
Outcomes of inpatient cholecystectomy among adults with cystic fibrosis in the United States
2021-09-18 02:30:24MitchellRamseyLindsaySobotkaSomashekarKrishnaAliceHintonStephenKirkbySusanLiMichaelMearaDarwinConwellPeterStanich
Mitchell L Ramsey,Lindsay A Sobotka,Somashekar G Krishna,Alice Hinton,Stephen E Kirkby,Susan S Li,Michael P Meara,Darwin L Conwell,Peter P Stanich
Mitchell L Ramsey,Lindsay A Sobotka,Somashekar G Krishna,Darwin L Conwell,Peter P Stanich,Division of Gastroenterology,Hepatology and Nutrition,The Ohio State University Wexner Medical Center,Columbus,OH 43210,United States
Alice Hinton,Division of Biostatistics,The Ohio State University College of Public Health,Columbus,OH 43210,United States
Stephen E Kirkby,Division of Pulmonary and Critical Care Medicine,The Ohio State University Wexner Medical Center,Columbus,OH 43210,United States
Susan S Li,Division of General Internal Medicine,The Ohio State University Wexner Medical Center,Columbus,OH 43210,United States
Michael P Meara,Division of General and Gastrointestinal Surgery,The Ohio State University Wexner Medical Center,Columbus,OH 43210,United States
Abstract BACKGROUND Symptomatic biliary and gallbladder disorders are common in adults with cystic fibrosis (CF) and the prevalence may rise with increasing CF transmembrane conductance regulator modulator use.Cholecystectomy may be considered,but the outcomes of cholecystectomy are not well described among modern patients with CF.AIM To determine the risk profile of inpatient cholecystectomy in patients with CF.METHODS The Nationwide Inpatient Sample was queried from 2002 until 2014 to investigate outcomes of cholecystectomy among hospitalized adults with CF compared to controls without CF.A propensity weighted sample was selected that closely matched patient demographics,patient’s individual comorbidities,and hospital characteristics.The propensity weighted sample was used to compare outcomes among patients who underwent laparoscopic cholecystectomy.Hospital outcomes of open and laparoscopic cholecystectomy were compared among adults with CF.RESULTS A total of 1239 inpatient cholecystectomies were performed in patients with CF,of which 78.6% were performed laparoscopically.Mortality was <0.81%,similar to those without CF (P=0.719).In the propensity weighted analysis of laparoscopic cholecystectomy,there was no difference in mortality,or pulmonary or surgical complications between patients with CF and controls.After adjusting for significant covariates among patients with CF,open cholecystectomy was independently associated with a 4.8 d longer length of stay (P=0.018) and an$18449 increase in hospital costs (P=0.005) compared to laparoscopic cholecystectomy.CONCLUSION Patients with CF have a very low mortality after cholecystectomy that is similar to the general population.Among patients with CF,laparoscopic approach reduces resource utilization and minimizes post-operative complications.
Key Words:Laparoscopic cholecystectomy;Nationwide Inpatient Sample;Cystic fibrosis;Mortality;Length of stay;Symptomatic biliary disorders
INTRODUCTION
Cystic fibrosis (CF) is a multisystem disease resulting from defects in the CF transmembrane conductance regulator (CFTR) apparatus.The highest incidence of CF is seen in people of northern European descent,where CF occurs in one out of 3000 live births and approximately one in 25 people carry a pathogenic allele[1].When initially described in the 1930s,median survival was only a few months but advances in pulmonary treatments have since increased the median predicted survival beyond 40 years[2,3].While the natural history and treatment of pulmonary and pancreatic diseases in CF have been well characterized,other affected organs,such as the biliary tree and gallbladder,have less epidemiologic and clinical data to guide care.Management of these other organ systems which affect quality of life will become increasingly important as median survival improves.
Biliary disorders are thought to be common in CF due to the high expression of the CFTR gene in the gallbladder and biliary tree[4].The mechanism of gallstone formation in CF is incompletely understood,but is likely the result of biliary stasis due to gallbladder dysmotility and prolonged transit through the bile ducts[4,5].Cholelithiasis is reported in 20%-30% of patients with CF,and symptomatic biliary colic is experienced by 4% to 40% of subjects in retrospective studies[6-8].One case series suggested that the incidence of cholelithiasis increases with age,from 0.1% in those less than 5 years of age,to nearly 10% in those aged 30-40[8].Additionally,the use of CF transmembrane conductance regulator (CFTR) modulators may increase the risk of biliary colic[9].The population of patients with CF are aging and CFTR modulators are increasingly used,which are leading to a greater number of patients at risk for biliary and gallbladder disorders.
