
Update on the management of the gastrointestinal effects of radiation
2021-05-20 08:23:44
Hannah McCaughan,Stephen Boyle,John J McGoran,Department of Gastroenterology,Altnagelvin Area Hospital,Londonderry BT47 6SB,United Kingdom
Abstract Radiation therapy is a long-established and essential modality in the treatment of many cancers.It is well known that tissue within a field of radiation can suffer indiscriminate effects,leading to acute and chronic problems.The gastrointestinal tract may be adversely affected by radiation.From the mouth to the rectum,patients can experience troublesome symptoms that require the concerted input of specialist teams.Interventions range from nursing care,dietetic optimization,pharmacological management,and mechanical procedures through endoscopy and surgery.Quality evidence exists mainly for radiation induced effects in four distinct areas of the gastrointestinal tract:oral mucosa,esophagus,small bowel,and rectum.This review explores the experiences of oncology and gastrointestinal teams in managing the most common conditions and some of the different practices for radiation associated morbidity.
Key Words:Radiation; Stricture; Endoscopy
INTRODUCTION
Worldwide epidemiological data suggests that around half of all patients with a cancer diagnosis may benefit from some form of radiation treatment[1,2].Due to the nature of radiation therapy,normal tissue is also included within the radiation field.The involvement of gastrointestinal (GI) tissue has the potential to create a significant burden of patients with new GI symptoms as a by-product of cancer therapy[3,4].Side effects can present long after cessation of treatment,so vigilance is advised with longterm care.
A combination of surgical,radiation,and chemotherapy agents are often combined to create a treatment regimen.This combination of therapies has also been shown to increase the risk of radiation effects.For example,an up to three-fold increase in GI toxicity has been noted in combined therapy for uterine cancer[5].
A multidisciplinary approach with medical gastroenterology input is recommended to manage the range of morbidities.The underlying symptomatology is diverse; side effects may be dose or schedule related.However,other factors such as genetic and patient-related issues play a role[5-7].This range of symptomatology has a significant impact on patient quality of life,and the dosage required to cause GI side effects is dependent on the underlying tissue[8].
With modern treatment modalities the clinician’s aim is to reduce these adverse effects.Effort is made during radiotherapy planning to limit damage to bystander tissue,either through more sophisticated machinery or employment of techniques prior to therapy[9].Local treatment such as brachytherapy (when contrasted with external beam treatments) reduces GI toxicity.Similarly,there is an improvement in toxicity with techniques such as intensity modulated and three-dimensional conformal radiotherapy compared to conventional radiotherapy.
Nutrition plays a significant role within cancer therapy and will be discussed throughout this review.Recognition of the underlying nutritional state is important prior to initiating therapy[10].It has additional significance in management of symptoms secondary to cancer therapies.Radiation causes a significant burden throughout the GI tract,requiring a range of interventions to ensure adequate nutrition[11,12].
GI side effects from radiation treatment are an ever-changing set of clinical issues.This review aims to give a summary overview on recent treatment recommendations.Four commonly impacted areas of the GI tract are explored:oral mucosa,esophagus,small bowel,and rectum.
ORAL MUCOSA
The incidence of oral mucositis in patients receiving high-dose head and neck radiation (6000-7000 Gy) is estimated up to 85%.It is one of the limiting factors for further oncological treatment in advanced head and neck cancer,impacting upon prognosis.The pain associated with oral lesions may lead to malnutrition and requires intense attention to manage it including the use of sufficient analgesia.A nutritional risk assessment for this patient population is advisable in order to anticipate requirements for early enteral nutrition to supplement poor oral intake[13,14].
The use of midline radiation blocks and three-dimensional radiation treatment to reduce mucosal injury is useful.Benzydamine oral rinse is recommended for prevention of radiation-induced mucositis in patients with head and neck cancer receiving moderate-dose radiation therapy.Xerostomia is a common side effect of irradiation of the head and neck,with treatment aimed at saliva replacement and stimulation.Oral candidiasis is treated with topical antifungals.Amifostine (Ethyol),a free-radical scavenger radioprotectant,is beneficial in preventing and treating xerostomia,but there is insufficient evidence to support its use for radiation-induced mucositis and esophagitis[15].
