
Effect of trabeculated myocardial mass on left ventricle global and regional functions in noncompaction cardiomyopathy
2021-07-31 01:36:28GulsahYildirimMemduhDursunfatArslan
World Journal of Cardiology 2021年7期
Gulsah Yildirim,Memduh Dursun,Rıfat Arslan
Gulsah Yildirim,Department of Radiology,University of Health Sciences,Istanbul Fatih Sultan Mehmet Training and Research Hospital,İstanbul 34752,Turkey
Memduh Dursun,Department of Radiology,İstanbul University School of Medicine,İstanbul 34752,Turkey
Rıfat Arslan,Department of Radiology,Istanbul University,Istanbul Faculty of Medicine,İstanbul 34752,Turkey
Abstract BACKGROUND Left ventricular (LV) noncompaction cardiomyopathy is a rare cardiomyopathic subtype that has been recognized in recent years and is being diagnosed at an increased rate.There is no consensus regarding the diagnosis of the disease,and increased trabeculation rates that meet the existing diagnostic criteria may even be present in healthy asymptomatic people.This indicates that differentiating criteria for diagnosis are needed.AIM To examine the increase in myocardial trabeculation and the change in left ventricular global and regional functions.METHODS This retrospective study included 65 patients (28 females,37 males) diagnosed with LV noncompaction cardiomyopathy who underwent cardiac magnetic resonance imaging between January 2011 and August 2016 and had a noncompacted/compacted myocardial thickness ratio of over 2.3 in more than one segment in the left ventricle.The distribution and ratios of trabeculations in apical,midventricular,and basal regions were examined in short-axis images obtained from cardiac magnetic resonance.In addition,by using short-axis cine images,regional ejection fraction (EF) and global EF were calculated using the Simpson method in the left ventricle at apical,basal,and midventricular levels.RESULTS While the number of trabeculated segments were similar at the apical (3.2±1.0)and midventricular levels,a statistically significant level of involvement was not observed at the basal level (0.4±0.9) (P>0.05).The highest noncompacted/compacted (trabeculation) ratio was observed at the apical level (3.9±1.4),while this ratio was higher at the anterior (59%-89.4%) and lateral (62%-84.8%) segments (P>0.05).Global EF was positively correlated with apical,midventricular,and basal regional EF (P<0.05).However,there was no significant correlation between regional EF and the number of trabeculated segments or trabeculation ratio in all three regions;nor was there a significant correlation between regional EF and the number of trabeculated segments or trabeculation ratio in the entire LV (P>0.05).CONCLUSION No global or regional relationship was observed between LV dysfunction and trabeculation rate or the number of trabeculated segments.This limits the usefulness of change in LV functions in the differentiation between normal and pathological trabeculation.
Key Words:Isolated noncompaction of the ventricular myocardium;Cardiomyopathies;Magnetic resonance imaging;Stroke volume;Magnetic resonance imaging;Ventricular function
INTRODUCTION
Left ventricular noncompaction cardiomyopathy (LVNC) is a form of cardiomyopathy that has been classified as primary genetic cardiomyopathy by the World Health Organization since 2006[1,2].It is characterized by phenotypically prominent trabeculations,deep intertrabecular recesses,and thick noncompacted endocardium vs thin compacted epicardium.Etiologic factors of the disease are not fully clear.Genetic transmission may occur in sporadic or familial forms[3,4].Several hypotheses have been prepared to explain the development mechanism of LVNC.However,there is a consensus of ideas that the left ventricle is the result of abnormal morphogenesis.In the 8thwk of gestation,myocardial trabeculations begin to be compacted starting from the basal region of the heart (compaction:Compacting of the trabeculations)[5].Ventricular compaction advances from the epicardium towards the endocardium,from the base of the heart towards the apex and from the septum towards the free wall[6].In the fetal heart,ventricular myocardial compaction is completed in the 4thmo.If the compaction process is interrupted,non-compaction cardiomyopathy occurs and the clinical manifestation varies depending on the stage of interruption.In addition,autopsy studies have shown that prominent trabeculations arising from the embryonal development process can also be found in high rates in the hearts of normal people and can be observed in the apex[7-9].