In patients without CF,symptomatic biliary disorders are managed surgically by cholecystectomy.However,few CF patients undergo cholecystectomy,due at least in part to concerns for perioperative complications[3,10].The few published case series of cholecystectomy show an aggregate mortality rate of 4% (3/71) among patients with CF,which is considerably higher than the 0.15% mortality reported in the general population[6,8,10-15].However,the CF surgical case series were completed over 25 years ago,and surgical technique and patient characteristics have changed dramatically since then.We hypothesized that the outcomes of cholecystectomy in a modern cohort of subjects with CF will be no different than the general population,especially when controlling for comorbidities.We aimed to evaluate the safety of cholecystectomy in subjects with CF compared to non-CF controls using a large national database.
MATERIALS AND METHODS
Data source
A retrospective analysis was performed using the Nationwide Inpatient Sample (NIS)(2002 to 2014),available through the Healthcare Cost and Utilization Project (HCUP)of the Agency for Healthcare Research and Quality.The NIS represents more than 35 million individual hospitalizations annually across the United States and is one of the largest publicly available databases.This database can be used to evaluate patient and hospital characteristics as well as resource utilization such as costs,mortality,and length of stay[16].As the NIS is a publicly available database of de-identified patients,The Ohio State University Institutional Review Board deemed studies utilizing this resource as exempt.
Study sample
Subjects were required to have a procedure code for cholecystectomy,defined as open,laparoscopic,or laparoscopic converted to open (Supplementary Table 1).Subjects were excluded if they were under the age of 18,pregnant,had cirrhosis,or underwent a partial cholecystectomy.Patients who underwent laparoscopic converted to open approach were categorized as open cholecystectomy.The cohorts were then defined by the presence or absence of CF diagnosis codes.
Outcomes of interest
The primary outcome of interest was mortality following cholecystectomy.As secondary outcomes,we evaluated length of stay,cost of hospitalization,and the rates of post-operative complications based on a validated set of diagnosis and procedure codes (Supplementary Table 1)[17,18].Additionally,we analyzed the indications for cholecystectomy among patients with CF using previously defined diagnosis codes(Supplementary Table 1)[19-21].Patients with choledocholithiasis and gallstone pancreatitis were included in the category of gallstone disease without cholecystitis(Supplementary Table 1).All outcomes were compared between patients with and without CF using survey weighting and propensity weighting and between patients with CF who received open or laparoscopic cholecystectomy using univariate and multivariate analyses.A study flowchart of patient inclusion and analyses is presented in Figure 1.
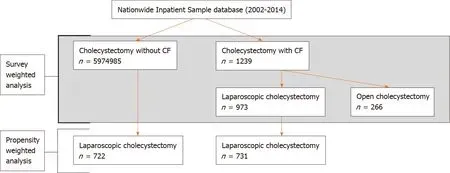
Figure 1 Study flowchart demonstrating survey weighted and propensity weighted analyses.
Definition of variables
Other variables evaluated include age,gender,race,income,type of insurance,hospital size,type of hospital,and hospital region.The presence of comorbid conditions were evaluated using the Elixhauser comorbidity index,which has been used widely since it was developed in 2005[22].
Statistical analysis
All analyses were performed using SAS version 9.4 (SAS Institute,Cary,NC,United States) on weighted data and accounted for the complex survey designs of the NIS.Differences between patient characteristics,hospital characteristics,and outcomes were compared between patients with and without CF through the use of chi-square tests for categorical variables andt-tests for continuous variables.Similar comparisons were made between the populations of patients with CF who underwent open or laparoscopic cholecystectomy.Multivariate linear regression models were created for length of stay and hospital costs using a stepwise selection process.Where less than 10 observations are recorded,the exact number is censored to protect subject privacy,per NIS regulations.Missing data is listed in Supplementary Table 2.
Propensity weighted analysis
Among patients who underwent a laparoscopic cholecystectomy,propensity scores were calculated using a multivariable logistic regression model for CF containing all patient and hospital characteristics and indications for cholecystectomy as well as all individual Elixhauser comorbidities.The logistic regression model was weighted and accounted for all aspects of the complex survey design.
