
Calcified Epidermal Cyst on the Neck
2021-04-21 09:17:48JiaQiLvandJianMinChang
国际皮肤性病学杂志 2021年1期
Jia-Qi Lv and Jian-Min Chang∗
Department of Dermatology, Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing 100730, China.
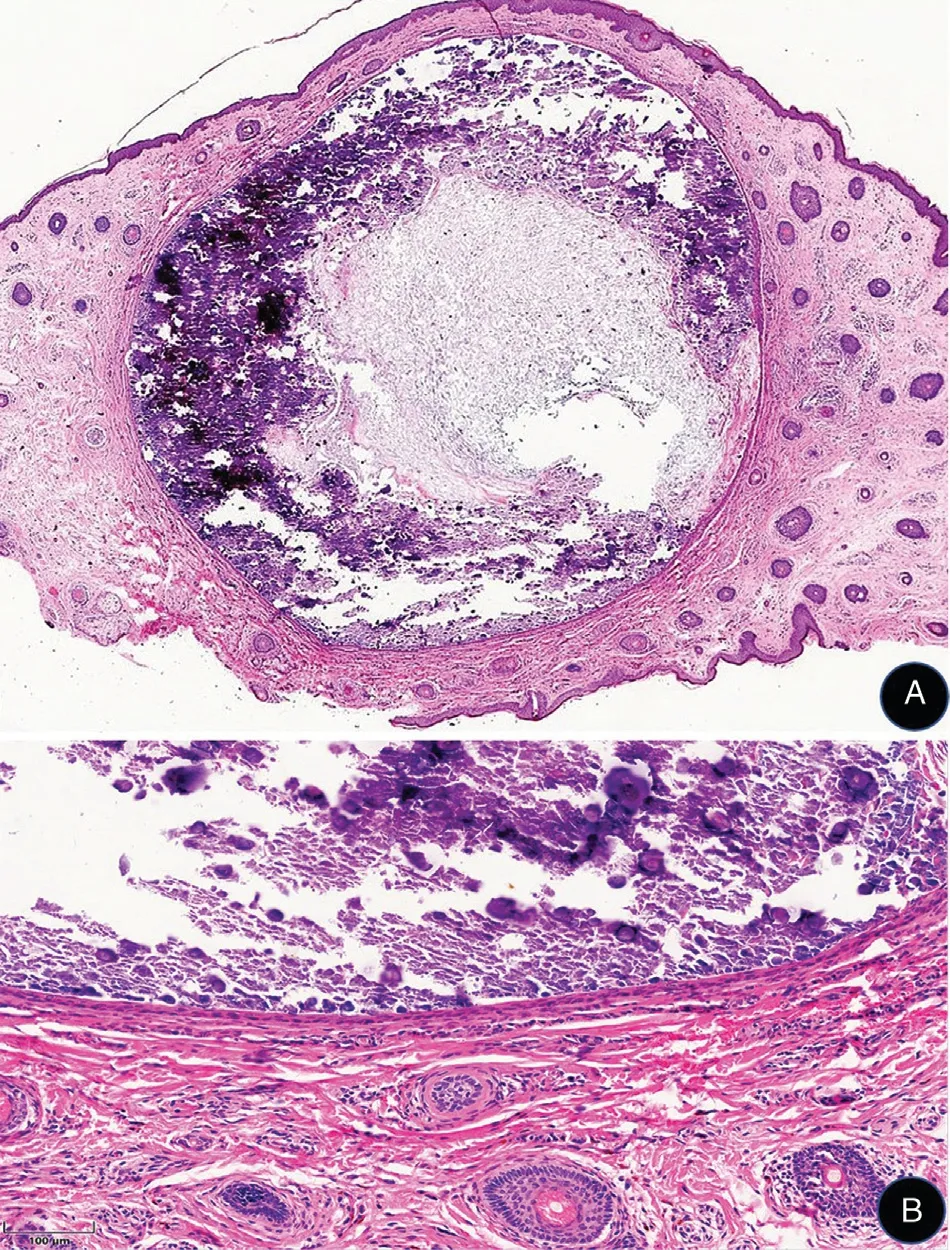
Figure 1. Histological characteristics of the lesion of calcified epidermal cyst on the neck. A: Histological examination reveals a dermal cystic structure. The cavity is filled with keratinous material and numerous amorphous basophilic calcareous sediments (hematoxylin-eosin staining, ×20). B: The cyst wall consists of thinned stratified squamous epithelium surrounded by fibrosis (hematoxylin-eosin staining, ×200).