The actual prevalence of non-compaction cardiomyopathy is not fully known;however,one single-study in the literature reported that it varies between 0.014%-1.3%[10].The most important diagnostic parameter is the ratio of non-compacted layer in relation to compacted layers of myocardium;this ratio should be over 2 in echocardiography and over 2.3 in cardiac magnetic resonance (CMR) imaging[11,12].Different criteria have been proposed for diagnosis,the most important of which is to decide whether the trabeculations observed in imaging are normal,a normal variant,or pathological.The existing diagnostic criteria based on echocardiographic and CMR findings have certain limitations[13].Recent studies have shown that increased trabeculation ratios may also be present in healthy asymptomatic individuals,leading to increased rates of LVNC diagnosis and indicating that new diagnostic criteria are needed.In addition,LVNC may be complicated by heart failure and result in cardiac transplantation,while the existing diagnostic criteria cannot determine or predict this process[6,14].
In this retrospective study,we aimed to investigate the effect of increased myocardial trabeculation on left ventricular global and ejection fraction (EF).In this regard,changes in EF can be included among the diagnostic criteria of the disease,preventing misdiagnosis,and can be used in the follow-up of the disease.
MATERIALS AND METHODS
Patient population
A total of 65 patients between ages 18-65 who were diagnosed with LVNC and referred to our department between January 2011 and August 2016 were included in our study.Patients were diagnosed by experienced cardiologists according to Jenni echocardiographic criteria.In the retrospective evaluations,the most important inclusion criteria independent from age and gender was CMR noncompacted/compacted myocardium ratio (NC/C) of 2.3 or higher.Exclusion criteria were as follows:Presence of contraindications for CMR,presence of other cardiomyopathies and congenital or non-congenital heart disease,and history of neuromuscular disease.
CMR protocol
The cardiac magnetic resonance imaging (MRI) protocol for LVNC in our clinic was applied to the patient group.Imaging was conducted in supine position with a 1.5 Tesla (Philips Achieva;Philips Medical Systems,Amsterdam,Netherlands) MRI device.The SENSE-XL-Torso cardiac coil was placed on the anterior chest wall,and a signal acquisition system using electrocardiogram and respiratory trigger was applied.Initially,cardiac survey imaging was performed for the coronal,axial,and sagittal planes with Single Shot Balanced transcription factor E sequence.From the survey images,the plane formed between the mitral valve and apex in the axial plane and long axis two-chamber cine images from the Balanced transcription factor E sequence were obtained.Long axis four-chamber cine and short-axis (SA) cine images were obtained from these images.Since equal breath-hold is important for image quality,patients were asked to hold their breath at the end of expiration.
Imaging analysis
Cardiac MRI images were retrospectively evaluated by two radiologist who were experienced with cardiac images together using the standard approach on a Philips workstation.In the analyses,first the segment’s non-trabeculated segment ratio was measured according to the American Heart Association’s 16-segment model based on the ratio of trabeculated segment to non-trabeculated segment in the left ventricle (LV)at end-diastole[15].Segments above the 2.3 cutoff value in all three SA planes (apical,mid,and basal),and the segment with the highest ratio in each axis was determined when making measurements.When distinguishing segmentation,the papillary muscle level was specified for the midventricular segment,the superior of the papillary muscles for the basal segment,and inferior of the papillary muscles as the apical segment.When determining the basal regions,the short axis section where more than half of the lumen was surrounded by myocardium was chosen.According to the current protocol,trabeculations were determined as regions with muscular structure moving together with the inner myocardium border,extending towards the cardiac region,and not accompanying the papillary muscles at the end of systole.The border between compacted and trabeculated myocardium in each segment was chosen outside of the line where trabeculation was not prominent (Figure 1).In the second step,systolic function analysis was performed separately for all three axes and globally for the entire LV.Simpson method was used for analysis.In the calculation of EF values,diastole and end-systolic endocardial boundaries were drawn manually for all three axes in short axis images,and finally,global EF values were calculated by drawing systole and end-diastolic endocardial boundaries in all sections from the apex to the base.The narrowest and widest ventricular cavity size was used at the midventricular region to determine the systole and end-diastolic phases,respectively.Endocardial boundaries were drawn using the difference between the hyperintensity of the blood-filled cavity and the moderate intensity of the myocardium[16].Papillary muscles were included in the ventricular cavity since they did not affect mass and cavity volume change in EF measurements.
