
A male-ABCD algorithm for hepatocellular carcinoma risk prediction in HBsAg carriers
2021-07-30 08:53:30YutingWangMinjieWangHeLiKunChenHongmeiZengXinyuBiZhengZhuYuchenJiaoYongWangJianZhuHuiZhaoXiangLiu0ChunyunDaiChunsunFanCanZhaoDeyinGuoHongZhaoJianguoZhouDongmeiWangZhiyuanWuXinmingZhaoWeiCuiXuehongZhang4Jianqia
Yuting Wang,Minjie Wang,He Li,Kun Chen,Hongmei Zeng,Xinyu Bi,Zheng Zhu,Yuchen Jiao,Yong Wang,Jian Zhu,Hui Zhao,Xiang Liu0,Chunyun Dai,Chunsun Fan,Can Zhao,Deyin Guo,Hong Zhao,Jianguo Zhou,Dongmei Wang,Zhiyuan Wu,Xinming Zhao,Wei Cui,Xuehong Zhang4,,Jianqiang Cai,Wanqing Chen,Chunfeng Qu
1State Key Lab of Molecular Oncology,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;2 Department of Clinical Laboratory,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;3 Office of Cancer Screening,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;4National Central Cancer Registry,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;5 Department of Hepatobiliary Surgery,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;6 Department of Diagnostic Radiology,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;7Department of Ultrasonography,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;8Qidong Liver Cancer Institute &Qidong People’s Hospital,Qidong 226200,China;9Lingbi Center for Disease Control and Prevention,Suzhou 234200,China;10 Mengcheng Center for Disease Control and Prevention,Bozhou 233500,China;11 Sheyang Center for Disease Control and Prevention,Yancheng 224300,China;12Shenqiu County Center for Disease Control and Prevention,Zhoukou 411624,China;13Dancheng Center for Disease Control and Prevention,Zhoukou 477150,China;14Channing Division of Network Medicine,Department of Medicine,Brigham and Women’s Hospital and Harvard Medical School,Boston,MA 02115,USA;15 Department of Nutrition,T.H.Chan School of Public Health,Harvard University,Boston,MA 02115,USA
Abstract Objective:Hepatocellular carcinoma (HCC) development among hepatitis B surface antigen (HBsAg) carriers shows gender disparity,influenced by underlying liver diseases that display variations in laboratory tests.We aimed to construct a risk-stratified HCC prediction model for HBsAg-positive male adults.Methods:HBsAg-positive males of 35-69 years old (N=6,153) were included from a multi-center populationbased liver cancer screening study.Randomly,three centers were set as training,the other three centers as validation.Within 2 years since initiation,we administrated at least two rounds of HCC screening using Bultrasonography and α-fetoprotein (AFP).We used logistic regression models to determine potential risk factors,built and examined the operating characteristics of a point-based algorithm for HCC risk prediction.Results:With 2 years of follow-up,302 HCC cases were diagnosed.A male-ABCD algorithm was constructed including participant’s age,blood levels of GGT (γ-glutamyl-transpeptidase),counts of platelets,white cells,concentration of DCP (des-γ-carboxy-prothrombin) and AFP,with scores ranging from 0 to 18.3.The area under receiver operating characteristic was 0.91 (0.90-0.93),larger than existing models.At 1.5 points of risk score,26.10% of the participants in training cohort and 14.94% in validation cohort were recognized at low risk,with sensitivity of identifying HCC remained 100%.At 2.5 points,46.51% of the participants in training cohort and 33.68% in validation cohort were recognized at low risk with 99.06% and 97.78% of sensitivity,respectively.At 4.5 points,only 20.86% of participants in training cohort and 23.73% in validation cohort were recognized at high risk,with positive prediction value of 22.85% and 12.35%,respectively.Conclusions:Male-ABCD algorithm identified individual’s risk for HCC occurrence within short term for their HCC precision surveillance.
Keywords:Hepatocellular carcinoma;asymptotic HBsAg carriers;risk prediction model;screening;laboratory tests
Introduction
Cirrhotic patients are at particularly high risk of hepatocellular carcinomas (HCC),a leading cause of cancer-related death and accounts for a large proportion of health economic burden (1,2).HCC surveillance every six months using B-ultrasonography (US) with or without determining serum α-fetoprotein (AFP),US/AFP is strongly recommended by professional societies including Asian-Pacific Association for the Study of the Liver (APASL) (3),American Association for the Study of Liver Disease(AASLD) and European Association for the Study of the Liver (EASL).Hepatitis B virus (HBV) causes HCC in absence of cirrhosis (1,4),AASLD updates the recommendations of HCC surveillance to all HBV chronically infected adults.In China,chronic HBV infection remains the leading risk factor of HCC (1).Resultsof a HCC-screening demonstration program using US/AFP biannually to HBsAg-positive adults in some rural communities of China showed no reduction in liver cancer mortality within first 4 years of follow-up (5).Antiviral therapy rarely cures HBV infection and needs life-long medications,considerable carriers with seropositive for hepatitis B surface antigen(HBsAg) did not receive the therapy (1,6).There were 257-291 million HBV chronically infected adults in 2015 worldwide (6).Tailoring to individual HCC risk is required for precision surveillance,so that limited HCC-screening resources could be allocated to high-risk individuals who might benefit most from early intervention or intensive surveillance (7).
In HBV chronically infected Asians,HCC incidence is different with variated risk factors and underlying liver diseases (1),the incidence rate was 3.2 per 100 person-years in patients with cirrhosis,and 0.4 in patients without cirrhosis (8,9).To predict long-term HCC occurrence in Asians,several HCC-risk models were constructed including REACH-B (10),CU-HCC (11),GAG-HCC(12) and AGED (13),which weighted significantly on HBV replication status,i.e.HBV-DNA,HBV e antigen(HBeAg).With the usage of nucleos(t)ide analogs that inhibit HBV replication,PAGE-B for Caucasian (14) and mPAGE-B for Asians (15) were constructed employing patient’s age,gender,baseline platelet (PLT) counts,and serum albumin (ALB) levels,which reflect the underlying liver diseases.EASL recommends HCC surveillance to non-cirrhotic HBV patients according to PAGE-B classes.Nevertheless,these models were mostly tested in patients with chronic hepatitis B by 2019 (16),evidences of current modification in surveillance strategy based on risk stratification models are insufficient for high-grade recommendation.None of these models was tested in Chinese HBsAg-carriers from rural community where liver cancer incidence was 20.0/105,which was higher than the urban (16.1/105) (17).
