
Biomarkers for hepatocellular carcinoma based on body fluids and feces
2021-05-20 08:24:16
Ming-Cheng Guan,Wei Ouyang,Na Li,Ting-Ting Fu,Hong Zhu,Department of Medical Oncology,The First Affiliated Hospital of Soochow University,Suzhou 215006,Jiangsu Province,China
Ming-Da Wang,Feng Shen,Wan-Yee Lau,Tian Yang,Department of Hepatobiliary Surgery,Eastern Hepatobiliary Surgery Hospital (Navy Medical University),Second Military Medical University,Shanghai 200438,China
Lei Liang,Qiu-Ran Xu,Dong-Sheng Huang,Tian Yang,Department of Hepatobiliary,Pancreatic and Minimal Invasive Surgery,Zhejiang Provincial People’s Hospital (People’s Hospital of Hangzhou Medical College),Hangzhou 310000,Zhejiang Province,China
Lei Liang,Qiu-Ran Xu,Dong-Sheng Huang,Tian Yang,Key Laboratory of Tumor Molecular Diagnosis and Individualized Medicine of Zhejiang Province,Hangzhou 310000,Zhejiang Province,China
Wan-Yee Lau,Faculty of Medicine,The Chinese University of Hong Kong,Hong Kong,China
Abstract Novel non-/minimally-invasive and effective approaches are urgently needed to supplement and improve current strategies for diagnosis and management of hepatocellular carcinoma (HCC).Overwhelming evidence from published studies on HCC has documented that multiple molecular biomarkers detected in body fluids and feces can be utilized in early-diagnosis,predicting responses to specific therapies,evaluating prognosis before or after therapy,as well as serving as novel therapeutic targets.Detection and analysis of proteins,metabolites,circulating nucleic acids,circulating tumor cells,and extracellular vesicles in body fluids (e.g.,blood and urine) and gut microbiota (e.g.,in feces) have excellent capabilities to improve different aspects of management of HCC.Numerous studies have been devoted in identifying more promising candidate biomarkers and therapeutic targets for diagnosis,treatment,and monitoring responses of HCC to conventional therapies,most of which may improve diagnosis and management of HCC in the future.This review aimed to summarize recent advances in utilizing these biomarkers in HCC and discuss their clinical significance.
Key Words:Hepatocellular carcinoma; Biomarker; Blood; Urine; Feces; Gut microbiota
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most frequently diagnosed malignancy of the liver,ranking as the fourth leading cause of cancer-related mortality worldwide[1].Despite significant advances in diagnostic methods,surgical procedures,and new treatments,overall survival (OS) of HCC patients remains dismal,with a 5-year survival of less than 18%.The bad prognosis is largely due to late diagnosis,a high rate of intrahepatic metastasis at the time of diagnosis,and poor responses to conventional therapies[2].At present,diagnosis of HCC is mainly based either by histopathological studies or imaging findings.In recent years,there is still a high but an unmet need for a safe,effective,and non-invasive approach for diagnosing early HCC,predicting responses to specific therapies,evaluating prognoses before or after therapies,and developing new therapeutic targets for this tumor.The emergence of liquid biopsy and omics-related techniques has increasingly made significant progression in discovering such biomarkers.Furthermore,screening tests using body fluids or feces can be used in early disease detection,with the advantages of quick and easy extraction,stability,good cost-effectiveness,and non- or mini-invasive accessibility when compared with traditional screening methods.
Thus,to be able to identify novel non-invasive biomarkers is of paramount importance not only for HCC diagnosis,but also for evaluating prognosis of patients before and after therapy,monitoring responses to therapy,and predicting recurrence.All these can eventually lead to developments of improved therapeutic regimens with better management results in HCC patients.In this review,the recent and important developments on diagnostic biomarkers of HCC from blood,urine,and feces,including proteins,metabolites,circulating nucleic acids,circulating tumor cells(CTCs),extracellular vesicles (EVs),and gut microbiota,and their clinical significances were reviewed (Figure1).
BLOOD-BASED BIOMARKERS
With recent developments in liquid biopsy and omics-based techniques,several bloodderived biomarkers for HCC diagnosis and management over the past several years have been identified.This section focuses on the therapeutic strategies in targeting EVs and the capability of CTCs as potential prognostic or predictive biomarkers for HCC(Table1).
Proteins
The most investigated biomarkers for HCC diagnosis are alpha-fetoprotein (AFP),lens culinaris agglutinin-reactive fraction of AFP (AFP-L3),des-gamma-carboxyprothrombin (DCP),glypican-3,dickkopf-1,Golgi protein 73,osteopontin,and midkine.AFP interacting with other proteins is involved in glucose metabolism,apoptosis,cytoskeleton,and translation in HCC cells,suggesting AFP may be related to malignant characteristics of HCC[3].AFP is still the most widely accepted serological biomarker for HCC diagnosis,monitoring responses to therapy,surveillance of post-treatment recurrence,and predicting long-term survival outcomes.
