
Current state and exploration of fat grafting
2021-03-08 12:54:38ChenChengYunXieQingfengLi
Chen Cheng, Yun Xie, Qingfeng Li
Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
Keywords:Fat grafting Fat compartment Regenerative treatment
ABSTRACT Fat grafting has become one of the most frequently used techniques in plastic and reconstructive surgery.Many studies have focused on optimizing procedures,such as donor site selection,harvesting,processing,and grafting.Representative basic techniques include Coleman’s and “3L3M” techniques.A new technique called compartment-based targeted fat grafting (CTFG) has gradually been established based on anatomical findings of the facial and hand compartments.CTFG achieved precise restoration of the fat volume in the anatomical state.Cell-based fat grafting has introduced new fields involving tissue repair and regeneration, including facial rejuvenation and scar improvement,among others.In this review,we summarize the timeline for the development of fat grafting.
1.Introduction
Since Neuber performed the first fat grafting procedure in 1983,1the technique has improved rapidly with the development of liposuction in 1977.2As fat harvesting,processing,and grafting advances by leaps and bounds, basic techniques of fat grafting have been established by many researchers.Currently, fat grafting is one of the most frequently used techniques in plastic and reconstructive surgery.Based on anatomical findings of the facial and hand compartments, a new technique of compartment-based targeted fat grafting (CTFG) has gradually been established, and fat grafting has been renewed.This technique offers optimal and safe outcomes for both surgeons and patients.In the field of tissue repair and regeneration, cell-based fat grafting results in facial rejuvenation, scar improvement, and other effects.In this review, we summarize the timeline of fat grafting and several key time points in the development of the technique.
2.Basic techniques of fat grafting
The aim of fat grafting is to harvest the fat with minimal tissue damage and safely inject the processed fat with long-lasting results.3Therefore,many studies have focused on optimizing the procedure.
2.1.Donor site selection
Many studies have aimed to identify possible differences related to the harvesting site.4–7Some studies have suggested that the lower abdomen and the inner thigh may have higher processed adipose cell concentrations,5–7but there are other studies showing no difference in cell viability between donor sites.8–10Given the lack of a strong consensus supporting the use of a specific site,donor site selection should likely be driven mainly by patient and surgeon preference.11
2.2.Fat harvest
The diameter of the aspiration cannula is one of the most important factors for fat harvesting.Many studies have shown that cannulas with larger diameters have lower inlet pressure and maximum velocity during the liposuction process, which further influences the viability of adipocytes and adipose stem cells,and thus has larger fat graft retention.12–15
Energy-assisted liposuction devices, including ultrasound-assisted and tissue liquefaction liposuction, have also been studied for fat harvesting.A number of studies have investigated cell counts,viability,and fat retentionin vivobetween different liposuction devices, and no significant differences have been demonstrated.16,17
2.3.Fat processing and grafting
Several studies have compared centrifugation and decantation with or without washing.Most studies have shown that centrifugation affects the cellular components of aspirated fat and decreases viability.17–19However, the difference in viability is not highly related to graft retentionin vivo.17,20,21
With systematic research on fat grafting, including fat harvesting,processing, and grafting, the efficacy of volume enlargement by fat grafting has largely improved.The representative techniques included structural fat grafting22,23and the“3L3M” technique.24
Structural fat grafting was established by Coleman et al.This technique leads to “structural improvement” in patients with remarkable bone and soft tissue deficiency.22Coleman’s technique was classified into several steps to determine how fat grafts should be harvested,processed,and placed.25Based on previous experience,the parameters for each step were established.
Based on an objective experiment called the glucose transport test,26the parameters of each step were optimized.The procedure of fat grafting could be summarized as“3L3M”,27,28which is low-pressure liposuction,low-speed centrifugation, as well as low-volume, multi-point,multi-plane, and multi-tunnel injection.Fat tissues should be harvested through cannulas measuring 2–3 mm in diameter.The pressure of liposuction should be less than 20–40 kPa.The volume rates of lipoaspirates and tumescent solution were suggested to be set at a ratio of 1:1 to 1:3.Centrifugation at low speeds (<100 g) would largely decrease the possibility of damaging fat particles.Lipotransfer at low volumes using a multi-plane, multi-tunnel, and multi-point approach would maximally increase the survival rate of fat particles.Based on these well-established techniques,fat grafting can be performed more efficiently.