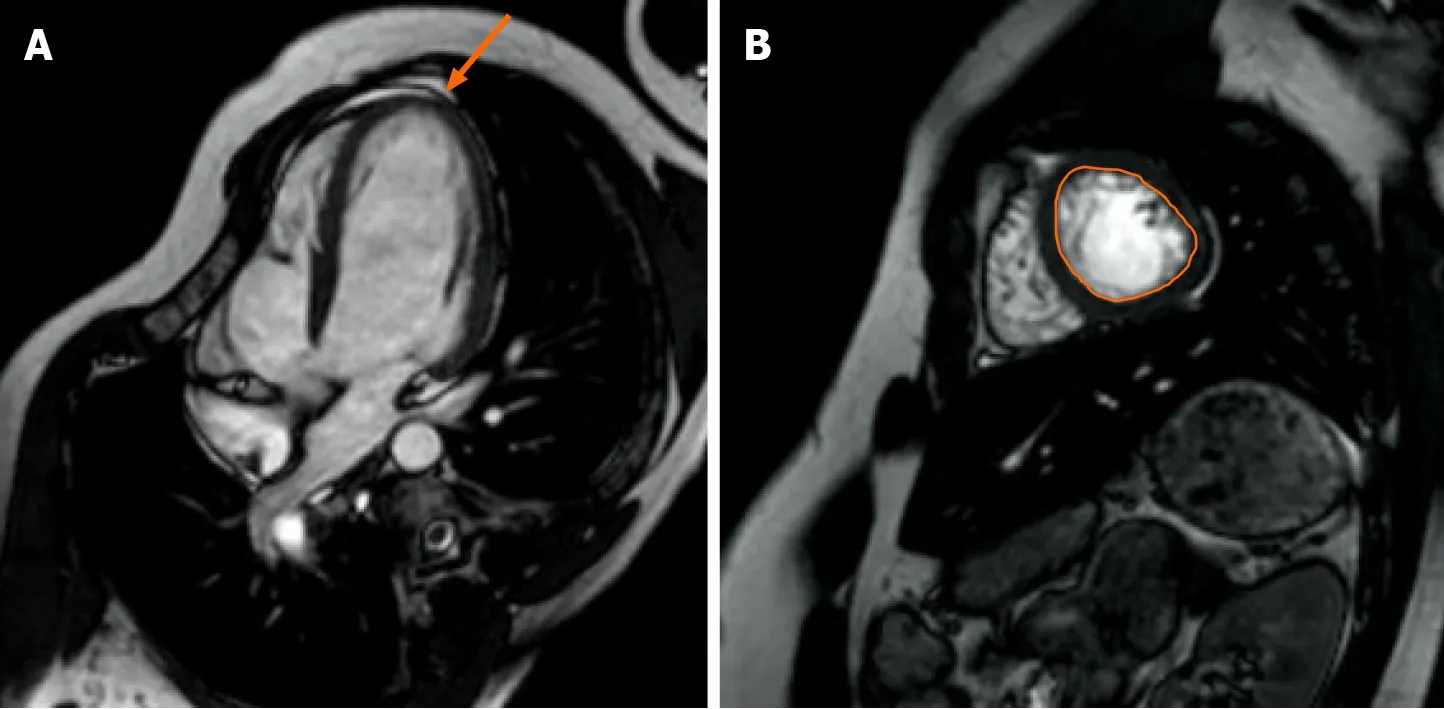
Figure 1 Cardiac magnetic resonance imaging appearance of left ventricular non-compaction.
Statistical analysis
Statistical analyses were performed using the SPSS 22.0 package program (Armonk,NY,United States).Mean,standard deviation,median,lowest-highest frequency,and percentage values were used in the descriptive statistics of the data.The distribution of variables was measured with the Kolmogorov-Smirnov test.Mann-Whitney U test was used in the analysis of quantitative independent data.Chi-square test was used to analyze qualitative independent data,and Fischer’s exact test was used when Chisquare test conditions were not met.Spearman’s rank correlation coefficient was used for correlation analysis.
RESULTS
We reviewed the electronic medical records and the baseline clinical characteristics,and cardiovascular compliments (congestive heart failure,syncope,embolic events,and any arrhythmias) of the patient population are summarized in Table 1.Also,in the study group none of the patients had diabetes mellitus and dyslipidemia.However,5 patients had hypertension.
All patients who were included in the study met echocardiographic and CMR diagnostic criteria.All 65 patients had trabeculation ratio over 2.3 in at least three segments and at least two regions (apical,midventricular,basal).The number of trabeculated segments were high and similar at apical (3±1) and midventricular (3±1.4) regions,while there was no statistically significant involvement in basal regions.According to segmental distribution,trabeculation was most frequently observed in the apical-lateral (93.9%) and apical-anterior (89.4%) segments (P<0.001).The highest trabeculation ratio was seen in the apical region (3.6±1.4) (Tables 2 and 3).
There was a positive correlation between global EF and apical,midventricular,and basal EFs (P<0.05).In addition,there was a positive correlation between the EFs of all three regions (P<0.05) (Figure 2).