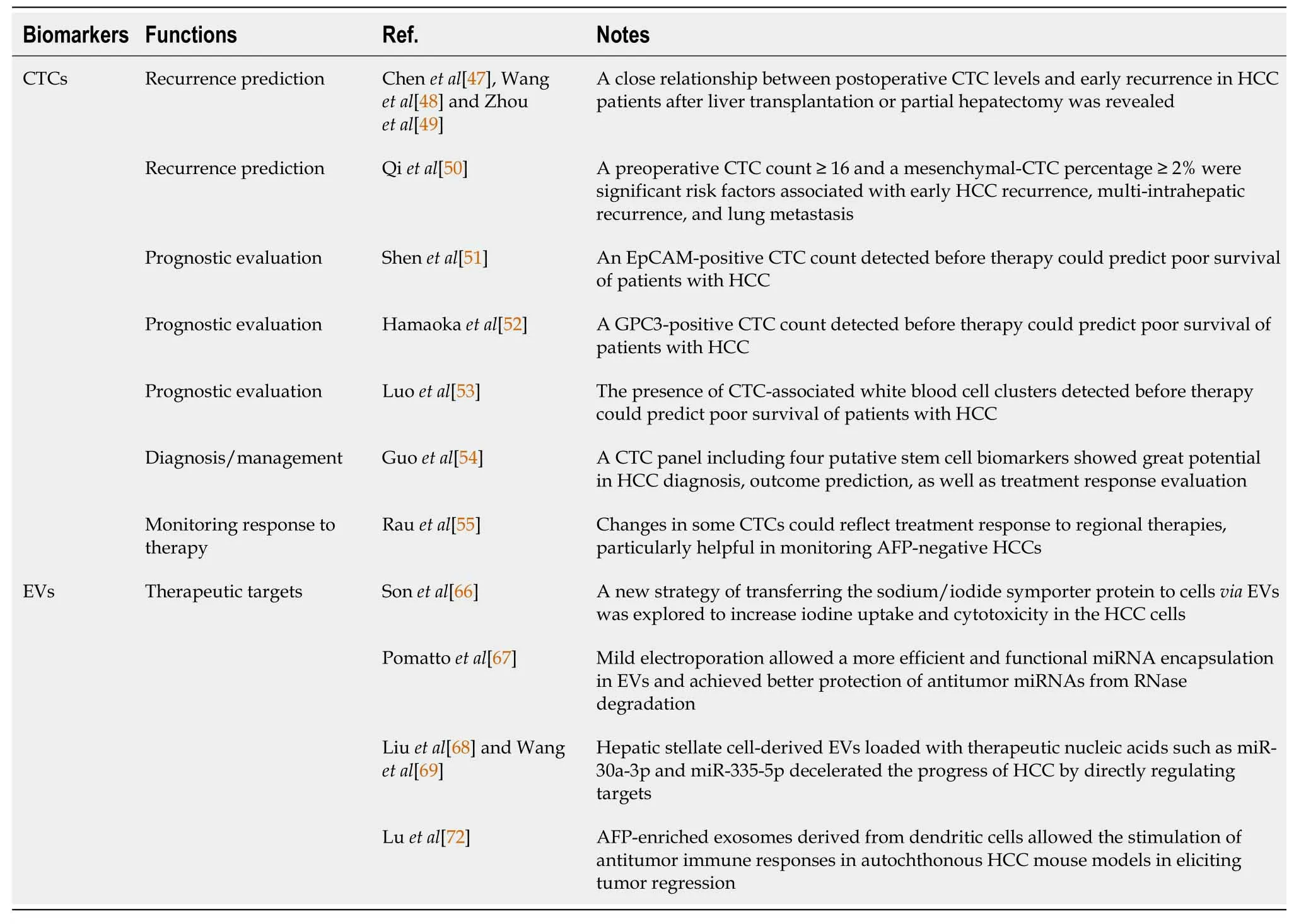
Table1 The major values of circulating tumor cells and extracellular vesicles for management of hepatocellular carcinoma
However,according to the clinical practice guidelines from the European Society for Medical Oncology and the American Association for the Study of Liver Diseases[4,5],it is ultrasound but not serum AFP that is recommended as a routine HCC surveillance tool for cirrhotic individuals.Nevertheless,a meta-analysis revealed serum AFP,when combined with ultrasonography,significantly improved the detection rate of HCC in clinical practice[6].Given the marked variations in sensitivity and specificity of using AFP alone in HCC detection,a combination of AFP with other parameters (e.g.,DCP,sex,and age) is expected to improve the early diagnostic rates of HCC.Three diagnostic prediction models (i.e.,the GALAD model[7],the ASAP model[8],and the HES algorithm[9]) have been developed to provide excellent diagnostic performance for HCC patients.To detect Barcelona Clinic Liver Cancer (BCLC) stage 0-A HCC,the GALAD model,which integrates age and gender into an algorithm based on serum AFP,AFP-L3,and DCP levels,had an area under curve of 0.92 with 92% sensitivity and 79% specificity at a cut-off of -1.18[7].The ASAP model,which incorporates age,sex,serum AFP,and DCP levels,was reported to have a sensitivity of 73.8% and specificity of 90.0% for Barcelona Clinic Liver Cancer stage 0-A HCC[8].The HES algorithm,including current AFP level,rate of AFP change,alanine aminotransferase level,platelet count,age,and etiology of cirrhosis,was able to identify early-stage HCC 6 mo prior to ultimate diagnosis,with 51.20% sensitivity and 90.00% specificity,compared with 46.02% sensitivity for AFP alone (P= 0.0015)[9].