Previous studies conducted in rural community showed that <40% of HBsAg-positive adults complied to the biannually repeat US/AFP tests after initial 2-3 years for HCC-screening (4,18).HCC development depends on presence of premalignant cells and is significantly influenced by the underlying severity and activity of liver diseases (1,19).Molecular and pathological analyses displayed that preneoplastic lesions harbored genetic alteration and abnormal expression of cellular proteins.For routine surveillance in community population,the risk prediction models of short-term HCC occurrence will avoid ineffective and wasteful distribution of demanding screening efforts to those relatively low-risk individuals (7).HBV-associated HCC developed more frequently in males than in females,with a female/male ratio of 1:4-7,due to the different effect of androgen and estrogen on HBV pathogenesis and carcinogenesis (3,20,21).In addition,healthy females have higher platelet and white blood cell counts than males (22).The serum level of alanine aminotransferase (ALT) was higher in healthy Chinese males than in females (23).The currently constructed HCC prediction models used the same variation and weigh in both gender of these laboratory tests,which reflect liver diseases at different severity and activity.In this study,based on a large population-level screening program in rural China,we aimed to build up a risk-stratified HCC prediction model for HBsAg-positive males using measurable tests which are currently performed in clinical laboratories.
Materials and methods
Participants and study design
The study participants were derived from the Communitybased Cohort study on Population with high risk of Liver Cancer (the CCOP-LC cohort;Chinese Clinical Registry,ChiCTR-EOC-17012853),which was described previously(24).CCOP-LC conducted community-based liver cancer screening by US/AFP in six rural areas (Lingbi county,Mengcheng county,Sheyang county,Shenqiu county,Dancheng county and Qidong county) from three provinces (Anhui,Jiangsu and Henan) in China since October 2017.Cluster sampling was used to select candidate screening sites where counties had a relatively higher incidence and mortality of liver cancer.All females and males aged 35-69 years who had no history of cancer(self-reported) in the selected villages (the smallest unit) of the participating counties were approached by means of personal contact and phone invitation by trained local medical staff.After receiving immunochromatographic strip-test for HBsAg,the HBsAg-positive participants were included in the cohort.Face to face interviews were conducted to collect sociodemographic information,body weight and height,lifestyle (smoking,drinking,eating habits,etc.),and family history of liver cancer among firstdegree relatives.HCC screening by US/AFP was provided annually. The study protocol (NCC201709011) was approved by Ethics Committee of National Cancer Center/Cancer Hospital,Chinese Academy of Medical Sciences (NCC/CH-CAMS) in Beijing.Each participant provided written informed consent before undertaking any study-related procedures in accordance with Good Clinical Practice and principles of the Declaration of Helsinki.
In the present study,we included HBsAg-positive males who met the inclusion criteria:1) males at 35-69 years old;2) HBsAg-positive;3) no previously diagnosed HCC or other malignant diseases;and 4) no other diseases that restricted taking the examinations of dynamic computed tomography (CT) or magnetic resonance imaging (MRI).Three screening centers (Lingbi,Mengcheng,and Sheyang) were randomly assigned as training cohort,the other three centers (Shenqiu,Dancheng and Qidong) as validation cohort (Figure 1).
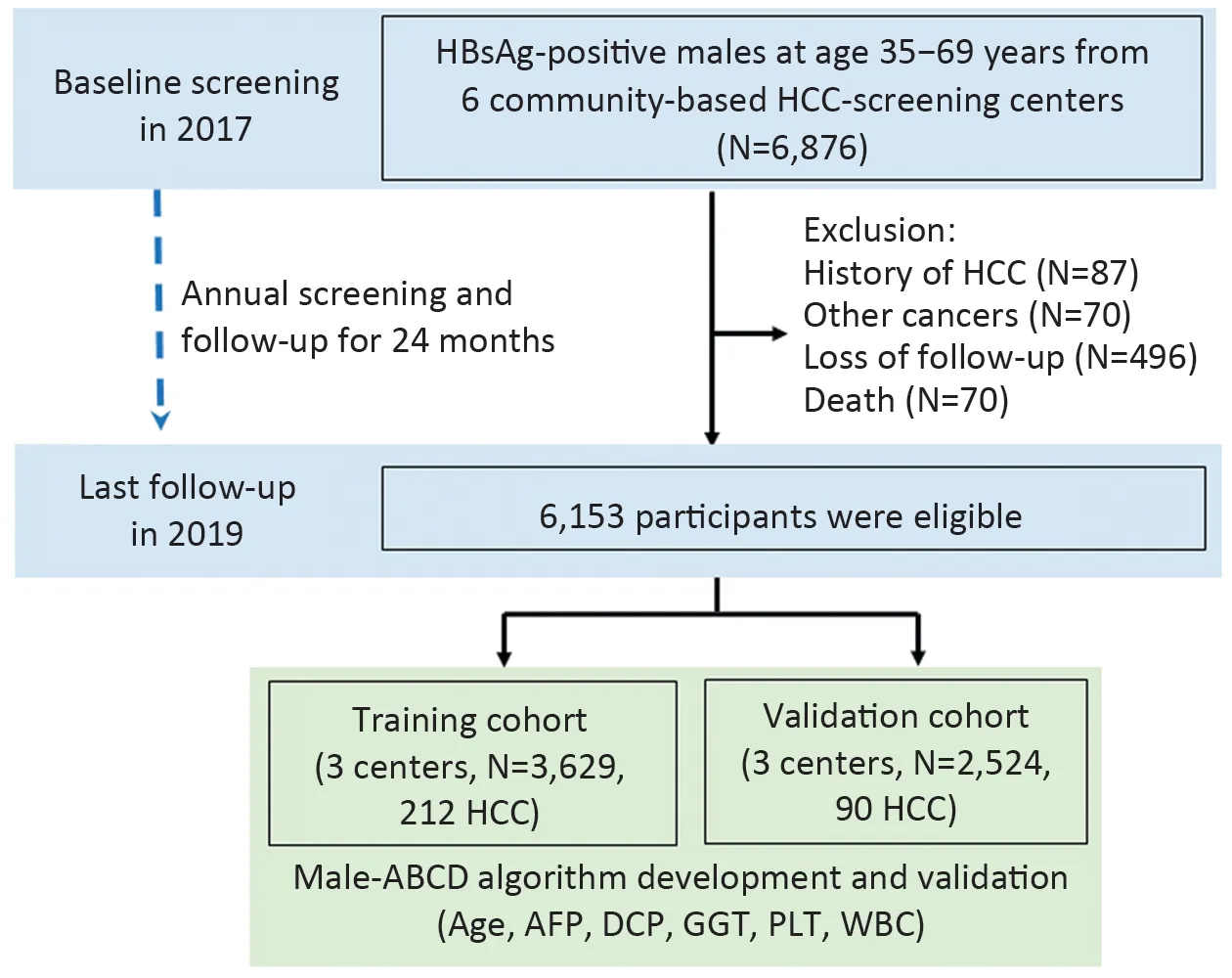
Figure 1 Flowchart of study population from multicenter population-based liver cancer screening.HBsAg,hepatitis B surface antigen; HCC,hepatocellular carcinoma; AFP,αfetoprotein;DCP,des-γ-carboxy-prothrombin;GGT,γ-glutamyltranspeptidase;PLT,platelet;WBC,white blood cell.