Figure 2 Comparison of left ventricular global function and regional (apical,midventricular,basal) functions.
There was no correlation between global EF and total number of segments involved and highest trabeculation rates for all three apical,midventricular,and basal regions (P>0.05).No correlation was found between the regional EF values of the apical,midventricular,and basal regions and the number of trabeculated segments and the highest trabeculation ratio in these regions (P>0.05) (Tables 4 and 5).
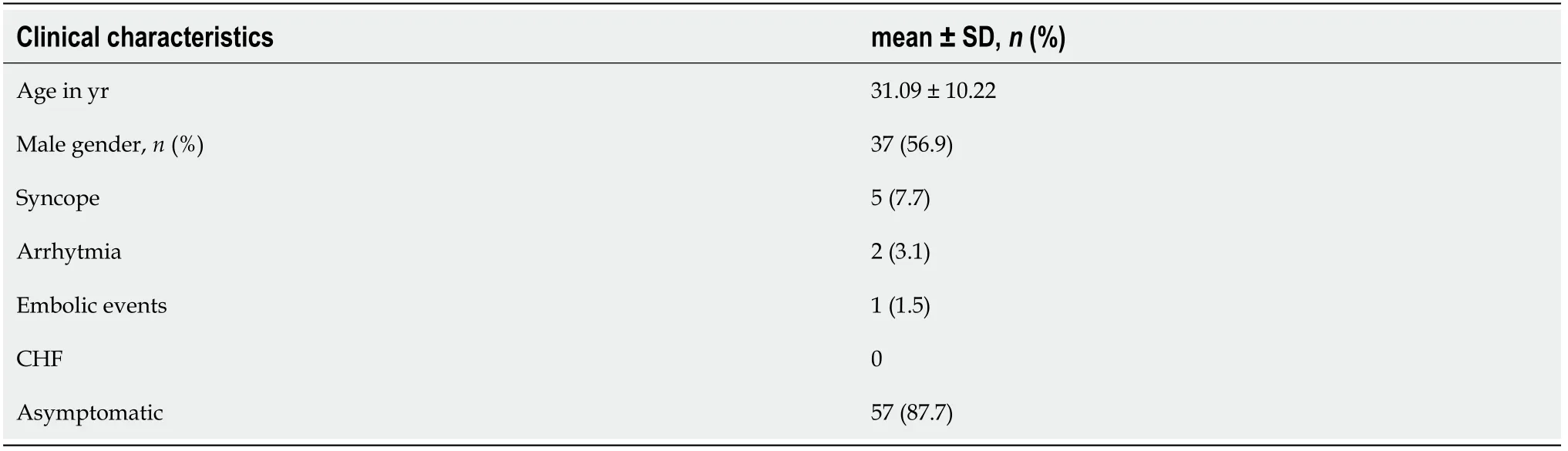
Table 1 Clinical characteristics of the study population
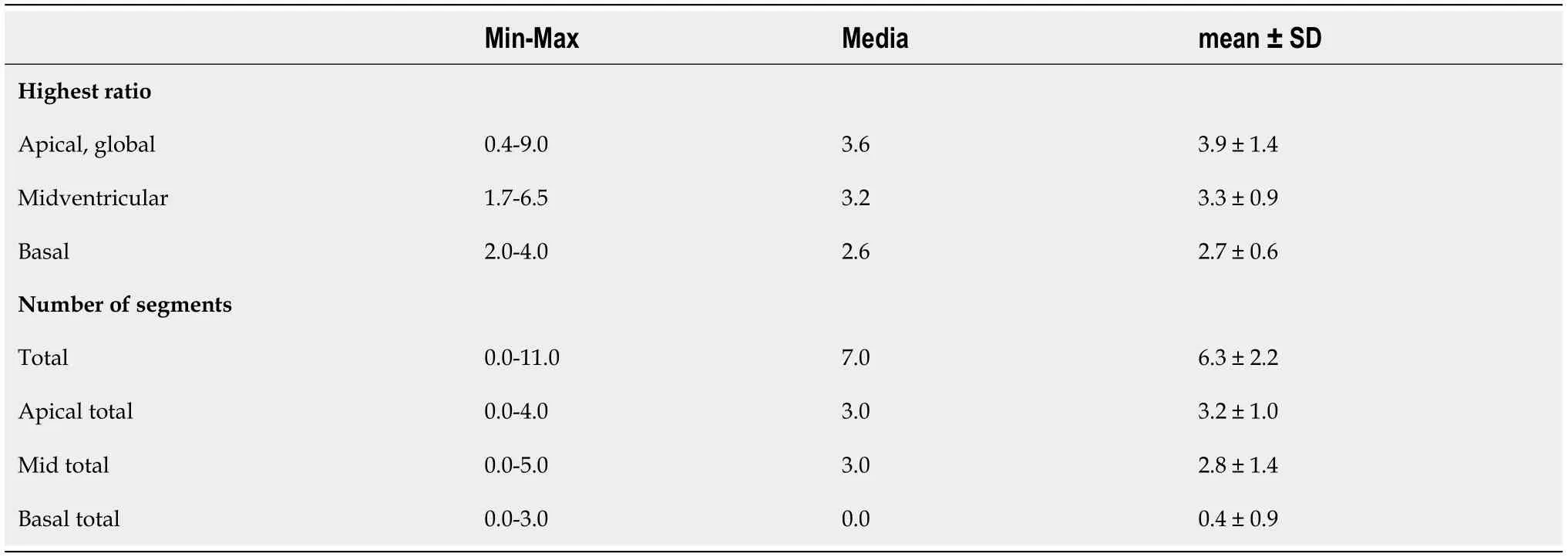
Table 2 The highest values of the trabeculation ratio for apical,midventricular,basal regions,and global left ventricle and the distribution of the total number of trabeculated segments

Table 3 Segmental distribution of trabeculations in the apical,midventricular,and basal regions of the left ventricle
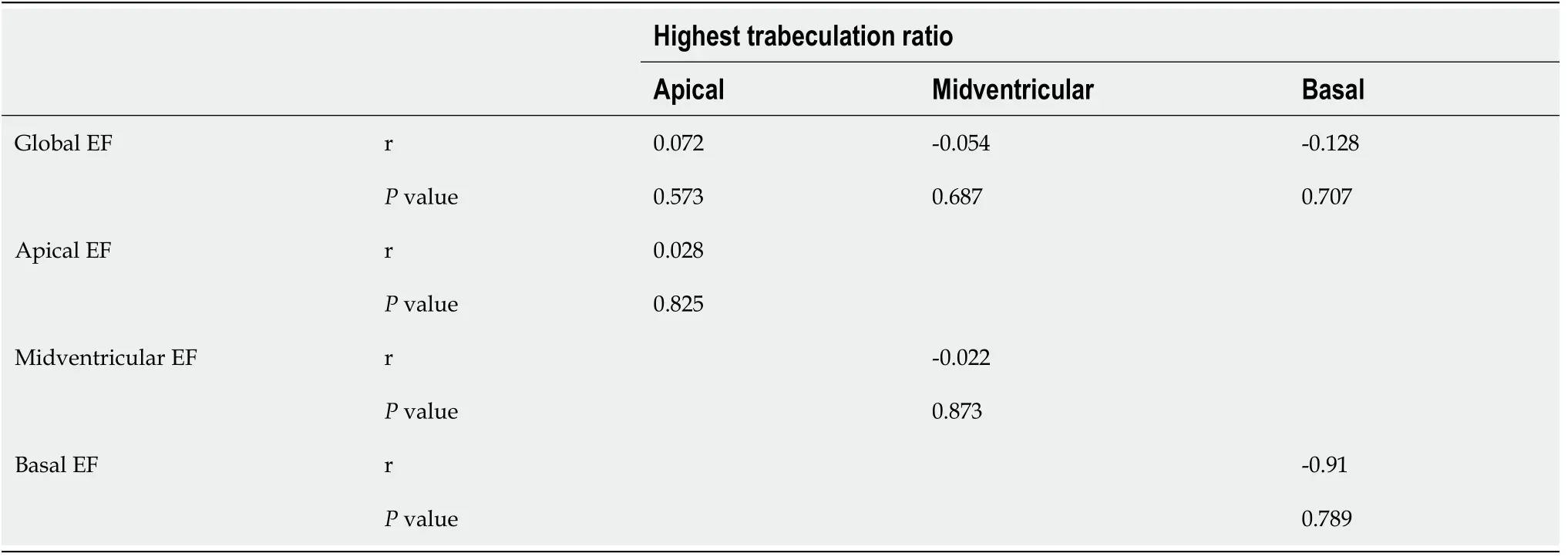
Table 4 Comparison of highest trabeculation ratio and ejection fraction in global and regional left ventricular function
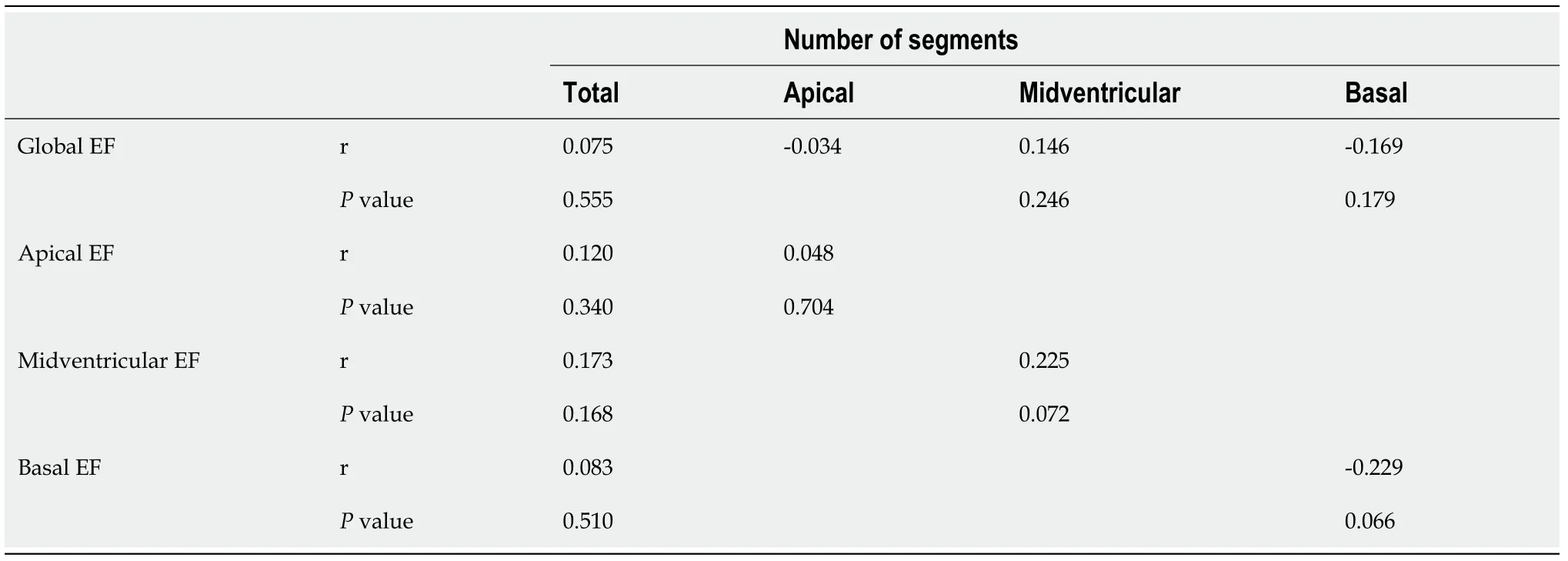