After deriving propensity scores (e) for each subject,propensity score weights were defined as 1 for subjects with CF and ase/(1-e) for subjects without CF.These propensity score weights were then multiplied by the original survey weights defined by HCUP to arrive at the new weights which were used in place of the original HCUP weights in the following propensity weighted analysis,as previously described[23].After propensity weighting was applied,all variables were well balanced between the two groups.The propensity weights were then used to evaluate differences in outcomes between patients with and without CF.
RESULTS
Demographics
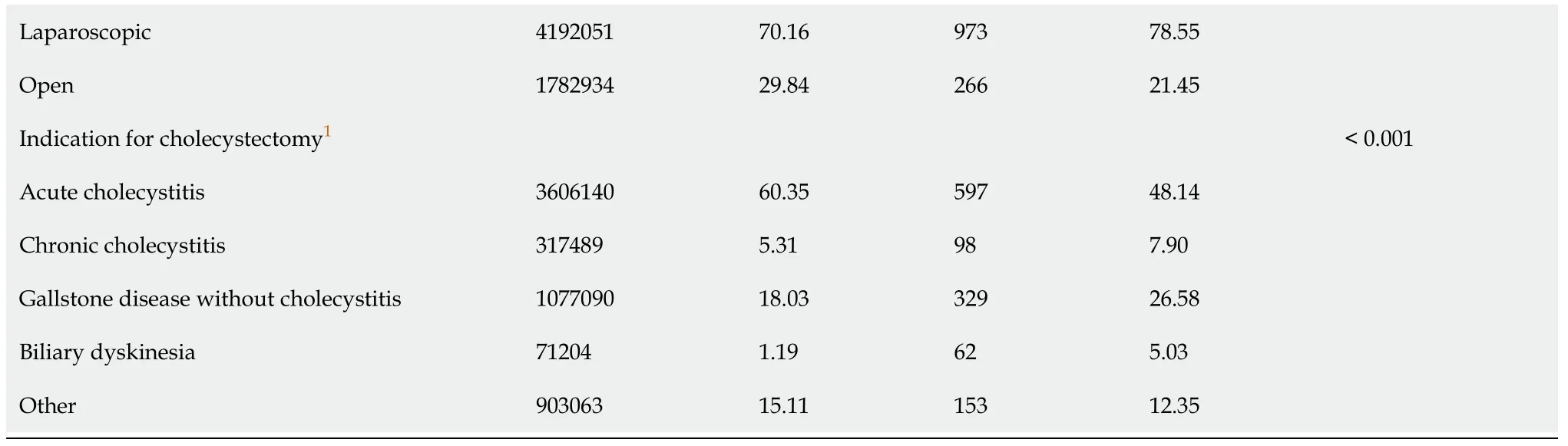
From 2002 to 2014,a total of 5976224 adults underwent inpatient cholecystectomy,of which 1239 (0.021%) had CF (Table 1,Figure 1).Subjects with CF were younger and were more likely to be white,have private insurance,be treated at an urban teaching hospital,and have comorbid chronic respiratory failure (Table 1).A laparoscopic approach was used more often in CF subjects than in controls (78.6%vs70.2%,P=0.003) (Table 1).The indications for surgery between these groups were different:subjects with CF were less likely to undergo cholecystectomy for acute cholecystitis(48.1%vs60.4%,P<0.001),but more likely to have gallstone disease without cholecystitis (26.6%vs18.0%,P<0.001) or biliary dyskinesia (5.0%vs1.2%,P<0.001)(Table 1).Mortality was not significantly different between those with CF and those without (≤ 0.81%vs0.99%,P=0.719) (Supplementary Table 3).Length of stay and total hospitalization costs were higher for CF patients than controls (10.1 dvs5.4 d,P<0.001;$27561vs$14059,P<0.001) (Supplementary Table 3).