Laboratory tests
At baseline,for each participant,we measured PLT and white blood cell (WBC) counts;blood levels of ALT,aspartate aminotransferase (AST),γ-glutamyl transpeptidase(GGT),ALB;and HCC biomarkers of AFP and des-γcarboxy-prothrombin (DCP).For participants in training cohort,we also detected their blood concentrations of HBV-DNA,HBsAg and HBeAg.PLT,WBC,ALT,AST,ALB and AFP were measured immediately after blood drawn in each screening center independently using unified reagents.Using commercialized Abbott reagents,blood levels of GGT,concentrations of HBV-DNA,HBsAg,HBeAg,DCP were determined,and AFP was doublechecked in the central laboratory of NCC/CH-CAMS using the plasma that were snap frozen in -80 °C for 1-2 months.HBV-DNA concentration was determined by quantitative real-time PCR using the reagents from Kehua Biotechnology in Roche LightCycler 480 II.
Surveillance and HCC diagnosis
Every year,individuals were offered US/AFP examination and defined as US/AFP-positive,US/AFP-suspected,or US/AFP-negative. “US/AFP-positive” individuals had either of the following:1) serum AFP levels of >400 ng/mL regardless of US-detected nodule;2) US-detected nodule of ≥2 cm in size regardless of serum AFP concentration;and 3) US-detected nodule of ≥1 cm in size with serum AFP≥200 ng/mL.“US/AFP-suspected” individuals had either of the following:1) serum AFP levels of ≥20 ng/mL regardless of US-detected liver nodule;and 2) US-detected nodule of ≥1 cm in size.“US/AFP-negative” individuals were defined as having serum AFP levels of <20 ng/mL without an US-detected liver nodule.Individuals with“US/AFP-positive” and “US/AFP-suspected” were referred to specialists for HCC confirmation diagnosis. All diagnosed HCC cases were ascertained by dynamic CT or MRI.CT/MRI images were independently evaluated by two radiologists from NCC/CH-CAMS.When diagnosis was unconfirmed,participants were offered and volunteered for US/AFP examination 3-6 months later.We also offered the examination to 20%-30% of participants with US/AFP-negatives 6 months later based on a randomized number after dividing them into groups of 35-44,45-54,55-64,and ≥65 years old.We further linked our data with local population-based cancer registries and bureaus of vital statistics of each center and confirmed liver cancer outcome(ICD-10 code C22.0 or C22.9) by Dec.31,2019.
Statistical analysis
All variables at baseline were first evaluated with unconditional univariate logistic regression analysis.The variables with P<0.1 in univariate analysis were further assessed by stepwise multivariable logistic regression.Variables with P<0.05 in multivariable logistic regression were subsequently included. The discrimination was evaluated by the area under the receiver operating characteristic curve (AUROC) and its 95% confidence interval (95% CI).Calibration was assessed by the Hosmer-Lemeshow test.
Then we created a point-based prediction rule based on coefficient-based model.The coefficient of each variable was divided by the smallest coefficient in the model and rounding to the nearest 0.1.In addition to overall performance,discrimination and calibration,the performance of the prediction rule was assessed according to its accuracy,including sensitivity,positive predictive value (PPV),negative predictive value (NPV),and the proportion of individuals of each risk group at different cutoff of risk score.
We validated the model internally using bootstrap procedure in the training cohort by sampling with the replacement for 1,000 iterations.The model was further externally validated in the independent validation cohort.With the same cutoff values defined in the training cohort,we measured the sensitivity,PPV,NPV,and the model predicted proportion of individuals in each risk group.The analyses were performed using R software (Version 3.6.0;R Foundation for Statistical Computing,Vienna,Austria).
Results
Participant demographics
At baseline in 2017,from six HCC-screening centers of three provinces,a total of 116,542 males aged 35-69 years received HBsAg test;among them,6,876 HBsAg-positive(confirmed with Abbott reagents) males were recruited.We excluded 723 male participants,of whom 87 were diagnosed with HCC before baseline,70 were diagnosed with the other cancers,and 70 died from the causes other than HCC during the study period,and 496 lost follow-up.At the last follow-up in Oct.2019,a total of 6,153 eligible HBsAg-positive males were included in our analyses.The training cohort recruited 3,629 HBsAg-positive males with 212 HCCs.Validation cohort recruited 2,524 HBsAgpositive males with 90 HCCs (Figure 1).The distribution in participants’ age and the other factors varied significantly at baseline among cohorts (Table 1).