Table 5 Comparison of global and regional (apical,midventricular,and basal) number of trabeculated segments and ejection fraction in left ventricular function
DISCUSSION
Noncompaction cardiomyopathy is a form of cardiomyopathy characterized by a bilayered compacted and noncompacted myocardium model with prominent myocardial trabeculations and intertrabecular recesses[17].While it may be isolated,it may also be accompanied by multiple cardiac malformations[18].Although there is no consensus regarding the etiopathogenesis of the disease,genetic studies have identified certain sarcomeric and non-sarcomeric cardiomyopathy genes[19,20].Usually,the LV is affected alone[21].While clinical presentation may occur at all ages,it usually manifests in childhood[19].The disease may be asymptomatic,or symptoms may vary depending on the severity of involvement,symptoms of the accompanying syndrome,and congenital heart diseases[18].In the literature,the most common clinical findings related to LVNC include heart failure,arrhythmias,and systemic embolic events[18].The compaction process in the fetal heart occurs from the epicardium towards the endocardium,from the base of the heart towards the apex,and from the septum towards the lateral,and severity of the phenotype varies depending on the time of interruption[21].In our study,trabeculations were observed more commonly in the apical and midventricular regions,consistent with the fetal compaction process.
In order to diagnose LVNC,the main defined structural features must be revealed with imaging.The most important parameter in diagnosis is the ratio of the noncompacted layer to the compacted layers.This ratio must be more than 2 in echocardiography,and more than 2.3 in CMR.Echocardiography and CMR are the main imaging modalities used to diagnose the disease.Echocardiography is widely used due to its availability,common use,low cost,and absence of radiation exposure[22].Chinet al[11] initially proposed evaluating the ratio of X to Y for echocardiographic diagnosis,in which X refers to the distance from the epicardial surface to the deepest part of the trabecular recess,and Y is the distance from the epicardial surface to the peak of the trabeculation.An X/Y ratio up to 0.5 at end-diastole is enough for diagnosis.Chinet al[11] also acknowledged the relationship between the clinical presentation of the disease and genetically transmitted cardiac diseases[11].