Figure1 Multiple molecular biomarkers derived from blood,urine,and feces,including proteins,metabolites,circulating nucleic acids,circulating tumor cells,extracellular vesicles,and gut microbiota,have great potential to diagnose early hepatocellular carcinoma,predict responses to specific therapies,evaluate prognoses before or after therapies,and be developed as new therapeutic targets for this tumor.P:Proteins; M:Metabolites.
Mounting evidence has been reported in the past several years on the usage of AFP in prognostic and recurrence prediction of HCC.While serum AFP levels at diagnosis have prognostic values on treatment results,an AFP response as defined by a decrease in AFP level after therapy has also been demonstrated to predict tumor recurrence and survival outcomes after liver resection or transarterial chemoembolization for HCC[10,11].Furthermore,an early AFP response has been shown to be associated with improved therapeutic effects of immune checkpoint inhibitors or antiangiogenic therapy for advanced HCC[12].A multicenter retrospective study noted that a decrease in perioperative serum AFP might be an independent risk factor for prognosis in HCC patients after liver resection[13].Patients who had a daily decrease of AFP by more than 9% had significantly better OS and recurrence-free survival (RFS)outcomes.
Development of new models in predicting survival and/or recurrence outcomes has recently been reported.Wanget al[14] constructed RFS- and OS-predictive nomograms based on AFP and six clinical variables that exhibited accurate values in predicting postoperative recurrence and OS for patients with hepatitis B virus (HBV)-related solitary HCC ≤ 10 cm.Chanet al[15] recruited 3903 patients after partial hepatectomy from six centers to develop pre- and post-surgical models based on serum AFP levels and other parameters in predicting early recurrence of HCC after liver resection.These models can help to identify patients with high risks of early recurrence,and they have been externally validated using international cohorts.Another reported study on a model allowed accurate preoperative risk stratification for early recurrence in patients with HBV-related HCC after deceased donor liver transplantation[16].In addition,two scoring models based on serum levels of bilirubin,albumin,AFP-L3,AFP,and DCP at the time of diagnosis of HCC correlated well with HCC staging and prognostication of survival[17].Meanwhile,close correlations between the peak preoperative AFP level and a total tumor volume ratio of > 20 with HCC recurrence have been demonstrated,thus providing another novel predictor for tumor recurrence[18].
Metabolites
The liver is known to be the main organ for detoxification,hormone production,and metabolism of carbohydrates,fats,and proteins,which are essential to maintain homeostasis of the internal environment.Metabolomics,a newly developed postgenomics field,has gradually played increasingly important roles in HCC diagnosis,recurrence prediction,and prognostic evaluation.
A recent prospective observational cohort study revealed that metabolic perturbations occurred before HCC diagnosis,and it identified 46 metabolites to be associated with hepatocarcinogenesis[19].Another study demonstrated remarkable changes from chronic HBV infection to HCC in amino acid and lipid metabolisms[20].Several metabolite panels have been developed to diagnose early HCC; for example,a fivemetabolite panel that included methionine,proline,ornithine,pimelylcarnitine,and octanoylcarnitine was constructed as a diagnostic tool for early detection of HCC[21].Another panel that consisted of serum phenylalanyl-tryptophan and glycocholate performed excellently for early diagnosis of HCC in high-risk populations[22].
Recent evidence has also pinpointed a positive association between dysregulated metabolism detected at an early stage of stereotactic body radiotherapy for HCC with subsequent radiation-triggered liver damage and tumor response[23].Furthermore,an effective nomogram based on preoperative plasma metabolomics profiling was able to predict the risk of HCC recurrence after liver transplantation,thus optimizing candidate selection for transplantation[24].Another study on a scoring system,which included phenylalanine and choline,could be used as an adjuvant tool to stratify patients who could benefit most from curative resection[25].
Circulating nucleic acids
Circulating nucleic acids are a group of extracellular deoxyribonucleic acid (DNA) or ribonucleic acid (RNA) fragments that are shed into peripheral bloodviaany moribund cells to include circulating cell-free DNAs (cfDNAs) and circulating noncoding RNAs (ncRNAs).