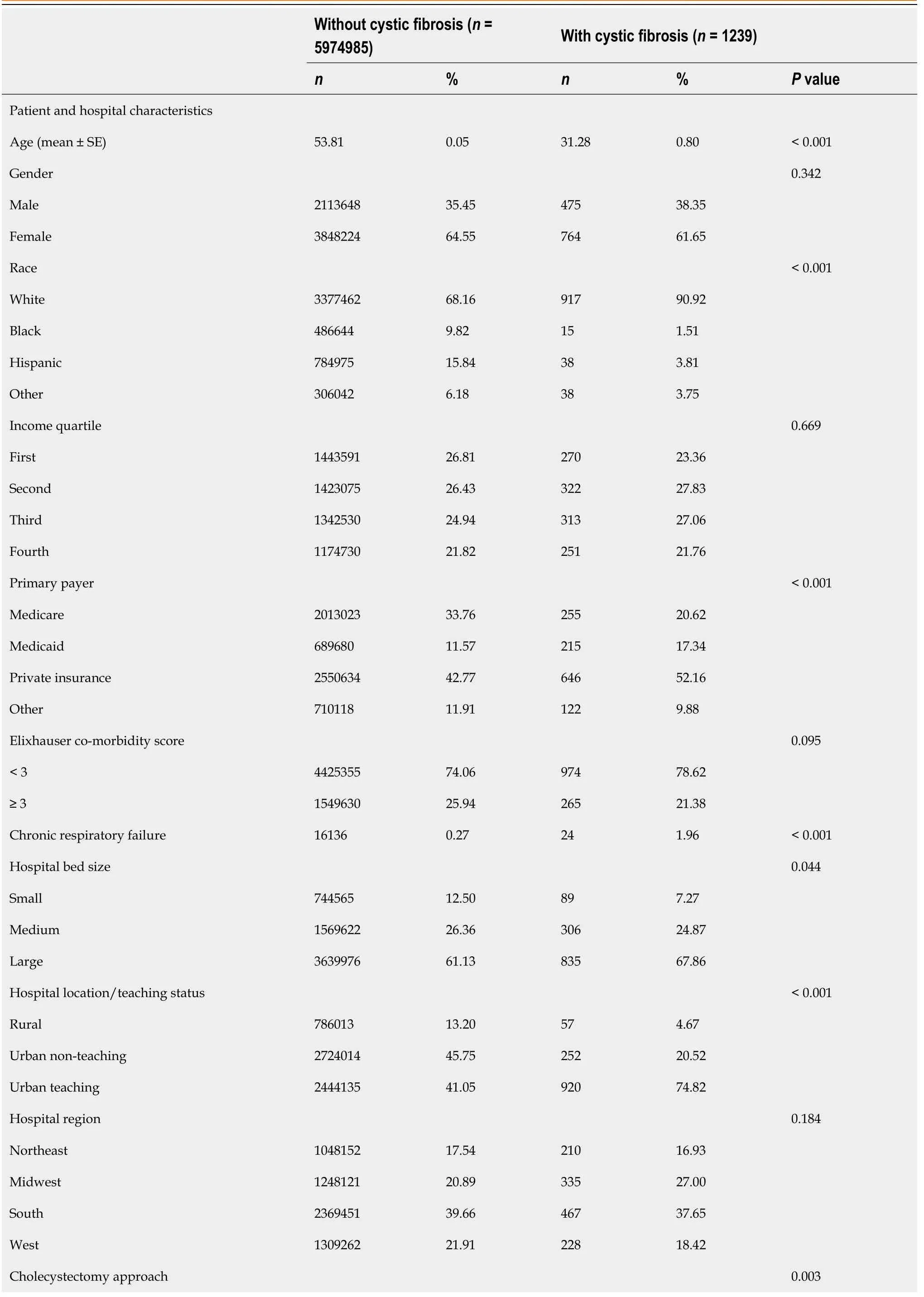
Table 1 Comparison of characteristics between subjects with and without cystic fibrosis who underwent cholecystectomy from 2002 to 2014
Propensity weighted analysis
1Hierarchy model.
After propensity weighting was applied to patients who underwent laparoscopic cholecystectomy,the variables were well balanced between groups(Supplementary Table 4).Hospital mortality was low among both groups,with less than 10 events observed (Table 2).Subjects with CF experienced a mean length of stay(LOS) of 9.4 d,compared to 5.2 d in those without CF (P<0.001) (Table 2).Similarly,total hospital costs were greater for subjects with CF ($25891vs$14103,P=0.003)(Table 2).There was no difference between CF and controls in post-operative surgical complications (4.5%vs2.3%,P=0.094) or pulmonary complications (6.6%vs4.1%,P=0.109) (Table 2).

