
Radiological assessment of extranodal extension in patients with head and neck squamous cell carcinoma
2021-05-11 14:50JanDankbaarFrankPameijer
Jan W. Dankbaar, Frank A. Pameijer
Department of Radiology, University Medical Center Utrecht, Utrecht 3584CX, The Netherlands.
Abstract The prognosis of patients with head and neck squamous cell cancer (HNSCC) decreases with the presence of extranodal extension (ENE) in lymph node metastases. Therefore, ENE was introduced in the 8th Edition TNM Classification (TNM8) for Head and Neck Cancer as a staging variable in all HPV-negative HNSCC. Patients with ENE may benefit from adjuvant or even primary chemotherapy and/or radiotherapy. There is a clear discrepancy between the definition of clinical ENE and pathological ENE. In TNM8, the radiological evaluation of ENE only plays a supportive role. Since not all patients with advanced disease will undergo a neck dissection, histologic proof of ENE will not always be available. In these cases, it would be of great help to be able to accurately determine ENE with radiological imaging. In this review, an update is given of the ability of radiological imaging to identify and grade ENE.
Keywords: Head and neck cancer, extranodal extension, TNM8, radiology, CT, MR
EXTRANODAL EXTENSION
Locoregional recurrences and distant metastases account for the majority of treatment failures in head and neck squamous cell cancer (HNSCC)[1]. The presence of cervical lymph node metastases increased the likelihood of locoregional recurrences and distant metastasis. It is therefore the most accurate prognostic factor in these patients[2,3]. Prognosis further decreases with the presence of extranodal extension (ENE) in lymph node metastases[4-8]. The incidence of ENE varies between 21% and 85%[8]. In a meta-analysis with 1620 patients, the five-year overall survival rate in patients with encapsulated lymph node metastases was 58.1%. In patients with ENE, the survival rate was only 30.7%[8]. A comparative analysis of the EORTC(#22931) and RTOG (#9501) trials showed that addition of concomitant chemotherapy to postoperative radiotherapy seems to improve the outcome of patients with ENE[9,10]. Therefore, ENE was introduced in the 8th Edition TNM Classification (TNM8) for Head and Neck Cancer as an important staging variable in all HPV-negative HNSCC. In TNM8, ENE is clinically defined as follows: skin involvement or soft tissue invasion with deep fixation/tethering to underlying muscle or adjacent structures or clinical signs of nerve involvement supported by radiological evidence. Radiologic evidence alone is not enough for nodal upstaging. ENE is histologically defined as any metastatic tumor cell microscopically extending outside the lymph node capsule. In the above-mentioned trials that identified ENE as a significant prognostic factor for poor outcome, ENE was determined histologically. The extent of ENE was not determined, and it was not mentioned whether patients met the criteria for the clinical definition in TNM8 before lymph node dissection was performed. Intuitively, one would say that the clinical definition of ENE identifies cases with much more advanced disease extension than the histological definition. It has been shown that not only the presence but also the extent of ENE is associated with the presence of distant metastases and adverse prognosis[4-7,11]. In one study evaluating the association between outcome and extent of ENE on histopathology in patients with HNSCC, ENE was graded according to the scale proposed by Lewiset al.[7].In this scale, an extension of 1 mm is used to differentiate minor from more extensive ENE. The results of the study show that dichotomization between “no ENE” and “any ENE” has limited additional prognostic value in the setting of adjuvant chemotherapy and radiotherapy (CRT). Patients with a high grade of ENE with complete replacement of the lymph node by metastatic tumor with no residual lymph node architecture retained a poorer prognosis with regard to overall survival despite CRT. CRT effectively mitigated the difference in prognosis between patients with lower grades of ENE (e.g., ≤ 1 mmvs. > 1 mm)[12]. In TNM8, all lymph nodes larger than 3 cm with histologically determined ENE result in classification N3b. If ENE is clinically evident or if there are multiple metastatic lymph nodes with at least one node with ENE, the node diameter is not taken into account. An extent of more or less than 2 mm was chosen as a cut-off between microscopic and macroscopic ENE[13]. This differentiation does not influence the TNM classification, but it was introduced to collect data to refine the use of ENE in future TNM classifications [Figure 1]. In a study investigating the difference in survival between patients with ENE of ≤ 2 mm or > 2 mm, no difference was found[14]. Patients with both ENE and multiple positive lymph nodes had decreased overall survival compared to patients with a single positive lymph node with ENE. Patients with multiple lymph nodes with ENE had the worst prognosis[14]. In a study subdividing patients into microscopic and macroscopic ENE, there was a consistent trend for worsening survival with increasing degree of ENE[15]. Regarding these findings, it would be of great interest to determine what degree of ENE contributes most to poor prognosis. Patients with poor prognosis due to a high grade of ENE may be candidates for trials investigating novel methods of adjuvant therapy intensification.