ESOPHAGUS
Radiation esophagitis can present early or late.The addition of chemotherapy further increases the likelihood of developing esophageal structuring[16].The risk of stricturing in the esophagus can be anticipated by greater tumor invasion and circumferential involvement.Mediastinal fibrosis resulting from radiation therapy can lead to progressive and frequently refractory esophageal stenosis[17-19].
In the acute phase,esophagitis has the potential to cause significant morbidity for patients.Simple therapies such as analgesia,topical anesthesia,proton pump inhibitors,and dietary modifications are appropriate.This is often a self-limiting condition but can necessitate an alteration or cessation of treatment[20-22].Certain foods including tobacco,alcohol,coffee,capsaicin containing foods,and ingestion of substances with extremes of temperature may irritate the esophageal mucosa.A soft or pureed bland diet is typically advised but often difficult to tolerate.A specialized dietetic assessment can provide estimates of daily nutritional requirements and advice for optimizing protein and calorie intake,such as the addition of liquid meal replacements[22].Mild to moderate odynophagia responds to topical analgesics such as oral viscous lidocaine.Patients with esophagitis may have reduced lower esophageal sphincter pressure and are prone to reflux.These patients should be prescribed a proton pump inhibitor or H2 receptor antagonist[23].When esophagitis has not resolved with supportive therapy,consideration needs to be made to nutrition.In appropriate cases this may be the initiation of parenteral nutrition (PN) to allow for mucosal healing[12].
Post radiation esophageal strictures are often classified as complex with features including length > 2 cm,angulated,irregular,and severely narrowed.Dilatation is the mainstay of treatment for benign strictures.Most patients will have partial occlusion of the esophagus rendering them amenable to anterograde endoscopic dilatation with either bouginage or endoscopic balloon therapy[24].
Symptoms from late radiation strictures typically include mechanical dysphagia from stenosis or impaired motility secondary to neuropathy and odynophagia from chronic ulceration[25].For a completely obstructed esophagus,a combined anterograde and retrograde approach can be taken.In this complex procedure the stricture is visualized firstlyviathe anterograde endoscope.The second endoscope is insertedviaa gastrostomy and is used to feed a guidewire proximally.This procedure is often performed with general anesthetic and under radiological guidance to manage the risk of perforation.When luminal patency is achieved these patients will often require serial esophageal dilatation every 2-3 mo[26].Refractory esophageal strictures(an inability to maintain a luminal diameter of > 14 mm following five sequential dilatation attempts 1-2 wk apart or maintain the diameter once it has been achieved for 4 wk) are rare and challenging.There is a lack of good quality evidence surrounding the best approach to treatment,but some individuals may benefit from self-expanding removable stent insertion[27,28].Those with radiation strictures may need additional help to manage undernutrition involving enteral or parenteral routes after appropriate assessment[12,29].
SMALL BOWEL
Small bowel tissue is particularly sensitive to radiation due to its high cell turnover[30].Acute small bowel symptoms are due to inflammation of the epithelium with evidence of crypt abscesses noted histologically[31,32].This can lead to presentations with pain,increased facial output,and malabsorption due to lack of functionality of the cells.Chronic side effects can also include pain and malabsorption due to chronic inflammation and tissue fibrosis.As with other tissue,severity is dose and tissue-type related; acute symptoms can occur with doses from 5-12 Gy[31].Chronic small bowel enteritis is rare in total dosage less than 50 Gy,with a slighter higher dosage tolerance in the colon.
Diarrhea is a commonly anticipated side effect of radiation therapy when targeting tumors in close proximity to the small bowel.This has multiple underlying etiologies including protein losing enteropathy,malabsorption,or bacterial overgrowth[5,6,33].The introduction of drugs such as loperamide or codeine phosphate may provide significant symptomatic relief,slowing intestinal motility in order to enhance gut water absorption[30].Caution should be taken with antimotility agents as this patient group can be prone to obstruction.This may be secondary to stricturing disease,postoperative status,or underlying pathology.