Jenniet al[23] specified diagnostic criteria as NC/C>2 measured at end-systole and recommended additional morphological criteria including visualization of deep perfused intertrabecular recesses on color flow Doppler,involvement predominately in the lateral,apical,or inferior walls of the LV,and absence of additional cardiac anomaly[23].The contribution of Stöllbergeret al[12] to echocardiographic diagnostic criteria was>3 trabeculations apically to the LV papillary muscles,apart from aberrant bands and false tendons[12].However,there are many studies on the pitfalls of echocardiographic diagnostic criteria.One such was a study by Ottavianiet al[24],who measured trabeculations in the explanted hearts of 105 patients diagnosed as LVNC by echocardiography and who underwent orthotopic heart transplant.NC/C ratio was found as 1.7/1±0.2,demonstrating the discordance between echocardiography and pathology[24].Echocardiography has several limitations,such as such as being operator dependent,inadequate apex evaluation,difficulty in distinguishing the bilayer appearance,and inadequate short axis imaging.Therefore,the weak correlation between the existing echocardiographic diagnostic criteria has led to the increased use of CMR in diagnosis[25].CMR is a highly sensitive method in the diagnosis of LVNC and stands out with its ability to provide three-dimensional data,functional imaging,and tissue characterization with late gadolinium enhancement imaging[26,27].However,its diagnostic criteria for the disease are not fully established[28].
Regarding CMR based diagnostic criteria,Petersen et al[27] conducted a study evaluating trabeculation distribution and NC/C ratios in different patient groups,such as dilated cardiomyopathy,hypertrophic cardiomyopathy,as well as 7 patients with LVNC;they concluded that trabeculation ratio>2.3 (NC/C>2.3) measured in end-diastole SA supported non-compaction cardiomyopathy diagnosis with 86%sensitivity and 99% sensitivity[27].Fazio et al[29] performed end-diastole measurements in 8 patients diagnosed with LVNC and reported that it would be more appropriate to increase NC/C ratio to 2.5[29].Other CMR-based criteria are more quantitative measurements,based on the measurement of trabeculated mass developed by Jacquier et al[30] and Grothoff et al[31].Jacquier et al[30] conducted a CMR imaging study on trabeculation mass and reported that the trabeculated LV mass should be more than 25% of the total LV mass,and the noncompacted myocardial mass should be>15 g/m2[30,31].
Ventricular myocardium in LVNC has varying morphology ranging from increased spongiosis to dysplastic appearance.Changes in coronary microcirculation together with myocardial abnormalities are thought to play a role in the development of fibrosis.Late gadolinium enhancement may reveal findings of subendocardial and trabecular fibrosis.Although fibrosis may emerge as a follow-up parameter due to increased fibrosis occurrence in adult patients and advanced disease,recent studies have shown that late contrast enhancement may also occur in normally compacted myocardium[32,33].Similar to a study by Nucifora et al[34],the presence and prevalence of myocardial fibrosis may be associated with EF but is insufficient for diagnosis and follow-up[34].Thanks to advances in high resolution imaging,the sensitive imaging techniques can be used to detect even the slight variations in myocardial morphology within normal limits.Dawson et al[35] conducted a study to determine the anatomic norm of trabeculation and evaluated normal hearts of 120 healthy volunteers using CMR.Similar to LVNC,they demonstrated the highest volume of trabeculated myocardium was at a young age and in the apical anterior segments enddiastolic,however,the study needs to be supported by large cohort studies to determine normal limits[35].The increasing prevalence of the disease indicates the need for strict diagnostic guidelines that can distinguish between normal and pathological trabeculation.LVNC is associated with systolic dysfunction and may clinically progress to heart failure.However,the factors affecting global and regional systolic left ventricular functions and their relationship with the LV noncompacted myocardial mass are not clearly known.Therefore,studies have been conducted to examine the relationship between the change in LV systolic function and the distribution and extent of trabeculation.