Circulating tumor DNA (ctDNA) belongs to a small fraction of cfDNA that derives from tumor cells.In general,the cfDNA levels in peripheral blood-streams from cancer patients are much higher than those in healthy individuals[26].ctDNA has emerged as a potential liquid biopsy biomarker for HCC diagnosis,monitoring,and management because it carries multiple tumor-specific genetic or epigenetic variation information.To date,plenty of tumor-specific genetic and/or epigenetic alterations in cfDNA have been identified as diagnostic and predictive biomarkers for HCC.Among them,testing DNA methylation profiling of ctDNA has the most promising potential to function as an approach for early detection of HCC[27].Several novel panels based on blood methylated DNA markers have recently been developed to yield optimal sensitivity in discriminating early-stage HCC[28,29].In addition,a growing amount of literature showed that TP53 R249S mutation[30],telomerase reverse transcriptase gene promoter mutations[31],and MutL homolog 1 single-nucleotide variant[32] in ctDNA were closely associated with overall prognosis of HCC patients.Other studies also revealed that mutations in ctDNA could dynamically reflect tumor burden in HCC patients,thus improving the estimations in prognostic risks and evaluation of therapeutic responses[33-35].Interestingly,a recent study reported that mutations in phosphoinositide-3 kinase/mammalian target of rapamycin signaling were significantly correlated with a shorter PFS outcome after tyrosine kinase inhibitors treatment,but not with immune checkpoint inhibition,suggesting possible involvement of this pathway in chemoresistance to sorafenib[36].
On the other hand,overwhelming evidence has manifested the roles of ncRNAs in diagnosis and management of HCC.Growing attention has been paid to micro-RNAs(miRNAs) that have about 20 nucleotides in serving as new biomarkers for HCC diagnosis.Although the diagnostic performances of mirR-125b[37],miR-122[38,39],and miR-21[40] have been estimated in a lot of studies,their clinical values still require to be validated.Other novel biomarkers like miR-22[41] and miR-3197[42] have also been identified to be useful in diagnosing HCC.A combination of several miRNAs has been shown to have a great potential in enhancing the diagnostic value of HCC[43].Furthermore,in clinical settings,different miRNAs can be used to function as potential prognostic biomarkers for different selected groups of HCC patients[44].
CTCs
CTCs are a crowd of scattered seed cells that invade from primary tumors into the circulatory system.Significant advancements of its utilization have been achieved in the last decade.Representatively,the CellSearch System (Veridex),based on the expression of epithelial cell adhesion molecules (EpCAM),enables detection of CTCs from the blood-stream in patients with breast,prostate,or colorectal cancers,and it has been approved for clinical use by the United States Food and Drug Administration[45].Detection of CTCs presents a great potential in facilitating management of HCC patients,especially in recurrence prediction and prognostic evaluation.
For HCC diagnosis,a systematic review showed presence of CTCs to have only a modest sensitivity of about 60%,but a high specificity of > 90%[46].For prognostic/predictive biomarkers,CTCs have become the most extensively studied for liquid biopsy.Recent studies have revealed a close relationship between postoperative CTC levels with early recurrence in HCC patients after liver transplantation[47,48] or partial hepatectomy[49].Also,the association of preoperative CTC counts in HCC patients with microvascular invasion has been documented in a recent study[49].Another study reported that a preoperative CTC count of ≥ 16 and a mesenchymal-CTC percentage of ≥ 2% to be significant risk factors associated with early HCC recurrence,multi-intrahepatic recurrence,and lung metastasis[50].Moreover,an EpCAM-positive CTC count[51],a glypican-3-positive CTC count[52],and presence of CTC-associated white blood cells clusters[53] before therapy predicted poor survival of patients with HCC.Guoet al[54] investigated the ability of CTC with stem-like phenotypes in diagnosis and prognostic evaluation for patients with HBV-related HCC.A CTC panel comprising of EpCAM,CD90,CD133,and CK19 allowed discrimination of patients with HCC from those with chronic hepatitis B infection,liver cirrhosis,and benign liver diseases,as well as in identifying early-stage and AFPnegative HCCs.In addition,the relationship between CTC loads and postoperative recurrence was established,indicating the promising role as a real-time tool for risk prediction and treatment monitoring.Also,changes in some CTCs have been reported to reflect treatment responses to regional therapies,and they were particularly helpful in monitoring patients with AFP-negative HCCs[55].
EVs
EVs,including exosomes and microvesicles,are small vesicular bodies with phospholipid bilayer membrane structures that are secreted into peripheral bloodstream by various cells[45].As multiple molecules,including RNA,DNA,and surface protein markers,are capsulized in EVs,they are protected by specific membrane structures against degradation of enzymes[56].