Male-ABCD algorithm development and performance
All parameters in the model development and validation were based on the baseline tests.In univariate analysis,the following variables showed significance of P<0.1 and they were used for further model selection (age,AFP,DCP,GGT,PLT,WBC,ALB,ALT,AST,and HBV-DNA)(Supplementary Table S1).In stepwise multivariate logistic regression,only age and five laboratory variables entered into the last model (Table 2).Based on these six variables,a coefficient-based model was employed to develop the score-based prediction rule,which was named male-ABCD algorithm,representing participant’s age,blood levels of GGT,counts of PLT,WBC,and concentration of DCPand AFP.Figure 2Ashows the sensitivity and specificity of different combinations.AUROC of coefficient-based male-ABCD was 0.93 (0.92-0.95),which was higher than the AFP and DCP combination (AUROC=0.84,P<0.001,DeLong’s test),or the combination with age (AUROC=0.88,P<0.001,DeLong’s test).The χ2of the Hosmer-Lemeshow test was 3.77 (P=0.88).Male-ABCD presented the lowest Akaike Information Criteria (AIC) of 887.18 compared with the AFP and DCP combination (AIC=1,007.08),or the combination with age (AIC=973.77),suggesting that it was the most suitable one.The algorithm was converted into a point-based prediction rule by dividing the coefficient of each variable by the smallest coefficient in the model (0.85) and rounding to the nearest 0.1.The total score ranges from 0 to 18.3.(Table 2).

Figure 2 Receiver operator characteristic curves of male-ABCD.(A) Comparison of male-ABCD with combination of age,AFP and DCP in training cohort;(B) Comparison of male-ABCD with some established models among 6,153 HBsAg-positive males.AUROC,area under the receiver operating characteristic;95% CI,95% confidence interval;AFP,α-fetoprotein;DCP,des-γ-carboxy-prothrombin;GGT,γglutamyl-transpeptidase;PLT,platelet;WBC,white blood cell.

Table 1 Baseline characteristics of training and validation cohorts
Point-based HCC prediction and stratification by male-ABCD
For each given participant,the risk score was calculated based on the male-ABCD algorithm.At different risk-score cutoffs,male-ABCD grouped the HBsAg-positive males into the variated proportion of HCC at high risk or at lowrisk.Table 3shows the sensitivity of identifying HCC within 2 years when the cutoff of risk score was set at different points,and PPV among the group at high risk,NPV at low risk.The performance of male-ABCD in training cohort was compared with previously developed risk-stratification models of AGED (13),REACH-B (10),PAGE-B (14),mPAGE-B (15) for general hepatitis B patients,and THRI (25) for cirrhotic patients and GALAD(26) for HCC diagnosis among the high-risk population.Male-ABCD generated the largest AUROC over AGED,REACH-B,PAGE-B,mPAGE-B,and THRI and GALAD(with all P-values less than 0.001,Delong’s Test)(Supplementary Table S2).
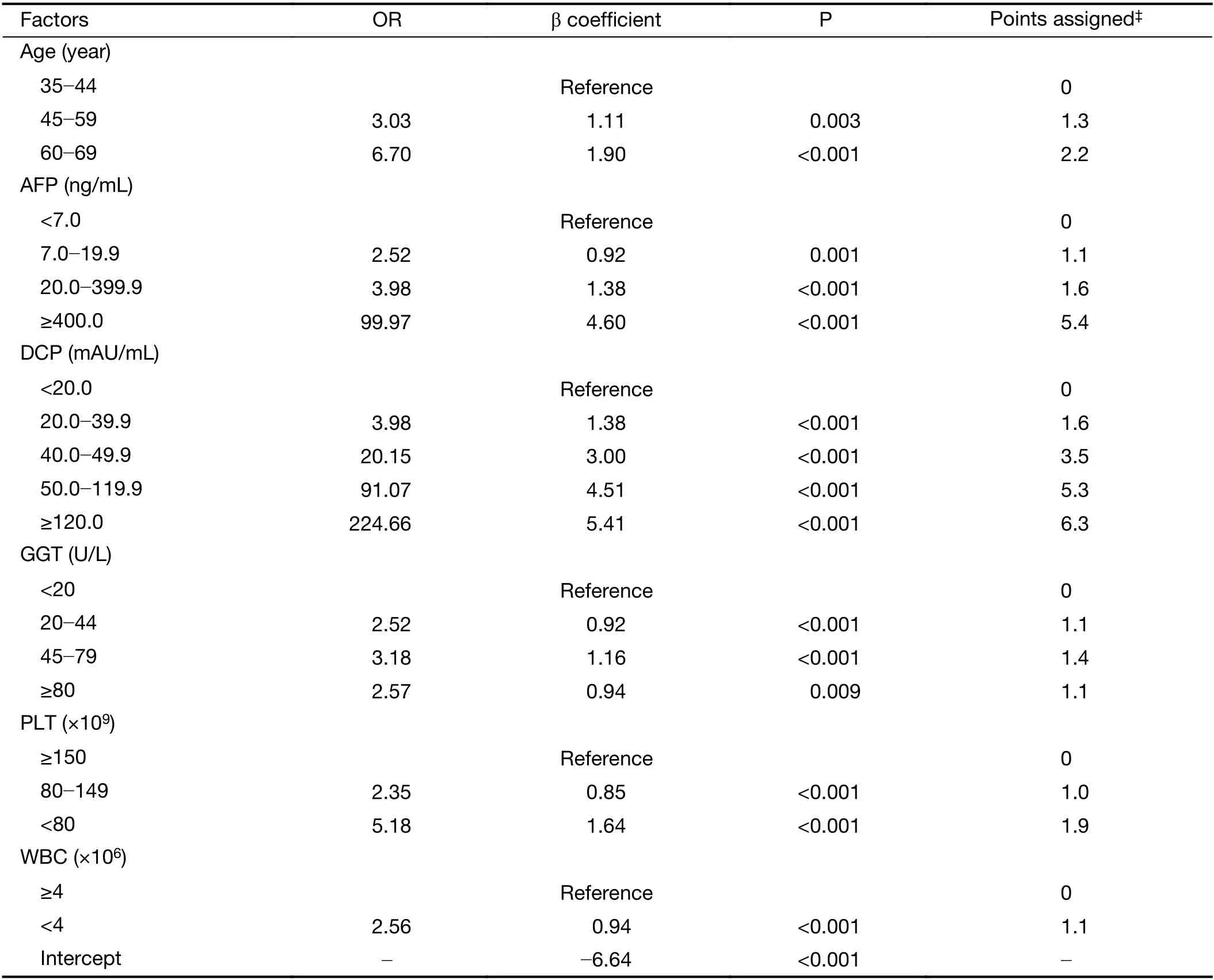
Table 2 OR and β coefficient of multivariate logistic regression analysis and point-based scoring system of male-ABCD
Validation of male-ABCD algorithm
The male-ABCD was validated in an external cohort of 2,524 HBsAg-positive males (Table 3).At 1.5 points of risk score,prediction reached 100% of sensitivity both in training and validation cohort.At 2.5 points,46.51% of the participants in training cohort,33.68% in validation cohort were recognized at low risk with 99.06% and 97.78% of HCC prediction sensitivity,respectively.NPV among population at low risk was 99.88% and 99.76%,respectively.At 4.5 points,20.86% of the participants in training cohort,23.73% in validation cohort were recognized at high risk.The PPV among the population at high risk reached 22.85% in training cohort and 12.35% in validation cohort (Table 3).