Histopathology
Histological examination of a calcified epidermal cyst reveals a dermal cystic structure. In addition to laminated layers of keratinous material, the cavity is filled with amorphous basophilic calcareous sediment (Fig. 1A). The cyst wall consists of thinned stratified squamous epithelium similar to the hair follicle infundibulum, which is surrounded by fibrosis (Fig. 1B). Active inflammation is sometimes seen around the cyst. The etiology and pathogenesis of these pathological findings are controversial. It remains unclear whether calcified epidermal cysts are the result of dystrophic calcification of preceding epidermal cysts that are affected by inflammation followed by cystic dilation, calcification, cyst wall rupture, and granulomatous reactions,1or if they are truly idiopathic growths without any triggering factor such as foreign body infiltration, metabolic or hormonal disorder, or trauma.2Calcified epidermal cysts reportedly have an eccrine origin.3In some cases the cyst wall and keratinous material are absorbed, leaving only areas of calcification,4suggesting that the pathological finding of the attenuated epithelial lining may ultimately disappear.
Clinical features
Calcified epidermal cysts are rare benign entities thatwere first described in 1947.5 There are reports of calcified epidermal cysts involving the intracalvarium, spinal cord, spleen,pancreas, kidney, testis, and several skin regions.6–9Cutaneous calcified epidermal cysts have been reported on the scrotum, vulva, scalp, subungual area, breast, andheel, but are most commonly located on the scrotum.9The typical clinical presentation is a rock-hard white nodule with associated pruritus that sometimes drains white chalky contents accompanied by secondary skin infection. The entity can also be clinically similar to a common epidermal cyst (Fig. 2).The differential diagnoses for calcified epidermal cysts include: cutaneous tumors such as steatocystoma, lipoma,solitary neurofibroma, pilomatricoma, and cervical lymphangioma; inflammatory nodules, including cervical lymphadenitis and cervical lymph node tuberculosis;systemic diseases that cause cutaneous nodules, such as hyperparathyroidism, dermatomyositis, and systemic sclerosis. General diagnostic workup includes a detailed history, urinalysis, blood biochemical examination (calcium, phosphorus, and parathyroid hormone levels), and histopathologic study. The gold standard for the diagnosis of a calcified epidermal cyst is excisional biopsy and pathologic evaluation, which reveals an epidermal cyst with central irregular calcifications. Surgical management with complete excision achieves excellent results and reduces recurrence.

Figure 2. Clinical presentation of the lesion of calcified epidermal cyst on the neck. A 2cm × 1cm, hemispherical, skin-colored, firm nodule with mild tenderness and a smooth surface in the upper part of the left neck.
- 国际皮肤性病学杂志的其它文章
- Understanding of Melanocyte Distribution in Skin
- Epidural Block Treatment on Postherpetic Neuralgia and Comorbid Spine Metastasis of Malignant Tumor: Two Cases of Report
- Role of Tight Junctions and Their Protein Expression in Atopic Dermatitis
- Consensus on the Diagnosis and Treatment of Vitiligo in China (2021 Revision)#
- Guidelines for Diagnosis and Treatment of Atopic Dermatitis in China (2020)#
- Erosive Pustular Dermatosis of the Scalp After Excision and Skin Grafting of Scalp Squamous Cell Carcinoma