Table 2 Univariate analysis of outcomes between propensity weighted cohort of patients with and without cystic fibrosis who underwent laparoscopic cholecystectomy in the Nationwide Inpatient Sample 2002-2014
Impact of surgical route on outcomes in CF
Of the 1239 patients with CF who underwent cholecystectomy,973 (78.6%) had a laparoscopic approach.Compared to an open approach,patients with a laparoscopic cholecystectomy were more likely to be female,but other demographics were similar(Table 3).There was no significant difference in mortality (≤ 1.0%vs≤ 3.8%,P=0.286)but the LOS was longer and total hospital costs were greater in the open cholecystectomy group (14.5 dvs8.9 d,P=0.009;$43024vs$23288,P=0.005)(Supplementary Table 4).After adjusting for significant covariates,open route at surgery was associated with longer LOS (4.82 d,95%CI:0.82 d,8.83 d,P=0.018) and increased hospital costs ($18449,95%CI:$5582,$31316,P=0.005) (Table 4 and Supplementary Table 5).There were insufficient observations of mortality and postoperative complications to fit a multivariate model for these outcomes.
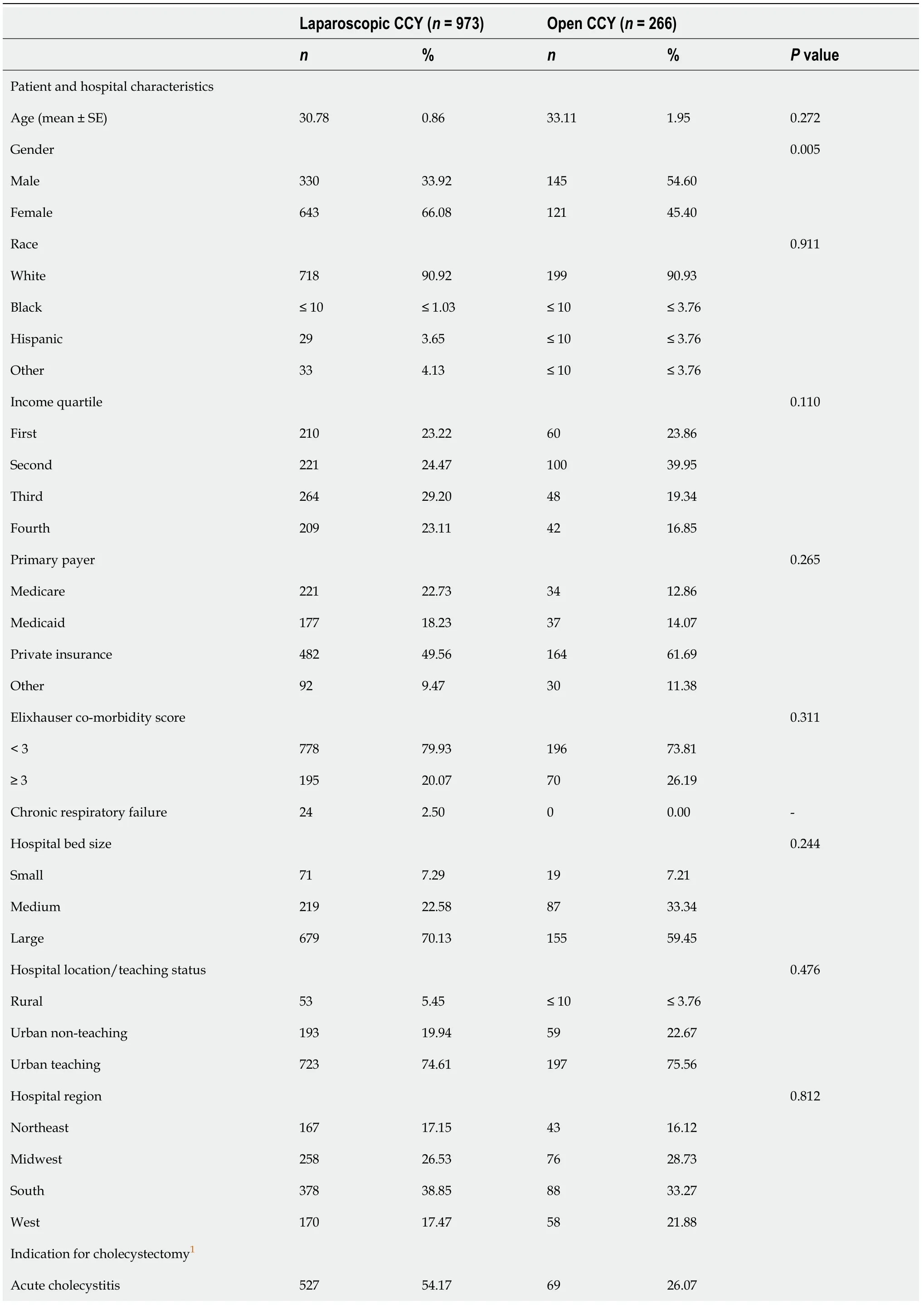
Table 3 Comparison of characteristics between subjects with cystic fibrosis who underwent open compared to laparoscopic cholecystectomy from 2002 to 2014

1Hierarchy model.2Where n ≤ 10,the exact value is censored to protect patient privacy,per Nationwide Inpatient Sample regulation.CCY:Cholecystectomy.