Comparison of male-ABCD with AGED,REACH-B,PAGE-B,mPAGE-B,THRI and GALAD
For HCC prediction and stratification,male-ABCD was compared with previously constructed models by the other investigators among the total of 6,153 HBsAg-positive males (Table 4). Male-ABCD generated the largest AUROC (with all P values less than 0.001,Delong’s Test)in comparison with the models of AGED (13),REACH-B(10),PAGE-B (14) and mPAGE-B (15) that were constructed based on hepatitis B patients,with THRI (25)that was based on cirrhotic patients,and with GALAD (26)that was used for early diagnosis of HCC among high-risk population (Figure 2B).For risk-stratification,male-ABCD predicted 21.52% of total HBsAg-positive males into HCC at low risk with 100% of sensitivity at 1.5 points of risk score.With 100% of prediction sensitivity,REACH-B recognized 4.27% and PAGE-B predicted 3.17% of the total as HCC at low risk.At 2.5 points of risk score,male-ABCD predicted 41.25% of total HBsAg-positive males into HCC at low risk with 98.68% of sensitivity,and the NPV reached 99.84%.The missed four HCCs were detected 6.1,9.9,9.9,19.9 months later since the baseline tests,respectively.While AGED predicted 6.37%,and mPAGE-B predicted 9.25% of total into HCC at low risk with 99.06% and 99.01% of sensitivity,and 99.13% and99.47% of NPV,respectively.With a risk score of 2.5-4.5 points based on male-ABCD,25.50% (13/51) of HCCs were detected between 12-24 months.
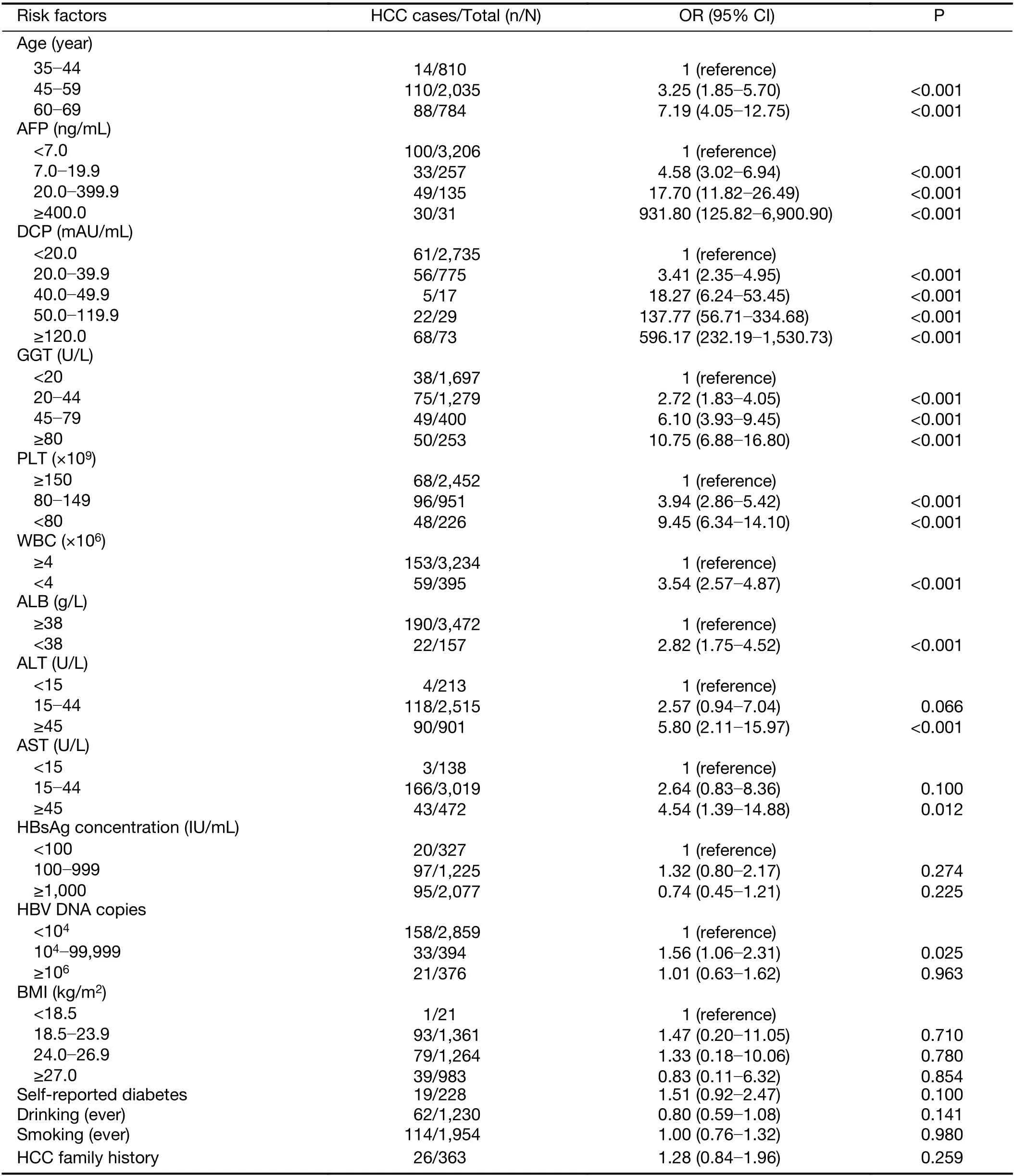
Table S1 Univariate logistic regression analysis of training cohort (N=3,629)
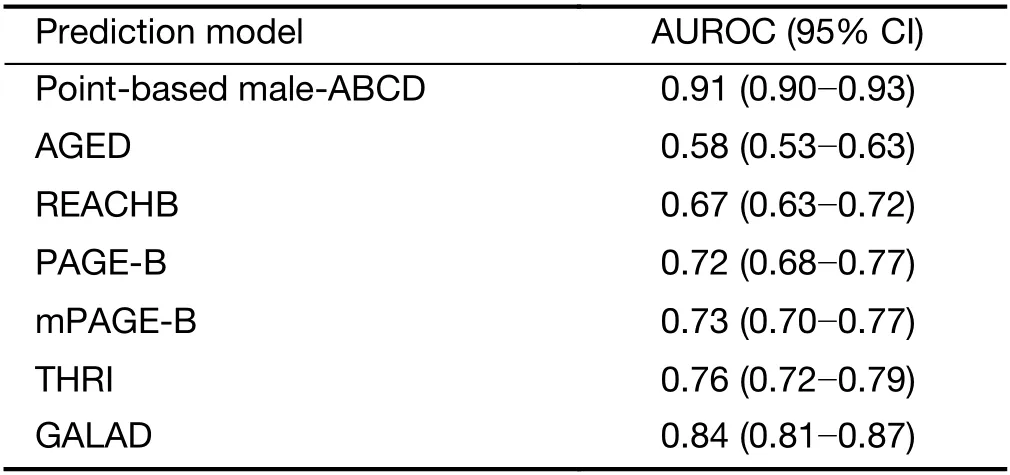
Table S2 Comparison of AUROC of point-based male-ABCD and some established models for HCC in training cohort
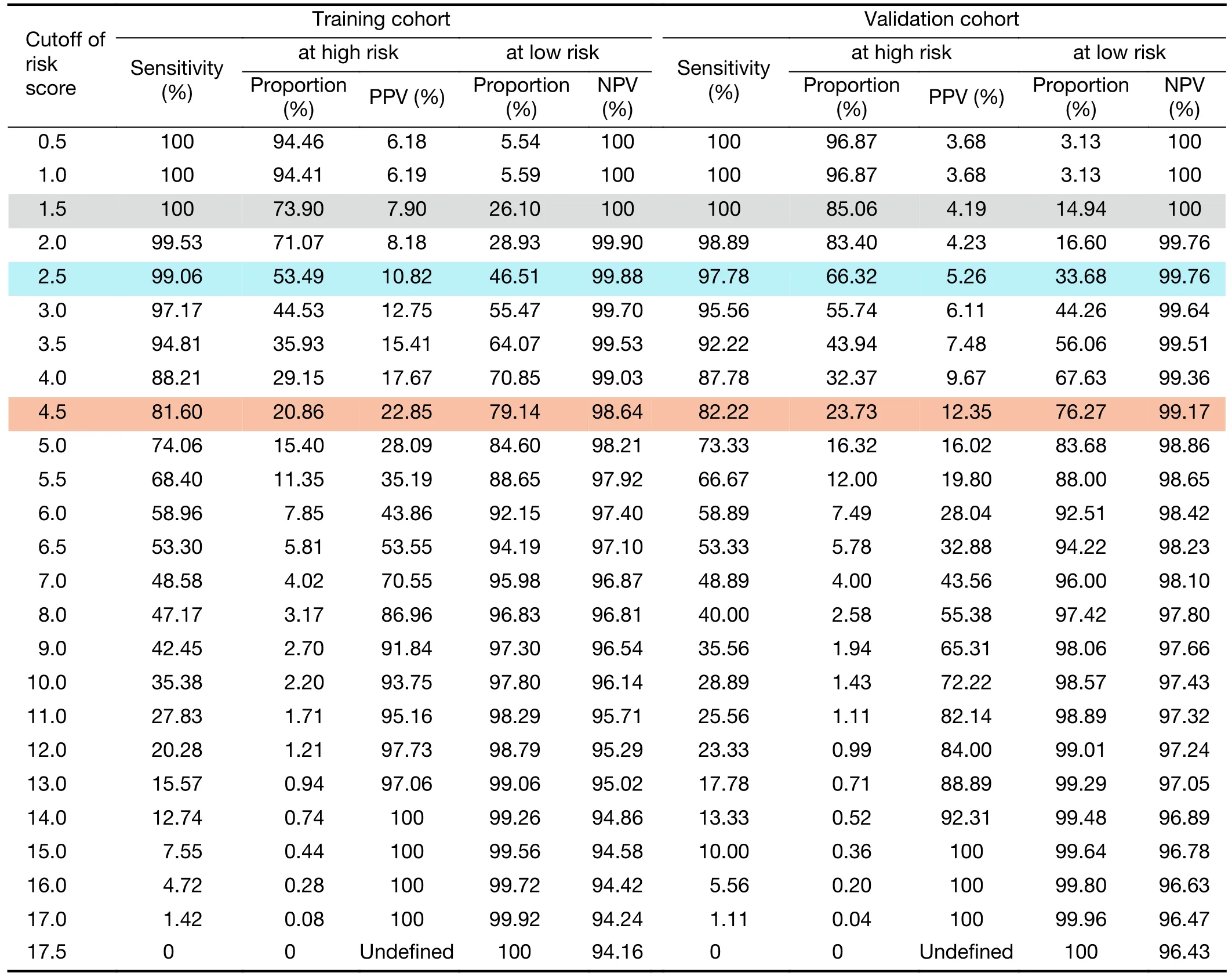
Table 3 Accuracy and HCC risk category at different cutoffs of risk score