Currently,most studies on EVs as diagnostic markers for HCC are mainly focused on diagnostic performance of ncRNAs derived from EVs.Accumulating evidence has shown that the serum EV-derived ncRNAs including long ncRNA (lncRNA)LINC00853[57],miRNA-10b-5p[58],and miRNA-4661-5p–based panel[58],which participated in pathogenesis of HCC,can serve as novel diagnostic markers for earlystage disease.However,their diagnostic performances are not superior to CTCs or cfDNA,partly because of high degrees of heterogeneity among different studies[46].Besides,exosomal miRNA-224[59] and lncRNAs ENSG00000258332.1 and LINC00635[60] have been reported to be potential diagnostic and prognostic biomarkers for HCC.Another study further elucidated the functional roles of these biomarkers in HCC progression[61].High circulating levels of exosomal miRNA-21 (≥0.09) and lncRNA-ATB (≥ 0.0016) in HCC patients have been found to associate with poor OS and PFS outcomes.Another study also revealed that a circulating exosomal lncRNA panel could predict recurrence and metastasis of HCC[62].
EVs,as significant intermediaries undergoing intercellular exchange of information and substances,maintain normal physiological functions and are involved in development and progression of cancers[63].Upon arriving at target cells,EVs can be absorbed by host cells,or dwell on their cytomembrane through mutual recognition,then activate downstream signaling pathways or transmit cargos intracellularly[63,64].Increasing studies have investigated the use of EVs in treating cancers,including HCC.EVs have been re-engineered in structures to transport and deliver specific therapeutic agents to cancer cells as vehicles in different pathological conditions to improve therapeutic efficacy of anti-cancer drugs and simultaneously to reduce side effects[65].
To increase iodine uptake and cytotoxicity in HCC cells,Sonet al[66] explored a new strategy of transferring the sodium/iodide symporter (NIS) protein to cellsviaEVs.HCC cells (Huh7) were first transfected withNISgene and then collected for isolation of cellular EVs that contained high levels of NIS protein.Treatment of hepatoma cells with these NIS-containing EVs led to enhanced iodine uptake with resultant promotion of cytotoxicity of the radioiodine therapy against cancer cells.Pomattoet al[67] further improved the engineering methods for drug loading of EVs.They found mild electroporation allowed a more efficient and functional miRNA encapsulation in EVs and achieved better protection of antitumor miRNAs from RNase degradation.In addition,EVs loaded with antitumor miR-31 and miR-451a were found to accelerate apoptosis of HCC cells.Moreover,hepatic stellate cell-derived EVs loaded with therapeutic nucleic acids such as miR-30a-3p and miR-335-5p decelerated progression of HCC by directly regulating targets[68,69].Preclinical trials demonstrated the role of EVs in migration,invasion,and metastasis of HCC.Nidogen 1-enriched EVs have been reported to induce pulmonary fibroblasts to secrete tumor necrosis factor receptor 1,resulting in accelerated extrahepatic metastasis[70].Similar findings on the functional role of exosomal miR92a-3p in promoting epithelialmesenchymal transition and metastasis were found by regulating the Akt/Snail signaling pathway[71].Also,AFP-enriched exosomes derived from dendritic cells have been found to allow stimulation of antitumor immune responses in autochthonous HCC mouse models in eliciting tumor regression[72].These recent findings provide the potential for development of new strategies in HCC treatment by either inhibiting EV production or up-taking and injecting immunocyte-derived EVs into patients.
URINE-BASED BIOMARKERS
As non-invasive tools,urine-based biomarkers can provide significant application values on cancers in clinical settings.Advances in omics technologies and computational capabilities in the past several decades have helped to identify multiple potential urinary biomarkers,including proteins,metabolites,and nucleic acids,for HCC diagnosis and prognosis evaluation (Table2).
Elevation of 8-oxodeoxyguanosine levels enhances repair of oxidative DNA damage with reduction in risks of developing HCC while increased 15-F2t-isoprostane levels are related to increased risks of HCC.Wuet al[73,74] investigated the role of oxidative stress and aflatoxin exposure on the risk of HCC by using a community-based cohort in Taiwan and demonstrated that both elevated levels of urinary 8-oxodeoxyguanosine(a biomarker of oxidative DNA damage) and urinary 15-F2t-isoprostane (a biomarker of lipid peroxidation) were associated with increased levels of aflatoxin exposure.A Shanghai Cohort Study by Yuanet al[75] identified 8-epi-prostaglandin F2α,a known indicator of oxidative stress,as a biomarker that can stratify individuals without traditional risk factors for HCC development into a high- and a low-risk group.Another study linked high urinary levels of 8-hydroxy-deoxyguanosine (another indicator of oxidative DNA damage) to genetic polymorphisms of two major DNA repair enzymes (XRCC1 rs25487 G/A and OGG1 rs1052133 C/G) in patients with chronic hepatitis C virus (HCV) infection and HCV-related HCCs and concluded that the urinary 8-hydroxy-deoxyguanosine level to be a promising non-invasive biomarker in HCV-related hepatocarcinogenesis[76].Taken together,these biomarkers can be used to facilitate HCC prevention and progression monitoring.