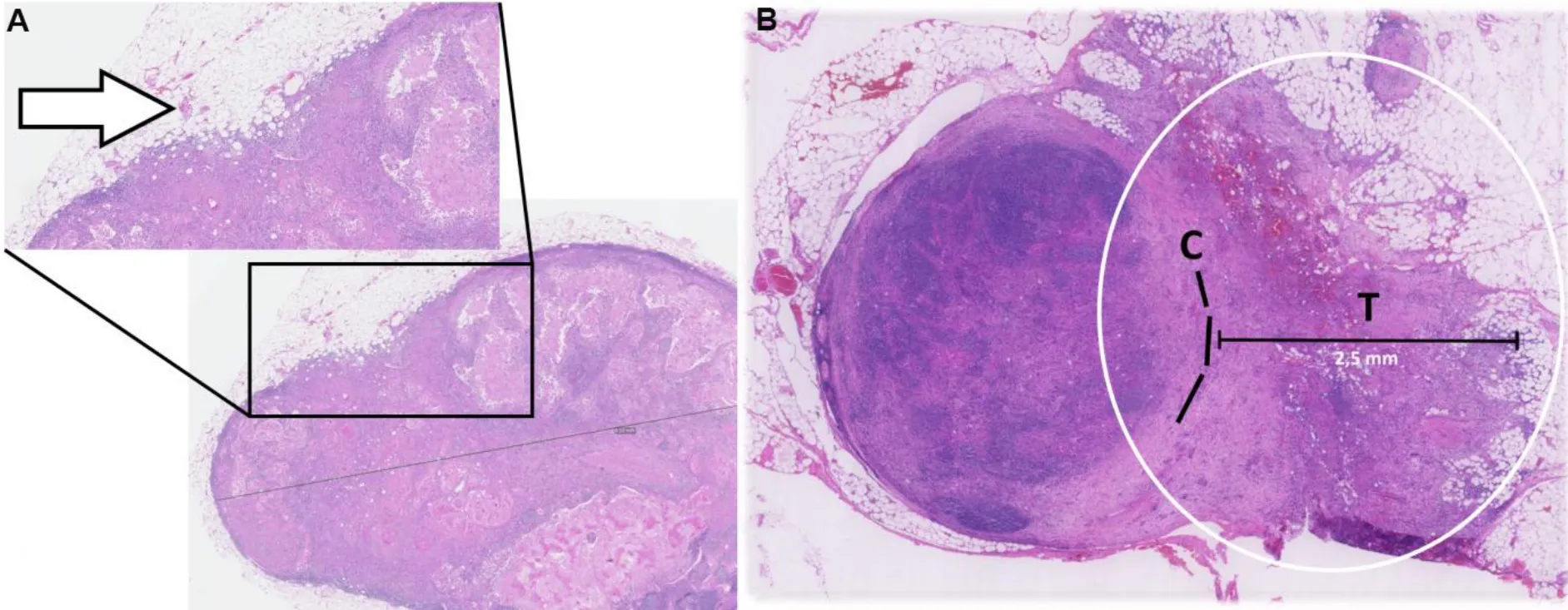
Figure 1. Examples of ENE measurement on hematoxylin-eosin-stained tissue samples of patients with HNSCC: (A) ENE < 2 mm with a small area of capsular disruption and a few malignant cells in the adjacent stroma (arrow); and (B) ENE > 2 mm (circle) as measured from the virtual external capsule border (C) to the farthest extend of the tumor (T).
In daily practice, not all patients with advanced disease will undergo a neck dissection. Histologic proof of ENE will therefore not always be available. In these cases, it would be of great help to be able to accurately determine ENE with radiological imaging. Determining clinically relevant ENE first could greatly improve the contribution of radiological imaging to tumor staging with regards to ENE and thereby primary treatment selection. Although not yet proven, it can be anticipated that the addition of concurrent chemotherapy to primary radiotherapy will also improve locoregional control and survival in patients with ENE.
In the next paragraphs, an update is given of the ability of radiological imaging to identify and grade ENE.
