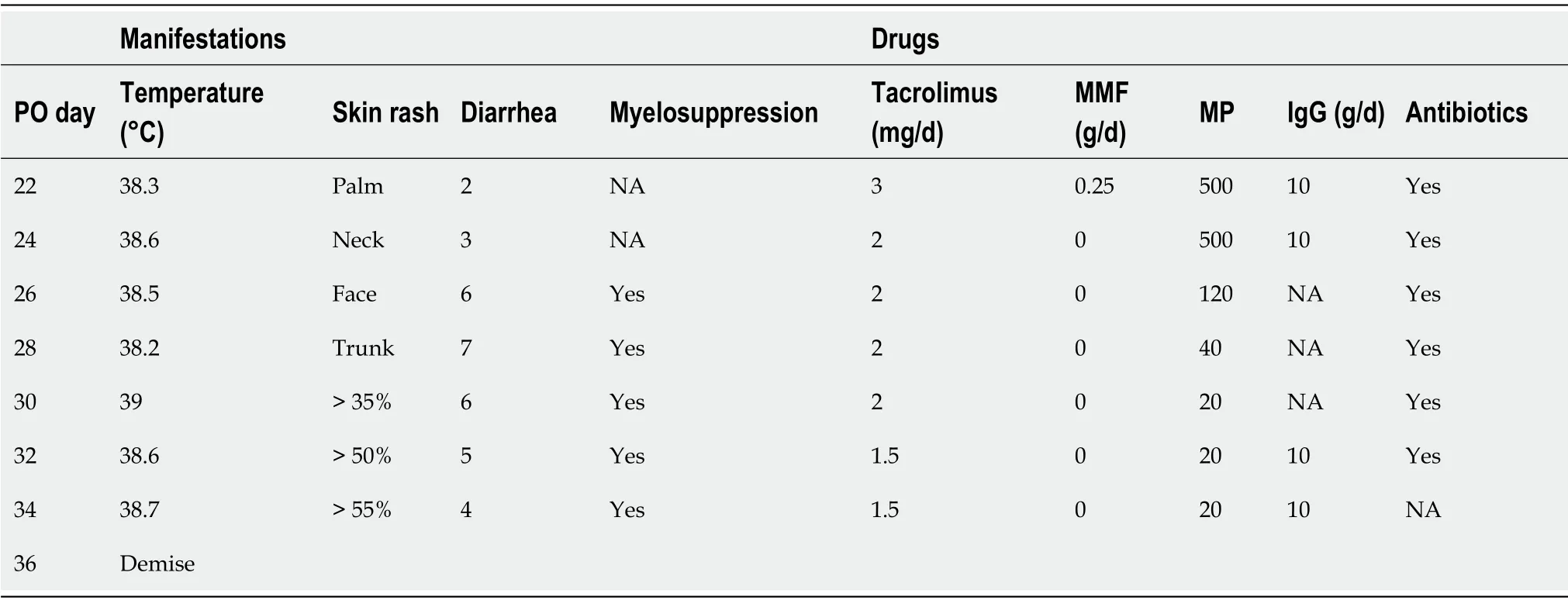
Table 2 Clinical manifestation and treatment timeline
Two days following the development of thrombocytopenia,a bone marrow biopsy revealed marked hypocellularity.No skin rash was yet apparent.The findings of detai-led post-operative laboratory investigation are summarized in Table 3.Because no sample of indwelling peripheral blood from the donor prior to LTx was available,donor lymphocytes could not be identified in recipient peripheral blood using short tandem repeat sequencing or human leukocyte antigen (HLA) typing.