Urinary proteins,metabolites,and nucleic acids have been identified to be useful in detecting HCC.Such proteins include urinary DJ-1,chromatin assembly factor-1 (CAF-1),Heat Shock Protein 60,AFP,and orosomucoid 1[77,78].CAF-1 exhibited the best performance in discriminating HCC in HCV patients,with a specificity of 90%,sensitivity 66%,and diagnostic accuracy 78%[77].Another study showed no significant difference between the diagnostic performance of urinary and serum AFP levels[78].Urinary proteomic profiling has identified seven urinary protein features that have been validated by targeted Multiple Reaction Monitoring to yield excellent performance in discriminating HCC from high-risk populations[79].Ladepet al[80]evaluated the diagnostic performance of a panel of urinary metabolites comprising of inosine,indole-3-acetate,galactose,and N-acetylated amino acid in a West African cohort.This panel showed a sensitivity of 86.9% and a specificity of 90.3% in discriminating HCC from cirrhosis; and eight metabolites that were significantly increased in the urine of HCC patients correlated with their clinical HCC stages.Other panels comprising of urinary metabolites also displayed favorable diagnostic capability in distinguishing HCC from cirrhosis[81,82].Furthermore,urinary miRNA (i.e.miR-618 and miR-650)[83] and nucleosides (i.e.adenosine,cytidine,and inosine)[84] were able to serve as additional diagnostic biomarkers when combined with AFP serology.These findings show the ability of these tests to facilitate HCC diagnosis and surveillance in a non-invasive manner.
During treatment of HCC,changes in levels of urinary biomarkers have been shown to predict tumor recurrence.Overexpression of the urinary trypsin inhibitor in HCC was found to be a risk factor for HCC recurrence after partial hepatectomy[85].Other reports on metabolites,including ethanolamine,lactic acid,acotinic acid,phenylalanine,and ribose,were shown to be effective predictors for early HCC recurrence after surgery[86].
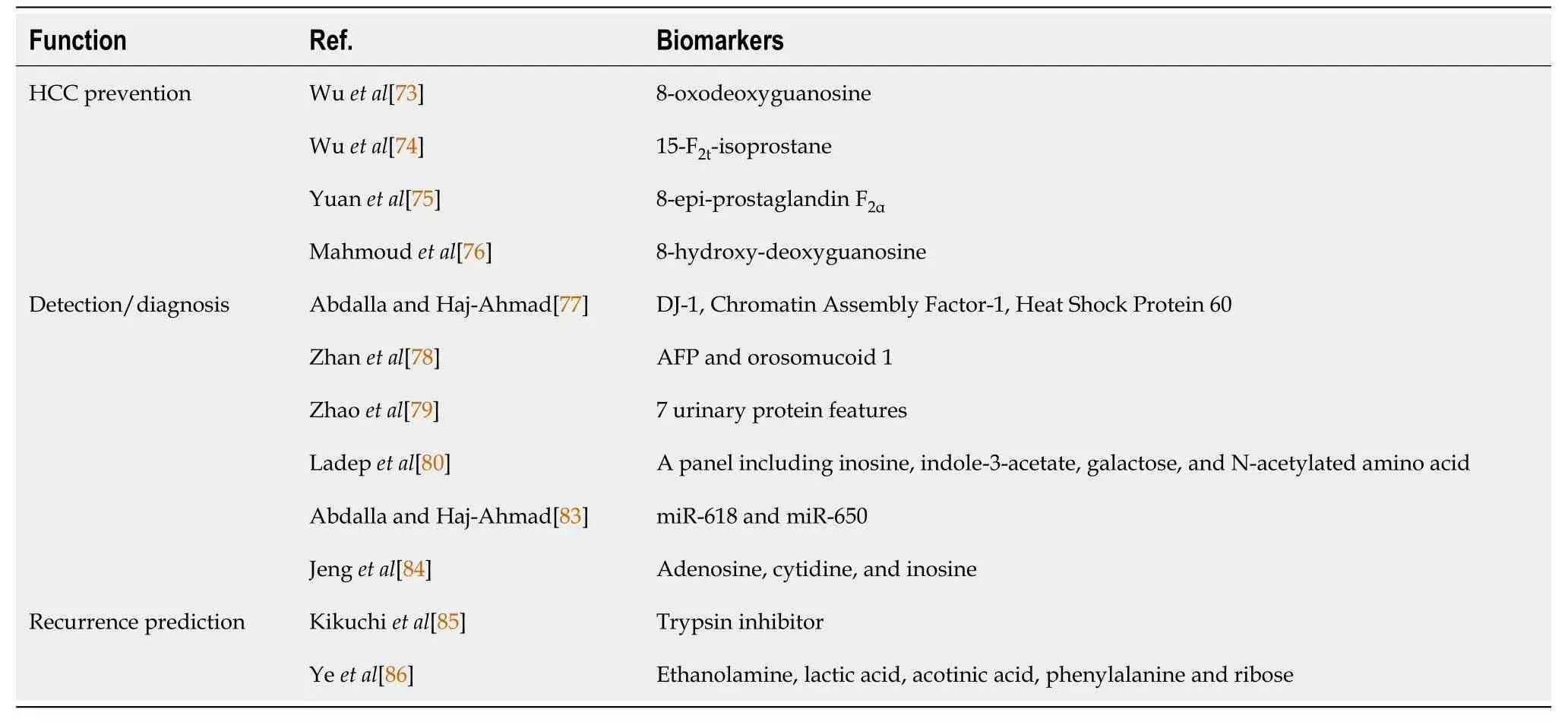
Table2 Multiple potential urinary biomarkers used for hepatocellular carcinoma prevention,diagnosis,and recurrence prediction
FECES-BASED BIOMARKERS — GUT MICROBIOTA
The gut microbiota exerts essential functions in maintaining homeostasis in a human body.It is involved in direct or indirect regulation of key processes in mammalian metabolism,immune tolerance,and immunocompetence[87].Growing preclinical studies have revealed involvement of gut microbiome in liver carcinogenesisviathe gut-liver axis,mainly through exacerbations of inflammation and accumulations of harmful compounds[88].Thus,disordered intestinal flora can be used for non-invasive diagnostic,prognostic,and therapeutic targets for HCC (Table3).