Antibiotics like rifaximin or metronidazole can be used to manage small intestinal bacterial overgrowth resulting from radiation[34].Prompt review to assess clinical effect in these relatively safe agents is advised to allow tailoring of management should the course be unsuccessful in bringing about significant improvement.
Due to involvement of the relatively fixed terminal ileum within the radiation field,type-1 bile acid malabsorption is associated with radiation enteritis in 40%-70% of those undergoing pelvic radiation therapy[35].Bile acid sequestrants like colestyramine and colesevelam are effective treatments for this disorder.
Surgical input should be considered in patients affected by obstructive and fistulizing disease.Conservative techniques such as a low residue diet or complete bowel rest using PN to allow for obstructive symptoms to settle may be employed.This is often a successful treatment,however the use of PN may be prolonged[36].Operative intervention may be unavoidable in around one third of patients who have chronic radiation enteritis[37].This may include division of strictures,resection,and bypass.Within the setting of radiation enteritis,surgery has higher risks of postoperative complications.This includes a higher risk of anastomotic leaks due to friable tissue with compromised healing.The surgery may be extensive due to multiple areas of fibrosis requiring complex resections or repeated operations[6,38].
With or without surgical intervention,intestinal insufficiency or failure can develop.Parenteral means of supporting the patient,who has limited reserves for enteral absorption of nutrients,is a recognized therapeutic approach and may involve nutrition,electrolyte replacement,or hydration[39,40].Home PN may be employed as a long-term option.However,some patients may use this to supplement oral intake and even ultimately resume normal intake[36].Figures from the United States suggest around 3% of home PN is due to the sequelae of radiation enteritis with higher figures noted throughout European studies[30].
RECTUM
Radiation proctopathy can occur acutely with radiotherapy.However,it is now recognized as a long-term side effect.This could be anywhere from 6 mo to many years following cessation of radiation therapy with the median onset around 2 years.Incidence rates range from 5%-20% of patients[41].It can be observed following therapy for a range of primary sites including prostate,cervix,urinary bladder,testes,uterus,rectum,and anus.A cumulative dose of less than 45 Gy is unlikely to cause significant injury,whereas beyond this and particularly above 70 Gy will likely cause significant injury[42].
Acutely,individuals can experience abdominal pain,discharge,tenesmus,diarrhea,incontinence,and rectal bleeding.The introduction of simple pharmacological agents may be enough to settle the majority of clinical features[43].Chronic rectal radiation effects also pose problems with pain,bleeding,tenesmus,diarrhea,and incontinence,but urogenital fistulae and strictures due to underlying tissue fibrosis are additional problems to consider[5,44].
There are multiple endoscopic and pharmacological treatment modalities for radiation proctopathy.Evidence for these numerous modalities continues to be explored robustly with consideration of benefits and drawbacks.Table1 outlines some of the main practices and highlights some of the issues facing the clinician who may manage the condition.
Treatment of rectal bleeding resulting from radiation has been explored in multiple systematic reviews.A 2015 Cochrane review carried out by van de Weteringet al[45]assessed nonsurgical interventions for late radiation proctopathy.Overall,the level of evidence for all studies of bleeding management was low.One moderate grade recommendation was for sucralfate.Sucralfate can be delivered orally or rectally to provide local action at the site of inflammation.Its proposed mechanism of action is both providing a barrier at the site of damaged tissue and encouraging healingviapromoting angiogenesis[45].At follow-up,73%-100% of patients reported improvement of symptoms.This study did note recurrence of symptoms in up to 20% of patients[46].5-aminosalicylic therapy is commonly used for its benefits within inflammatory bowel disease.Data for use within radiation proctopathy is mixed,and there is no strong evidence to recommend it as a treatment modality[45,47,48].
Hyperbaric oxygen therapy (HBOT) is a further medical option for management of rectal bleeding.It is purported to act through increased stimulation of damaged cells and improves the activity of free radicals[49].Recommendation for the use of HBOT is based on data from a 2008 double blind crossover trial carried out by Clarkeet al[50].Evidence suggests a clinical improvement in symptomatology following at least 30 sessions of HBOT[46,51].Bennettet al[52] in 2016 assessed the outcome following administration of HBOT to various areas for late radiation tissue injury.Within this review multiple small studies were assessed to review its benefit,but due to the limited evidence it was not possible to assess the overall improvement with HBOT[52].None of these studies have shown any serious ill effects from HBOT and have noted improved quality of life from bowel specific symptoms[41].