CT EVALUATION OF ENE
The diagnostic performance of contrast enhanced computed tomography (CT) for the detection of ENE has been evaluated most extensively [Figure 2]. Fewer reports are available on the detection of ENE with magnetic resonance imaging (MRI). The imaging features used to radiologically determine ENE are similar for CT and MRI. The most frequently applied imaging features on CT are indistinct or irregular lymph node margins, perinodal fat stranding, absence of perinodal fat planes, nodal necrosis, intranodal cysts,nodal matting, invasion into surrounding structures, lobular contours rather than spherical or oval,inhomogeneous nodal enhancement, size of largest node, and thick-walled, enhancing nodal margins. There is significant overlap among these imaging findings. Invasion of surrounding structures, for example,implies the presence of indistinct margins, perinodal fat stranding, and absence of perinodal fat planes. In addition, nodal necrosis is most likely indistinguishable from intranodal cysts and inhomogeneous nodal enhancement. Clear cut-off points between one feature and the others do not exist. The inter-observer agreement (kappa value) of the CT features varies between 0.1 and 0.83, with central necrosis showing the highest agreement (0.79) and infiltration of adjacent planes the lowest one (0.46). The overall inter-observer agreement for CT varies between 0.37 and 0.91[16-20].
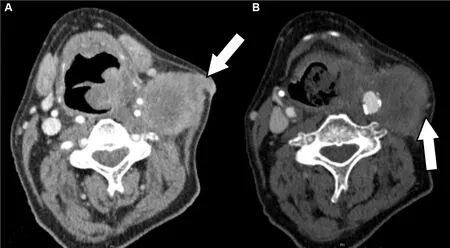
Figure 2. Examples of ENE on CT: (A) macroscopic ENE of a Level 2 lymph node in a patient with HNSCC with invasion of the sternocleidomastoid muscle and subcutaneous fat tissue (arrow); and (B) less extensive (minor) ENE of a Level 2 lymph node in another patient with HNSCC with subtle infiltration of adjacent planes (arrow).
In a recent meta-analysis, the results of 16 CT studies were pooled[16-32]. All these studies compared a blinded CT evaluation of lymph nodes with histological evaluation after lymph node dissection in patients with HNSCC[27]. The pooled sensitivity for the detection of ENE was found to be 0.73 (95%CI: 0.62-0.82). The pooled specificity was 0.83 (95%CI: 0.75-0.89). Two radiological features were pooled separately in a subanalysis. For central necrosis, the pooled sensitivity was 81% (95%CI: 67%-91%) and the pooled specificity 65% (95%CI: 57%-72%). For infiltration of adjacent planes, the pooled sensitivity was 51%(95%CI: 34%-67%) and the pooled specificity 94% (95%CI: 76%-99%). Only one study investigated the difference in the diagnostic performance of CT for different grades of ENE. As expected, the performance of CT, primarily sensitivity and PPV, increased as the grade of ENE increased[28].
MRI EVALUATION OF ENE
The advantage of MRI over CT is the higher soft tissue contrast that can be achieved. Fat planes, subtle enhancement, and especially edema are often better seen on MRI than on CT. However, due to its longer acquisition time, MRI is more prone to movement artifacts. In addition, MR images can be degraded by field inhomogeneities caused by air in the oral cavity, pharynx, and larynx. Therefore, MRI is still less frequently used than CT in the evaluation of patients with HNSCC. As mentioned above, the imaging features that are used to detect ENE with MRI are similar to the features used on CT. In addition to irregular lymph node margins, absence of perinodal fat planes, nodal necrosis, invasion into surrounding structures, and size, T2 hyperintensity in the interstitial tissue around the lymph node is used [Figure 3].The overall inter-observer agreement of MRI varies between 0.5 and 0.76[18,25,33]. In the above-mentioned meta-analysis, the results of nine studies that evaluated MRI for the detection of ENE were pooled[15,18,21,25,27,33-37]. The pooled overall sensitivity for MRI was 60% (95% CI: 49%-70%) and the specificity 96% (95%CI: 85%-99%). Several MRI features were also analyzed separately within some of these studies.One study showed high specificities for infiltration into surrounding structures (100%, with a sensitivity of 50%) and irregular lymph node margins (93%, with a sensitivity of 63%)[36]. Another study showed a specificity of 99% for irregular lymph node margins with a sensitivity of 65%[35]. As with CT, the sensitivity of MRI for ENE is lower with lower grades of ENE on histopathology[25].