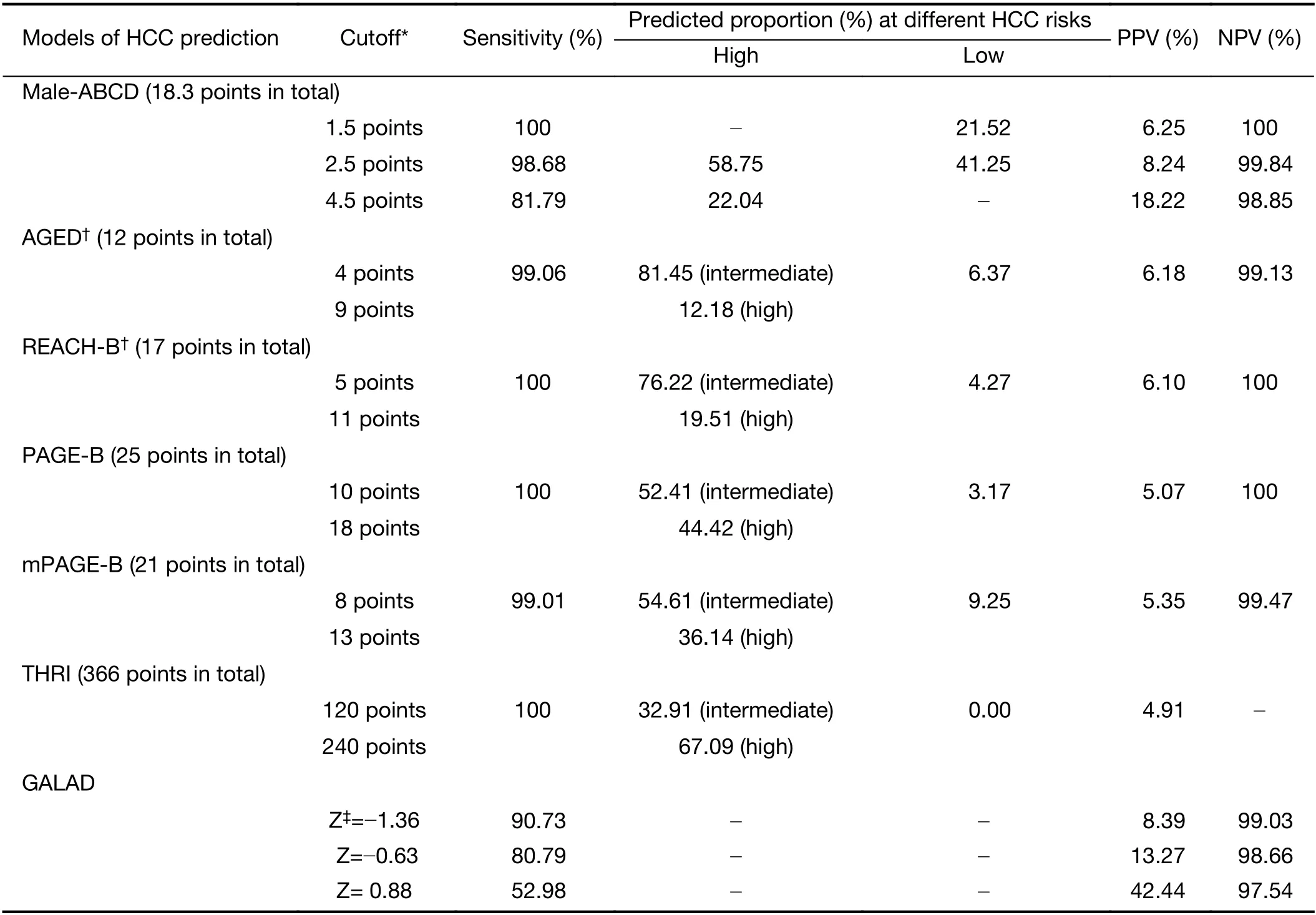
Table 4 Performance of male-ABCD and some established models for HCC prediction and stratification among 6,153 HBsAg-positive males
Discussion
Based on a large population-level screening program,this study included 6,153 HBsAg-positive male adults from six HCC-screening centers of three provinces in rural China.In this perspective,multicenter study,we developed and validated an HCC risk-stratified algorithm named male-ABCD,which represents participant’s age,blood levels of GGT,counts of PLT,WBC,and concentration of DCP and AFP.Based on this algorithm,for a given HBsAgpositive male,his HCC risk within 2 years was recognized at low risk when the risk score was ≤2.5 points,particularly≤1.5 points.However,this HCC risk within 2 years was very high when the risk score reached >4.5 points.For the population of HBsAg-positive male adults with the pointbased prediction,1,324 of total 6,153 HBsAg-positives(21.52%) were grouped into HCC at low risk when risk score was ≤1.5 points,none HCC occurred within 2 years.At 2.5 points of cutoff,2,538 of 6,153 (41.25%) HBsAgpositives were recognized HCC at low risk,only four HCCs occurred within 2 years.The sensitivities were 99.06% in training cohort,and 97.78% in validation cohort with 99.88% and 99.76% of NPV,respectively.At 4.5 points of cutoff,22.04% (1,356/6,153) of the HBsAg-positives were recognized as HCC at high risk within 2 years with 18.22% of PPV.After head-to-head comparison with previously developed models of AGED (13),REACHB (10),PAGE-B (14),mPAGE-B (15) for general hepatitis B patients,THRI (25) for cirrhotic patients,and GALAD(26) for HCC diagnosis among high-risk population,male-ABCD generated the largest AUROC.Our current study indicated that HBsAg-positive male adults could be identified at different