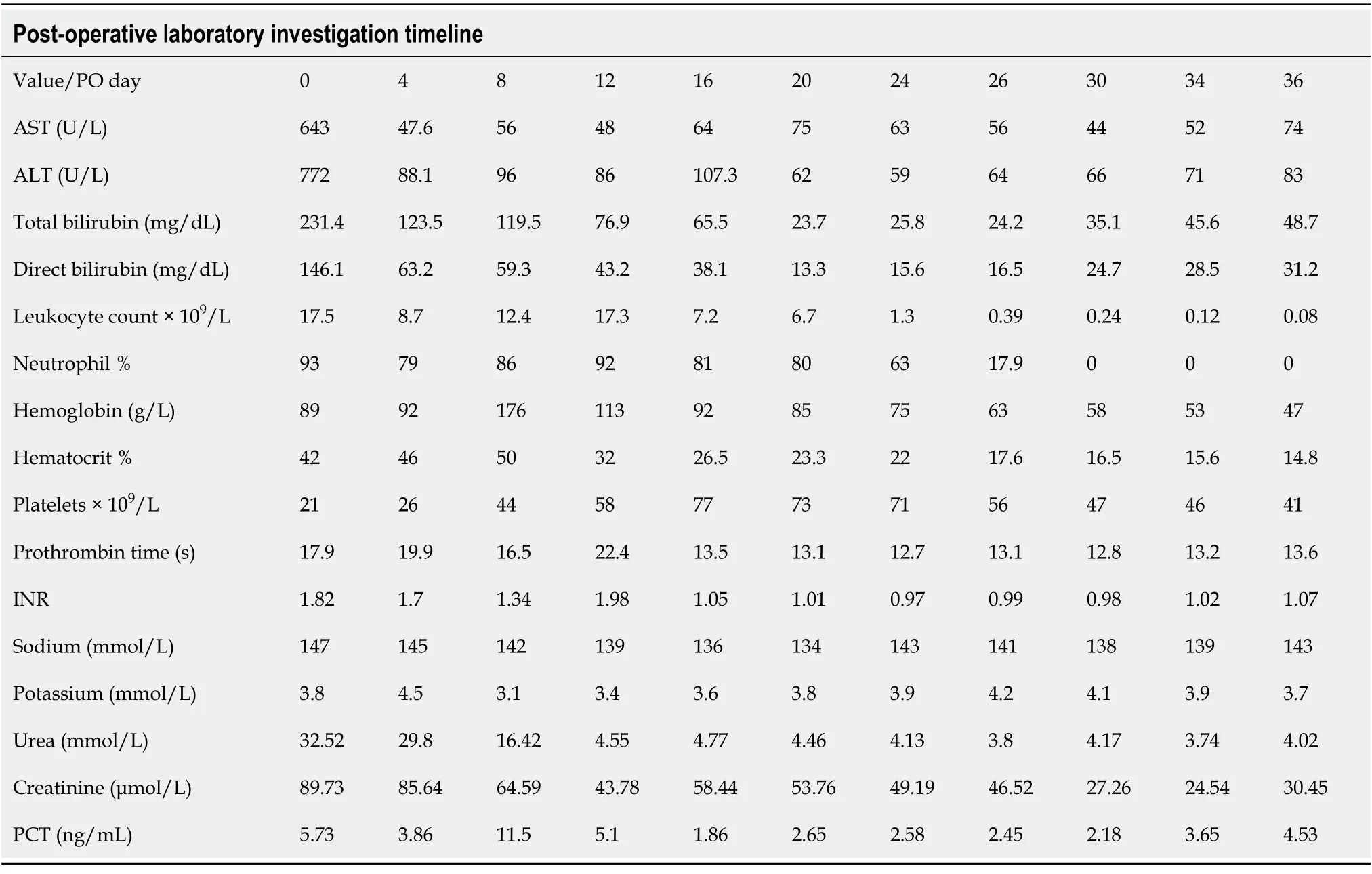
Table 3 Post-operative laboratory investigation timeline
Imaging examinations
Abdominal computed tomography and color ultrasound findings suggested laminar portal vein,inferior vena cava,hepatic artery,and hepatic venous flow (Figure 3).

Figure 3 The portal vein,inferior vena cava,hepatic artery,and hepatic venous blood flow were smooth.
FINAL DIAGNOSIS
aGvHD,primary biliary cirrhosis,esophageal-fundal variceal hemorrhages,and decom-pensated hepatocirrhosis.
TREATMENT
Initial treatment involved tapering the dosage of immunosuppressants to allow the recipient immune system to reject donor lymphocytes.Due to the inefficacy of thisapproach,the following treatment was administered subsequently:High-dose (500 mg/d) intravenous methylprednisolone,antibiotics,and immunoglobulin G (Table 2).
OUTCOME AND FOLLOW-UP
Severe inflammation induced multi-system organ failure,which led to the patient’s demise on post-operative day 37.
DISCUSSION
At present,the risk factors,pathogenesis,optimal treatment,and prognosis associated with aGvHD following LTx are unclear.Current (incomplete) understanding of aGvHD pathogenesis may be summarized as follows.The conditioning regimen induces initial recipient tissue damage,followed by auto- and alloantigen denudation in the recipient concomitant with antigen-presenting cell activation and massive inflammatory cytokine release (a “cytokine storm”).If a sufficient number of donor lymphocytes,especially T lymphocytes,of the correct specificity are present,direct recognition of and activation by antigen-presenting cell (either locally or within secondary lymphoid tissues) results in T lymphocyte interleukin (IL)-2 and IL-2R expression.Activated T-cells then stimulate donor monocytes to produce significant levels of myeloid cytokines (e.g.,IL-1 and tumor necrosis factor) and also trigger a cascade of cytotoxic signal transduction pathways,such as the perforin/granzyme B or Fas/FasL pathways (although direct cytokine-mediated injury is also possible).Finally,inflammatory infiltration in the digestive tract,skin,and bone marrow leads to severe clinical presentations[7].In the present case,abnormally high numbers of CD8+T lymphocytes were present during the acute phase of GvHD,while the CD4+ T lymphocyte:CD8+ T lymphocyte ratio was less than 0.1.This indicates that perhaps cytotoxic T lymphocytes (with a minor contribution by helper T lymphocytes) are the cells primarily involved in GvHD pathogenesis.In summary,the necessary conditions for the occurrence of aGvHD[8-10] include the presence of donor immunoreactive cells within graft tissue,presence of recipient tissue antigens not present in donor organ tissue,and inability of the recipient immune system to eliminate effectively donor leukocytes.