Figure 3. Examples of ENE on MR: (A) contrast-enhanced fat saturated T1 image; (B) T2 fat saturated image of a Level 2 lymph node in a patient with HNSCC with minor ENE with subtle enhancement and T2 hyperintensity in the tissue around the lymph node (arrows);(C) contrast-enhanced fat saturated T1; and (D) T2 fat saturated image of a Level 2/3 lymph node in a patient with HNSCC with extensive ENE all the way through the skin (circles).
US EVALUATION OF ENE
In the literature, there is only one study on the use of ultrasound for the detection of ENE in patients with HNSCC. This study, in 110 patients with HNSCC, reports a specificity of 82% and a sensitivity of 79%. The false negative findings were largely caused by microscopic ENE[38]. A study in 29 patients with thyroid cancer evaluated different ultrasound characteristics for their ability to detect ENE. A sensitivity of 64% and a specificity of 89% were found when ≥ 3 ultrasound characteristics were present[39]. Cystic changes in > 50%of a lymph node was the most specific finding of ENE on ultrasound, but with a very poor sensitivity of only 28%. Detection of unclear margins had a specificity of 62% and a sensitivity of 36%.
ARTIFICIAL INTELLIGENCE IN THE EVALUATION OF ENE
To reduce the inter-observer variability of the radiological evaluation of ENE, efforts have been put into the use of automated detection algorithms. In one of these efforts, a deep learning convolutional neural network was trained to identify ENE[24]. The network was trained on a dataset of 2875 CT-segmented lymph node samples with correlating pathology labels. The obtained algorithm predicted ENE with an area under the receiver operating characteristic curve (AUC) of 0.91 (95%CI: 0.85-0.97). In another study, this model was validated in two different hospitals on pretreatment CT imaging in patients with HNSCC[40]. The algorithm achieved an AUC of 0.84 (83.1% accuracy) and an AUC of 0.90 (88.6% accuracy) in the two hospitals. The radiologists who visually evaluated the presence of ENE in this study had significantly lower AUCs of 0.60,0.70, 0.71, and 0.82. The diagnostic accuracy of the radiologists improved when receiving assistance form the detection algorithm. The diagnostic accuracy of MRI is also likely to improve from the use of deep learning methods[41]. With MRI, it is possible to extract a large number of quantitative features (radiomics)from the standard T1 and T2 sequences, contrast enhanced sequences, DWI, and dynamic contrast enhanced sequences. All these features could be used to improve automatic detection algorithms for ENE.In addition, the information from imaging could be combined with genomic and epigenetic markers. It has for example been shown that high-risk TP53 mutations are associated with ENE[42]. Moreover, advances in next generation sequencing and multi-platform genomic and epigenetic characterization of solid tumors may result in an individualized determination of treatment response and prognosis in patients with HNSCC in the future[43-45].
DISCUSSION
As of the introduction of TNM8 in 2017, head and neck surgeons, pathologists, and radiologists are trying to implement the new ENE criteria in daily practice. As described above, there is a large variation in the reported diagnostic performance of both CT and MRI for the detection of ENE. This variation is most likely caused by significant variations in the histological and radiological diagnostic criteria. The histological criteria are not mentioned in the majority of the studies. Furthermore, in most studies that mentioned histological criteria, no difference was made between macroscopic invasion and microscopic ENE in the analysis. With standardized histological criteria and identification of clinically relevant ENE on histology,radiological criteria can be improved. Accurately defining the radiological criteria of clinically relevant ENE and testing the reproducibility of these criteria will improve the applicability in clinical practice and thereby aid treatment decision making. It is likely that automated detection algorithms with the incorporation of MRI radiomics will also benefit from these efforts. We expect refinements of the ENE criteria in the upcoming TNM9. In addition, genomic and epigenetic features are expected to play an increasingly important role in future determination of response and prognosis of patients with HNSCC.
DECLARATIONS
Authors’ contributions
Made substantial contributions to conception and design of the study and performed data interpretation and manuscript drafting: Dankbaar JW, Pameijer FA
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
Both authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2021.
 Journal of Cancer Metastasis and Treatment2021年9期
Journal of Cancer Metastasis and Treatment2021年9期
- Journal of Cancer Metastasis and Treatment的其它文章
- Comparison of immediate vs. deferred cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma
- AUTHOR INSTRUCTIONS