Table 4 Multivariate comparison of post-operative outcomes between subjects with cystic fibrosis who underwent open compared to laparoscopic cholecystectomy from 2002 to 2014
DISCUSSION
More patients with CF are reaching adulthood due to advances in CF care and CFTR modulators are increasingly used.With this,clinicians are likely to see an increasing prevalence of biliary disorders for which cholecystectomy will be considered as a definitive treatment.Therefore,it is important to clarify the safety of cholecystectomy.In this study,we used a nationally-representative database to evaluate the postoperative outcomes among adult patients with CF who undergo cholecystectomy.Importantly,we found that cholecystectomy had very low in-hospital mortality that was not significantly different from the general population.The surgical indications and approach were different between patients with and without CF.Open cholecystectomy was independently associated with longer LOS and greater hospital costs compared to laparoscopic approach.Finally,there is increased healthcare utilization among patients with CF compared to a propensity weighted cohort following laparoscopic cholecystectomy.
Our data shows a low mortality rate in a large and nationally representative cohort of CF patients,comparable to previous case series of cholecystectomy among CF patients.Aggregate data from case series show no deaths out of 12 patients who underwent laparoscopic surgery and 3/59 (5.1%) who underwent open cholecystectomy (although many of these surgeries were performed over 25 years ago)[6,8,10-12,15].The previous case series also reported long lengths of stay after open cholecystectomy,up to 22 d in one series,partially due to prolonged pre- and postoperative intravenous antibiotics and frequent respiratory care[12].Compared to these older studies,the current mean length of stay for laparoscopic cholecystectomy (8.9 d,standard error 0.71 d) is shorter.Similarly,CF patients experience longer LOS after sinus surgery compared to non-CF patients[24].In one study using the American College of Surgeons’ National Surgical Quality Improvement Program-Pediatric database,the authors suggested that the longer LOS was not due to complications but rather due to extended monitoring and intravenous antibiotics[24].Our study shows this also appears to be true for cholecystectomy:Patients with CF have longer LOS than controls despite similar rates of post-operative complications.
Post-operative pulmonary decompensation and infection has been reported in previous case series,with an overall incidence of 7.0% (5/71) that is similar to our study[6,8,10-13,15].To mitigate this risk,chest physiotherapy and antibiotics were used pre- and post-operatively.One group targeted pre-operative pulmonary function tests at the “highest level attained in the past 2 years,or until a prolonged period of therapy reaches a plateau of improvement” for elective surgery[10].Increased pulmonary complications after open cholecystectomy may be attributed to derangements in respiratory mechanics due to the surgical incision near the diaphragm and increased post-operative pain[25].Accordingly,laparoscopic cholecystectomy is recommended over open cholecystectomy for subjects with chronic pulmonary comorbidities to minimize risks of post-operative complications[25,26].These data suggest that optimal outcomes are attained by elective laparoscopic intervention,and further study may be required to determine the best approach for pre- and postoperative pulmonary optimization among patients with CF.
While the incidence of post-cholecystectomy pulmonary complications has been described,the risk of surgical complications including soft tissue infections,perforation during surgery and need for recurrent surgery in CF compared to the general population has not been previously reported.We demonstrate an increased risk of surgical complications in patients with CF compared to the general population in the survey weighted cohort,and an increased risk with open compared to laparoscopic cholecystectomy among patients with CF.In the propensity weighted analysis,we found no significant difference in the rate of surgical complications.Patients with CF have an increased risk of infections with drug resistant bacteria,which may place this population at higher risk of infection after surgical intervention as these organisms may not be treated by routine pre-operative antibiotics[27].