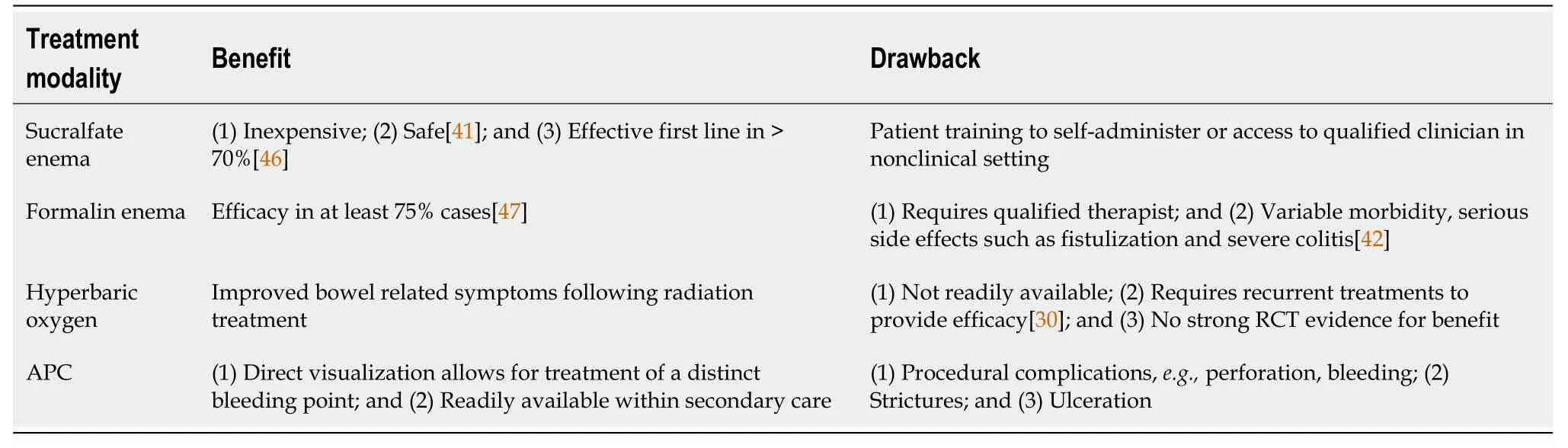
Table1 Treatment modalities for radiation proctopathy and associated bleeding
Hyaluronic acid use for management of the adverse effects of radiation has also been assessed in a 2018 systematic review[53].The studies involved in the review assessed symptomatic improvement in both vaginal symptoms with minimal exploration of rectal symptoms.Formalin application has been shown to have benefit in the management of rectal bleeding[54].Its application to tissue causes sclerosis to the fragile neovasculature.Application methods include a direct “dab” technique or irrigation with an enema.Formalin has been noted to show improvement after a single application,with improvement in bleeding in 90% of patients with 99% after multiple applications.Lower strength 4% formalin shows lower evidence of toxicity compared to 10%,which showed increase adverse effects in follow-up.
Endoscopy is useful for both investigation and management of radiation proctopathy[55].Management of rectal bleeding refractory to medical therapies has been assessed in a recent review by the American Society of Gastrointestinal Endoscopy[56].Over 60 years of reviews and cases were assessed.However,the recommendations are limited by the lack of controlled trials.These findings were also noted in earlier reviews[46,54,57].Various endoscopy modalities,such as argon plasma coagulation (APC),bipolar cautery,and heater probe,and radio-frequency ablation were used for treatment.There was no direct comparison between the endoscopic modalities.APC is a commonly used endoscopic technique and has been shown to be an effective way to treat rectal bleeding,but it does have associated short and long-term complications[58].Repeated treatments may be required to achieve control of bleeding[59].Treatment comparison between formalin and APC suggests formalin application should be used preferentially to APC as it has a lower risk profile.This is from one of the few direct comparison trials[54].Radio-frequency ablation has not been assessedviarandomized controlled trial.However,success has been noted within case series with a low rate of adverse events reported[60-63].From reviews,due to risk profile and lack of randomized controlled trial data the two recommended forms of endoscopic treatment for bleeding are bipolar and APC,with APC being the most efficacious therapy[42].