HCC risk based on male-ABCD algorithm.The tests employed in are measurable and currently performed in clinical laboratories.As barriers in the community to screen all HBsAg carriers biannually,male-ABCD algorithm provided an applicable model for identifying the higher risk group who truly need intense screening intervals.
Several studies in clinic-based patients indicated that the combination of AFP/DCP,which are employed in the GALAD for early HCC diagnosis (26),discriminates early HCC from benign chronic liver diseases (1,27,28).AFP has been widely used for HCC surveillance (29),DCP elevation was observed several months before HCC occurred (24,27).When cutoff values were fixed at AFP=20 ng/mL,DCP=40 mAU/mL,the combination well discriminate HCC from benign liver diseases 12 months before the clinical HCC diagnosis based on patients of two genders (22).Among the HBsAg-positive males,we observed that HCC risk increased when DCP≥20 mAU/mL and AFP≥7 ng/mL.We didn’t include AFP-L3 because our previous results indicated that AFP-L3 addition decreased the sensitivity of HCC discrimination from cirrhosis (28).Increase of serum GGT is related to liver inflammation and is also recognized as an independent HCC risk factor (30,31).We previously reported that GGT with some clinical factors predicted 3-year HCC occurrence among HBsAg-positive individuals (30).Our current study showed that GGT at 20-44 U/L and ≥80 U/L showed similar impact,but higher impact at 45-79 U/L on HCC risk.PLT is a critical indicator of cirrhosis,which is at particularly high risk of HCC (25,29).Our study showed that adding these laboratory tests that reflect the underlying severity of liver diseases to age/AFP/DCP,the algorithm significantly improved the sensitivity and risk-stratification among the HBsAg-positive male adults.