Our study has several limitations inherent to the use of a large database,such as the potential for coding errors.Additionally,we cannot account for characteristics that are not included in the NIS which may influence outcomes,such as medication use,nutritional status,and baseline pulmonary function,nor can we evaluate survival beyond the inpatient period.Lastly,there may be selection bias,as only patients with acceptable surgical risk would have undergone cholecystectomy.Due to these limitations,“causality” cannot be inferred from large database analyses.However,in the absence of a prospectively collected surgical registry among patients with CF,the NIS remains an excellent data source due to its large number of observations and sophisticated sampling design.The NIS included 1239 inpatient cholecystectomies among patients with CF which greatly outnumbers the 71 cases reported in the literature to date.Additionally the NIS represents national demographics so the reported outcomes are likely to be generalizable to similar CF patients encountered in clinical practice.Finally,the volume of cholecystectomy in the control population allowed for a propensity weighted analysis to approximate a randomized trial,which could not be reasonably accomplished outside of a large database.
CONCLUSION
Cholecystectomy among adult patients with CF did not carry an increased risk of inhospital mortality compared to controls.Length of stay and hospital costs are higher in patients with CF and there is a higher risk of post-operative surgical complications and a tendency to develop more pulmonary complications,although this risk of complications is no longer seen when demographic and health variables are taken into account.A laparoscopic approach is safer and reduces healthcare utilization compared to an open approach in adults with CF.These results should inform the discussion between clinicians and patients with CF when cholecystectomy is considered.
ARTICLE HIGHLIGHTS
Research background
Symptomatic biliary disorders are common in cystic fibrosis (CF) and may become more common now that patients with CF are living longer.Biliary disorders are often managed with cholecystectomy but this surgery carries high risk of morbidity and mortality among adults with CF.However,the reported rate of complications is based on older studies,and may not represent modern surgical outcomes.
Research motivation
Currently,there is insufficient data examining the safety of cholecystectomy among adults with CF using modern surgical techniques.
Research objectives
To investigate the outcomes of inpatient cholecystectomy among adults with and without CF.
Research methods
The Nationwide Inpatient Sample was used to collect data on inpatient cholecystectomies between 2002 and 2014.Subjects without CF were matched 1:1 to subjects with CF,accounting for over 20 variables including age,sex,and comorbidities.
Research results
Among patients with CF,1239 cholecystectomies were performed during the study period.Open cholecystectomy was independently associated with an $18449 increase in hospital costs (P=0.005) and a 4.8 d longer length of stay (P=0.018) compared to laparoscopic cholecystectomy.The mortality rate among patients with CF was <0.81%,which was similar to the mortality rate among patients without CF (P=0.719).Similarly,there was no significant difference in mortality or post-operative surgical complications (4.5%vs2.3%,P=0.094) or pulmonary complications (6.6%vs4.1%,P=0.109) after laparoscopic cholecystectomy between patients with and without CF in the propensity weighted analysis.
Research conclusions
With modern anesthesia and surgical techniques,cholecystectomy is equally safe for patients with and without CF.
Research perspectives
Cholecystectomy may be increasingly considered for the management of biliary symptoms among adults with CF.Future research will need to clarify if there are unique indications for cholecystectomy among patients with CF.
 World Journal of Gastrointestinal Endoscopy2021年9期
World Journal of Gastrointestinal Endoscopy2021年9期
- World Journal of Gastrointestinal Endoscopy的其它文章
- Ectopic pancreas at the ampulla of Vater diagnosed with endoscopic snare papillectomy:A case report and review of literature
- Endoscopic treatment of periampullary duodenal duplication cysts in children:Case series and literature review
- Enlarged folds on endoscopic gastritis as a predictor for submucosal invasion of gastric cancers
- COVID-19 in the endoscopy unit:How likely is transmission of infection? Results from an international,multicenter study
- Clinical characteristics and prognosis of patients with ulcerative colitis that shows rectal sparing at initial diagnosis
- Gastrointestinal hemorrhage in the setting of gastrointestinal cancer:Anatomical prevalence,predictors,and interventions