Triulziet al[9] have described the diagnostic criteria for aGvHD following LTx in the following three requirements:(1) Characteristic clinical symptoms affecting related organ systems (e.g.,skin,gastrointestinal tract,and bone marrow),including rash,diarrhea,and pancytopenia,among others;(2) Abnormal skin or digestive tract histology;and (3) HLA or DNA evidence of donor immunoreactive lymphocytes in involved organs or peripheral blood of the recipient.In addition to the above criteria,T lymphocyte counts and cytokine quantitation provide clear diagnostic support.Currently,the most reliable diagnostic method is specific immunostaining for donorspecific antigens.If the donor is male and the recipient is female,FISH-based detection of the Y chromosome is a diagnostic option[9,11,12].At present,no false negatives have been reported for this method.In the present case,aGvHD was confirmedviaFISH,demonstrating the presence of male donor DNA.
Due to inter-individual differences in post-operative GvHD pathogenesis and presentation,no unified treatment plan exists.Each hospital follows a unique treatment plan associated with unique advantages and disadvantages.A commonality across most centers is reduction of the tacrolimus dose,cessation of anti-metabolic immunosuppressants,decreasing the steroid dose,and administering antilymphocyte globulin[13-15].Successful treatmentviaincreasing immunosuppressant dosages has also been reported,with recommendations for cessation of all immunosuppressants in favor of isolated anti-human thymocyte globulin treatment[16].Certain patients also exhibit drug resistance or even resistance to the effects of some hormones[17].Treatment with anti-tumor necrosis factor-α or anti-IL-2 receptor monoclonal antibodies may prove beneficial[18,19].Currently,corticosteroids are the best-recognized first-line treatment agents for GvHD.Glucocorticoids exert efficient anti-inflammatory effects and can induce donor lymphocyte apoptosis.High-dose corticosteroid pulse therapy is administered during the acute phase of GvHD.It can inhibit inflammatory cell activation,thereby blocking the inflammatory cytokine cascade to improve systemic signs and symptoms.In cases of observation of GvHD symptoms(gastrointestinal disturbance,immunodeficiency despite overzealous inflammation,and deficient coagulation),hydration,electrolyte and acid-base rebalancing,nutritional support,restoration of gastrointestinal mucosal integrity,correction of microfloral imbalance,and transfusion of plasma and platelets can help mitigate poor outcomes,including severe infection[13,20].
In order to lessen mortality resulting from aGvHD,early detection and optimal standardized treatment are paramount.Additionally,an improved understanding of pathogenesis may assist in the prevention and treatment of this disorder.Based on our experience and the literature review,we make the following recommendations:Baseline (presurgical) donor and recipient blood samples should be obtained and cryopreserved.High-risk patients should routinely undergo HLA typing as a preliminary risk evaluation step.Ideally,the age difference between matched donors and recipients should not exceed 20 years.Pre-existing use of oral immunosuppressants should be minimized or discontinued prior to transplantation wherever possible.During perfusion of the donor abdominal aorta and portal vein,the effluent should run clear and the liver texture should soften.Finally,minimizing blood product infusion may lessen the rate of complications[15].
CONCLUSION
In the present case,aGvHD was confirmedviaFISH,demonstrating the presence of male donor DNA.If the donor is male and the recipient is female,FISH-based detection of the Y chromosome is a diagnostic option.
 World Journal of Gastrointestinal Surgery2021年9期
World Journal of Gastrointestinal Surgery2021年9期
- World Journal of Gastrointestinal Surgery的其它文章
- Trends of rapamycin in survival benefits of liver transplantation for hepatocellular carcinoma
- Role of minimally invasive techniques in gastrointestinal surgery:Current status and future perspectives
- Three colonic cancers,two sites of complete occlusion,one patient:A case report
- Perioperative steroid administration reduces overall complications in patients undergoing liver resection:A meta-analysis
- Literature review of the outcome of and methods used to improve transperineal repair of rectocele
- Quality of life after colorectal surgery:A prospective study of patients compared with their spouses