In our study,we investigated the relationship between and global and regional EF of apical,midventricular,and basal regions and the trabeculation ratio and number of trabeculated segments of these regions in 65 patients diagnosed with LVNC.We did not find any concordance between EF and trabeculated segment number and ratio for all three regions or global LV.Choudhary et al[36] investigated the relationship between LV systolic function and global and regional LVNC mass.Contrary to our study,a significant inverse correlation was found between global EF and NC/C ratios in basal,apical,and midventricular regions in end-systolic measurements,and a significant inverse correlation was observed between end-systolic NC/C ratio and regional EF[36].Dellegrottaglie et al[37] used qualitative and quantitative methods such as wall motion score and fractional wall thickening to measure regional systolic function in 16 adult patients.In measurements of regional systolic functions,an inverse relationship was found between NC/C ratio and fractional wall thickening,and a direct relationship with wall motion score.In other words,a positive correlation was found between regional function and NC/C myocardial ratio.While no significant correlation could be found between the number of noncompacted segments and left ventricular EF,it was considered an indicator of global left ventricular dysfunction[37].
Choi et al[38] conducted a study on 145 people [24 isolated LVNC,33 non-isolated LVNC,30 dilated cardiomyopathy with noncompaction,27 dilated cardiomyopathy,and 31 healthy controls] and,similar to our study,did not find a significant correlation between left ventricular trabeculation volumes and EF in isolated LVNC patients compared to the control group[38].
Fazio et al[29] evaluated the relationship between ventricular dysfunction and the number of noncompacted segments in noncompaction cardiomyopathy and found that 122 of 238 patients (mean EF 44.39%) diagnosed with isolated LVNC had ventricular dysfunction with mean EF as 34.6%.However,they did not find a correlation between the number of affected segments and systolic dysfunction[29].
The severity and extent of myocardial involvement in patients with LVNC varies according to the stage of the disease and is heterogeneous.While some studies have found a significant relationship between trabeculation ratio and change in global ventricular function,other studies did not find a significant correlation between ventricular function and the ratio and frequency of trabeculation,as in our study.In addition,most of the studies conducted to date have focused on the relationship between trabeculation volume and global LV systolic function (EF).The limited number of studies on the impact to segmental function report varying results.In our study,we did not find a significant relationship between segmental function and the number of trabeculated segments or trabeculation ratio (P>0.05).
The main limitations of this study are the lack of control group and its retrospective design.In addition,cardiac biopsies and genetic factors were not available for the included patients.Histopathological findings and genetic factors could help to provide more accurate diagnoses for LVNC.
CONCLUSION
In conclusion,there is a need for large cohort studies that include healthy subjects in order to utilize changes in left ventricular function as a criterion in the diagnosis of LVNC.There is not enough evidence yet for the use of segmental and global functions in the diagnosis and follow-up of the disease.
ARTICLE HIGHLIGHTS
Research background
The frequency of left ventricular noncompaction cardiomyopathy (LVNC) diagnosis is increasing day by day due to inadequate diagnostic criteria.In addition,the criteria used cannot determine the prognosis and stage of the disease.
Research motivation
New cardiac magnetic resonance (CMR) criteria that can be used in the diagnosis of LVNC can explain when the increased trabeculation rate in healthy individuals can be called disease.In this context,left ventricular function changes due to increased trabeculation may be a parameter.
Research objectives
In our study,it was aimed to evaluate the relationship between LV global and regional function and trabeculation increase.A new parameter that can be used in diagnosis and follow-up will increase the diagnostic specificity of LVNC.
Research methods
The distribution and ratios of trabeculations in apical,midventricular,and basal regions were examined in CMR.In addition,by using short-axis cine images,regional ejection fraction (EF) and global EF were calculated with the Simpson method in the left ventricle (LV) at apical,basal,and midventricular levels.
Research results
Global EF was correlated with apical,midventricular,and basal regional EF,but there was no significant correlation between global EF and the number of trabeculated segments or trabeculation ratio in the global LV.Also,there was no significant correlation between regional EF and the number of trabeculated segments or trabeculation ratio in all three regions.
Research conclusions
Global and regional EF changes may be new diagnostic criteria in the diagnosis of LVNC and in the follow-up of the disease.
Research perspectives
Studies on the relation of LV segmental functions with trabeculation are limited.Studies with larger cohorts and control groups should be conducted.
 World Journal of Cardiology2021年7期
World Journal of Cardiology2021年7期
- World Journal of Cardiology的其它文章
- Sliding with the sines-fatal hyperkalemia:A case report
- Modes of failure with fractional flow reserve guidewires:Insights from the manufacturer and user facility device experience database
- Large eustachian valve fostering paradoxical thromboembolism:passive bystander or serial partner in crime?
- Current concept in the diagnosis,treatment and rehabilitation of patients with congestive heart failure