The current male-ABCD was constructed based on the HBsAg-positive male adults from community population instead of patients from hospitals.HBV has long-term effects on HCC,that higher levels of serum HBV-DNA and HBsAg showed increased HCC risk in the models of REACH-B and GAG-HCC (10,12,30).We failed to observe their impact on HCC occurrence in short term.It has been documented that normal values of ALT and PLT in healthy males are different from healthy females (22,23).We failed to observe the significant effect of elevated blood levels of AST and ALT on REACH-B (10),and decreased blood albumin levels on CU-HCC (11),mPAGE (15) as the short-term HCC risk factor for the HBsAg-positive males.
HCC surveillance every six months using US/AFP is recommended by many professional societies.However less than 40% of HBsAg-positive adults complied to the biannually repeated US/AFP tests after initial 2-3 years for HCC-screening (5,18).Precision surveillance could be allocated to high-risk individuals who might benefit most from early intervention or intensive surveillance.As the limitation of B-ultrasonography in the detection of early HCC (32),individuals at the very early stage of HCC could be missed out.In the current study,we aimed to identify any of HCC cases who had developed clinical HCC and those who were at very high risk of HCC developing within short period.With the risk assessment using male-ABCD,the HBsAg-positive males were grouped into at high risk,or at low risk.This discrimination would be helpful to take different strategies to monitor their HCC.Based on male-ABCD,no HCC occurred among the 1,324 of total 6,153 (21.52%) HBsAg-positive males with risk score of ≤1.5 points.Instead of the biannually examination,the annually or longer interval follow-up would reduce the total US-examination number to avoid over-screening,and relieve the participant anxiety.However,22% (1,356/6,153) of the HBsAg-positive males were recognized with the risk score of >4.5 points and the PPV reached to 18.22%.It is better for these population of HCC at high risk strictly follow the recommendation by professional societies,which is US/AFP examination every six months (3).
The male-ABCD is constructed based on HBsAgpositive males.The applicability for HBsAg-positive females may not be suitable,and needs to be evaluated in the future.Because the population of training and external validation cohorts were derived from different provinces,their characteristics were quite different.The discrimination of point-based male-ABCD in external validation cohort was acceptable,with an AUC of 0.90(95% CI:0.86-0.93) and sensitivity of 97.78% at the cutoff value of 2.5 points.However,the proportion of at low risk was 14.94% (at 1.5 points of cutoff) and 33.68% (at 2.5 points of cutoff) in validation cohort,lower than that of training cohort (26.10% and 46.51%,respectively).The generalizability of male-ABCD should be further evaluated by external validations based on randomized controlled trial of liver cancer screening.To avoid recall bias and selfreported bias,our model development was based on age and laboratory variables that are objective and measurable.Several potential factors,such as cirrhosis,were not included in the current analysis,which would impair the performance as well as generalizability of the model.Clinically,cirrhosis is typically classified as compensated and decompensated cirrhosis,and compensated cirrhosis is usually free of symptoms with a better quality of life than decompensated cirrhosis.The diagnosis of cirrhosis at clinical early state is depended on the liver stiffness measurement with sophisticated instrument or in combination with platelet count and spleen size (33).Bultrasonography is not sensitive enough and is easily affected by the operator’s experience and subjective judgment.Therefore,in the current study,Bultrasonography detected cirrhosis was not selected as a candidate predictor.We will perform further investigations when data are available to solve this issue.No significant impact of higher levels of HBV-DNA on HCC occurrence in short-term was observed,which potentially provides a window time for the standardized antiviral therapy to reduce HCC risk (10-13) as around 80% of participants in our study received no and/or not-standardized antiviral therapy.With the reduced cost and the use of more effective antiviral medicines,the applicability of male-ABCD needs to be further evaluated.
Different from REACH-B (10),AGED (13),PAGE-B(14),mPAGE-B (15) and THRI (25),male-ABCD was unable to class the HBsAg-positive males into HCC at highest and HCC at middle-high risk,respectively.However,when risk score was >4.5 points based on male-ABCD,our model recognized around 22% of HBsAgpositive males into HCC at high risk with 18.22% of PPV.
Conclusions
The male-ABCD algorithm could identify individual HCC risk within 2 years since initial laboratory tests among HBsAg-positive males.All tests are currently performed in clinics with an immediate clinical applicability for their HCC precision surveillance.
Acknowledgements
This work was supported by State Key Projects Specialized on Infectious Diseases (No.2017ZX10201201-006),Key research projects for precision medicine (No.2017YFC0908103),Innovation Fund for Medical Sciences of Chinese Academy of Medical Sciences (CIFMS,No.2019-I2M-2-004,2016-I2M-1-007,2019-I2M-1-003),and National Natural Science Foundation Fund (No.81972628,No.81974492).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2021年3期
Chinese Journal of Cancer Research2021年3期
- Chinese Journal of Cancer Research的其它文章
- Current evidence and challenges of systematic therapies for adult recurrent glioblastoma:Results from clinical trials
- Phase 1 studies comparing safety,tolerability,pharmacokinetics and pharmacodynamics of HLX01 (a rituximab biosimilar) to reference rituximab in Chinese patients with CD20-positive B-cell lymphoma
- Single-cell DNA methylome analysis of circulating tumor cells
- Prognostic value of a modified Immunoscore in patients with stage I-III resectable colon cancer
- Profiling of hepatocellular carcinoma neoantigens reveals immune microenvironment and clonal evolution related patterns
- Pain threshold,anxiety and other factors affect intensity of postoperative pain in gastric cancer patients:A prospective cohort study