Renet al[89] first validated the potential of gut microbiome as non-invasive tools for early diagnosis of HCC.A decrease in fecal microbial diversity was observed from healthy to cirrhotic individuals,while an increase was detected from cirrhotic individuals to patients with early-stage HCC with cirrhosis.Besides,bacterial genera generating butyrate were decreased,while lipopolysaccharide-yielding genera were increased in patients with early HCC when compared with healthy individuals.Remarkably,a selected panel of 30 optimal gut microbial markers showed a powerful diagnostic performance for early HCC,achieving an area under the curve of 80.64%between a group of 75 patients with early HCC and a group of 105 non-HCC subjects.Lapidotet al[90] also recently revealed changes in gut microbiota in individuals with progression of cirrhosis to HCC and the associations among diet,lifestyle,and microbiome.In addition,an association between excess weight and increased dysbiosis in HCC patients was noted.Environmental factors leading to fatty liver,consumption of artificial sweeteners,and high-sugar foods were significantly associated with alternations in microbiota of cirrhotic patients with HCC.Moreover,an increase ofClostridiumandCF231but a decrease inAlphaproteobacteriain patients with cirrhosis with HCC were found when compared to those without HCC.All these changes were independent of severity of cirrhosis and dietary habits.Future studies recruiting more populations from different regions with diverse underlying diseases are urgently needed for verification of these findings.
There is more evidence supporting the importance of gut microbiota in HCC patient management.Zhenget al[91] compared taxa richness and gene counts of fecal samples from HCC patients who were sensitive to immunotherapy with non-responders and found that gut microbiota could influence the response to anti-programmed cell death protein 1 immunotherapy.This information is critical for treatment decision-making and disease management.As for evaluation of prognosis,a study identified six microbial biomarkers to be related to the tumor immune microenvironment or to bile acid metabolisms[92].These biomarkers had a potential to predict clinical outcomes.In day-to-day clinical practice,overuse of antibiotic drugs can result in disorder and disturbance of gut microbiota.A study revealed the association of gut flora and antibiotics with prognosis of liver cancer patients after chemotherapy[93].Intestinalanaerobic bacteria,includingBlautia,were reported in this study to be associated with more favorable prognosis in these patients,but usage of anti-anaerobic drugs had poorer prognosis.Thus,modulation of gut microbiota using antibiotics is a promising strategy to intervene development or progression of HCC.In addition,use of probiotics in murine HCC models inhibited HCC development,suggesting this strategy might have a potential to be used as a therapeutic option for HCC patients in the future,provided that alterations of gut microbiota by certain probiotics could also be observed in human[94].Another viable way to regulate human gut microbiome is through fecal microbiota transplantation,but such studies remain under-investigated.