Endoscopy may also be required to dilate rectal strictures due to radiation.A relatively simple endoscopic treatment with significant benefit to patients with relief of obstructive symptoms.It does have an associated risk of perforation as with other dilation procedures.Limited information exists for lower GI radiation strictures with more information available for its use in esophageal structuring[42,47].Surgical management needs to be considered in those patients with symptoms refractory to medical management.However,due to the invasive nature and associated risks this is reserved to limited cases.One such option for surgical management is a diversion colostomy.
CONCLUSION
Radiation therapy is a mainstay of cancer tre atment that may harbor side effects involving the GI tract (Table2).The treatment of these side effects is heterogeneous,and the outcomes are variable.Multiple small studies and case reports exist.However,few larger ones exist.As technology for providing radiation improves,it is hoped that the side effect burden will lessen,but the increasing population that survive cancermay pose a legacy effect.Acute symptoms may necessitate dose reduction or a cessation in treatment.Conservative measures should be employed where possible.Similarly,with the chronic effects of radiation,medical therapies should be considered as a first line with surgery reserved as a last resort.
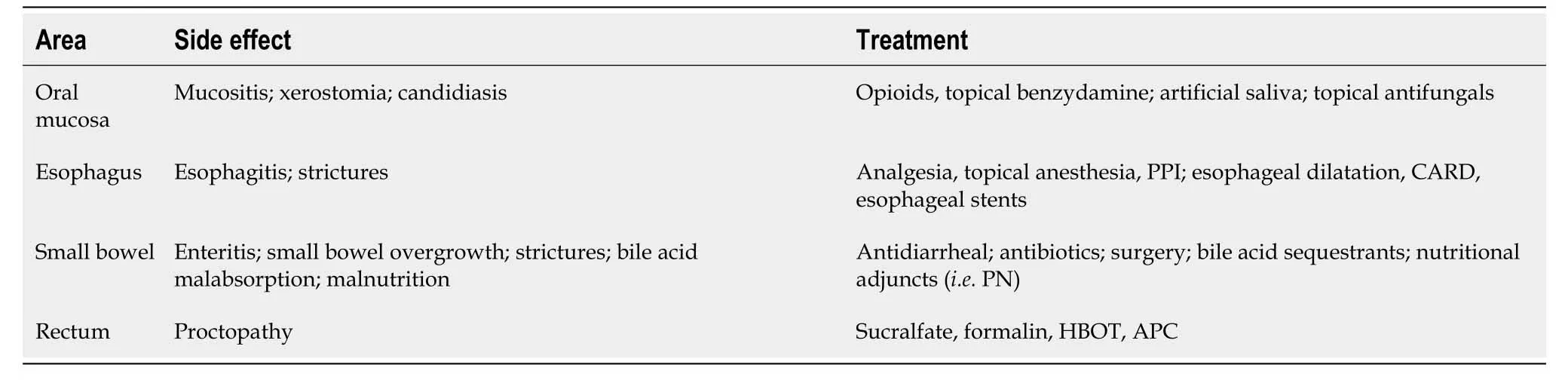
Table2 Overview of specific therapies for side effects associated with radiation therapy
 World Journal of Gastrointestinal Oncology2021年5期
World Journal of Gastrointestinal Oncology2021年5期
- World Journal of Gastrointestinal Oncology的其它文章
- Hypoxia and its impact on the tumour microenvironment of gastroesophageal cancers
- Liquid biopsy in cholangiocarcinoma:Current status and future perspectives
- Biomarkers for hepatocellular carcinoma based on body fluids and feces
- Molecular-targeted therapy toward precision medicine for gastrointestinal caner:Current progress and challenges
- Outcomes of curative liver resection for hepatocellular carcinoma in patients with cirrhosis
- Sex as an effect modifier in the association between alcohol intake and gastric cancer risk