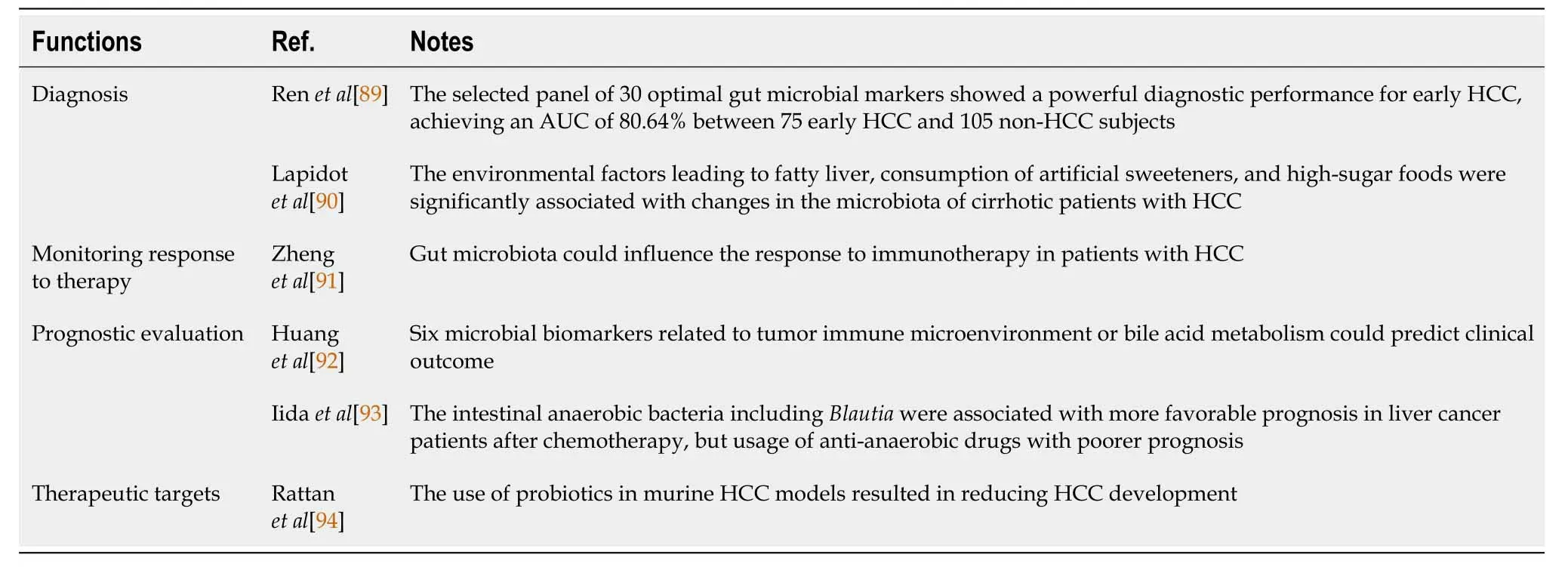
Table3 The diagnostic,prognostic,and therapeutic values of gut microbiota
CONCLUSION
In this review,advanced developments for HCC in biomarkers derived from body fluids and feces,including proteins,metabolites,circulating nucleic acids,CTCs,EVs,and gut microbiota,were summarized.These biomarkers or their panels have the potential values in diagnosis,monitoring responses to therapy,recurrence prediction,and prognostic evaluation of HCC.
As for blood-based biomarkers,despite wide utilization of AFP,AFP-L3,and DCP in most countries,the sensitivity of a single biomarker for the early diagnosis of HCC is relatively low.In turn,those diagnostic models (e.g.,the GALAD model,the ASAP model,and HES algorithm) have satisfactory diagnostic performance,which not only facilitates early detection of HCC in high-risk populations but also avoids undue healthcare costs.These models need to be further optimized and validated in different countries and different populations before widely applied in clinical practice.With the approval of miRNA7™ molecular diagnostic kit for HCC diagnosis and therapeutic monitoring in China,liquid biopsy,especially cfDNA methylation and miRNA test,has a good application prospect in the diagnosis of HCC.However,the maturity of related technology,cost reduction,and the establishment of internationally recognized reference standards are required to ensure early clinical application.At present,imaging examination is routinely used for prognosis evaluation and post-treatment monitoring around the world,but computed tomography or magnetic resonance imaging combined with serum AFP or DCP test is recommended as a regular followup examination strategy after HCC treatment according to Chinese,Japanese,and other clinical practice guidelines.Besides,EVs with specific therapeutic agents to liver cancer cells are regarded as a novel therapeutic method for HCC.The mechanism of EVs arrival at and uptake by target cells needs to be further investigated,and these findings fromin vitroexperiments are urgently needed to be verified in animal models due to complicated internal environment.
As to urinary biomarkers,multiple protein,metabolite,or nucleic acid changes in urine potentially allow for HCC diagnosis and prognosis evaluation.But in fact,no effective urinary biomarkers for HCC have been applied in clinical practice now,and most of the studies are still in the exploratory stage.For gut microbiota from feces,whether gut microbiota can be used for early detection of HCC or as a novel therapeutic remedy should be further studied and clarified.
In conclusion,future well-designed multicenter prospective studies on biomarkers for HCC derived from body fluids and feces as well as transformation of the relevant basic research results into clinical application will optimize current strategies of HCC diagnosis and management.
 World Journal of Gastrointestinal Oncology2021年5期
World Journal of Gastrointestinal Oncology2021年5期
- World Journal of Gastrointestinal Oncology的其它文章
- Hypoxia and its impact on the tumour microenvironment of gastroesophageal cancers
- Liquid biopsy in cholangiocarcinoma:Current status and future perspectives
- Molecular-targeted therapy toward precision medicine for gastrointestinal caner:Current progress and challenges
- Update on the management of the gastrointestinal effects of radiation
- Outcomes of curative liver resection for hepatocellular carcinoma in patients with cirrhosis
- Sex as an effect modifier in the association between alcohol intake and gastric cancer risk