2.4.Complications
Aside from efficacy issues,there are also safety issues that come with fat grafting.Several complications may occur with facial fat grafting,including contour irregularities, prolonged bruising and swelling, infection, and granulomas.Severe complications may also occur, such as vascular embolization with visual loss or stroke.29For large-volume grafting, including breast and buttock augmentation, complications of cysts, calcifications,fat necrosis,and others have been reported.30
3.New concepts of fat grafting
3.1.Anatomic fat compartments
Castanares described the lateral fat compartment of the lower eyelid in 1983,31followed by several studies focusing on the infraorbital fat compartment.32,33Rohrich described the facial fat compartment through anatomical studies and suggested that the adipose tissue of the entire human body is highly compartmentalized.34For facial fat grafting, the recipient site has been well identified after the anatomical discovery of fat compartments.
Based on anatomical studies,several structures referred to as retaining ligaments are formed simply by fusion points of the abutting septal barriers of facial compartments.35Rohrich combined superficial musculoaponeurotic system lifting and selective fat compartment volume restoration to achieve facial rejuvenation.36,37The nasolabial fold and deep malar fat compartments were directly restored by the open incisions from the face lift procedure, which was described as the “lift-and-fill”technique.36
Fat compartments in the temporal, midface, and hand regions were systematically studied,and a large sample of clinical cases were operated on through minimally invasive grafting.38–41With the findings from these studies,the technique of CTFG has gradually been established and is expected to become an advanced surgical approach for better anatomical restoration of the face.42
3.2.Compartment-based targeted fat grafting
The concept of fat compartments suggests that facial fat is not a uniform and continuous structure.35,43The precise restoration of fat compartments is a primary consideration.Therefore,any fat graft outside a compartment would cause unnatural facial contour,such as a“balloon”face, or an unnatural appearance.
In addition to efficiency, safety issues are another unavoidable problem.It has been reported that embolism caused by fat grafting may cause vision loss and hemiplegia.44CTFG may prevent any unintended injury to the blood vessels or nerves in the recipient area by placing the injection site over the selected fat compartment.
Compared with previous fat grafting techniques, CTFG offers an optimal and safe outcome for soft tissue augmentation,because it allows for the precise restoration of fat volume in the anatomical state.38–41Fat compartments in the face or hand40have been anatomically studied more than the other two popular sites of the breast and buttocks.For breast augmentation, liponecrotic cysts and related breast cancer concerns are still considered difficult cases.24However,buttock augmentation with fat grafting has been associated with a significantly increased risk of pulmonary fat embolism.45Therefore,more studies should be conducted to understand the compartments of the breasts and buttocks to improve the safety of the technique.
3.3.From fillers to regenerative medicine
Fat grafting could improve volume defects.However,decreased skin pigmentation in fat recipient sites was also noticed in a clinical study,46which indicates the regenerative capacity of fat grafts.
Different methods of fat processing have been explored over time,and fat grafting has entered new fields involving tissue repair and regeneration.The fractions or cells of fat particles made by emulsification or by collagenase digestion, known as nanofat47or stromal vascular fractions(SVF),48were used for intradermal injection.The clinical applications of nanofat showed remarkable improvements in skin quality after six months.47Cells combined with fat grafts or cell-assisted lipotransfer(CAL) were also found to be more effective for augmentation and superior to conventional techniques.49
Moreover, through specific extraction and isolation procedures,adipose-derived stem cells (ADSCs) and cellular adipose matrix can be harvested from fat, which is also used in regenerative treatment.50,51Several studies have implied that SVF or ADSCs could shorten the tissue expansion process by enhancing skin regeneration.52,53SVF or ADSCs can also enhance angiogenesis after skin grafting and improve the texture and elasticity of skin grafts.54,55These cell-based therapies supplement current techniques and allow fat grafting to enter a new area.
The nanofat can be injected smoothly through needles up to 27 gauge.47Methods on how to obtain smaller fat particles while maintaining the regeneration capacity of the graft requires further study.Although the regenerative treatment of fat grafting varies in different studies,the clinical indications still need to be further explored through evidence-based studies.
For safety concerns,the exact effects of collagenase,culture media,or other non-autografts on human bodies remain unknown.The clinical investigators of cell-based therapy had to obtain approval from the ethics committee and perform clinical studies before performing extensive application.Moreover, standard procedures of SVF harvest or ADSC culture required establishment under the supervision of the Center for Drug Evaluation.
4.Prospect
Fat tissues are reproducible and easy to obtain under local anesthesia.Although their initial purpose was to be used as fillers, fat grafts have many beneficial effects in terms of tissue repair and regeneration.Currently, regenerative treatment of cell-based fat grafting includes the fields of facial rejuvenation,56,57scar improvement,58,59hair regrowth,60and wound healing,61among others.Fat grafts are tissue-inducing biomaterials.It was implied that fractionated human adipose tissue holds promise as a new class of bone substitutes that promote endochondral ossification,62,63which made it possible to induce fat in cartilage and bone tissues.Several key time points for fat grafting are summarized in Fig.1.
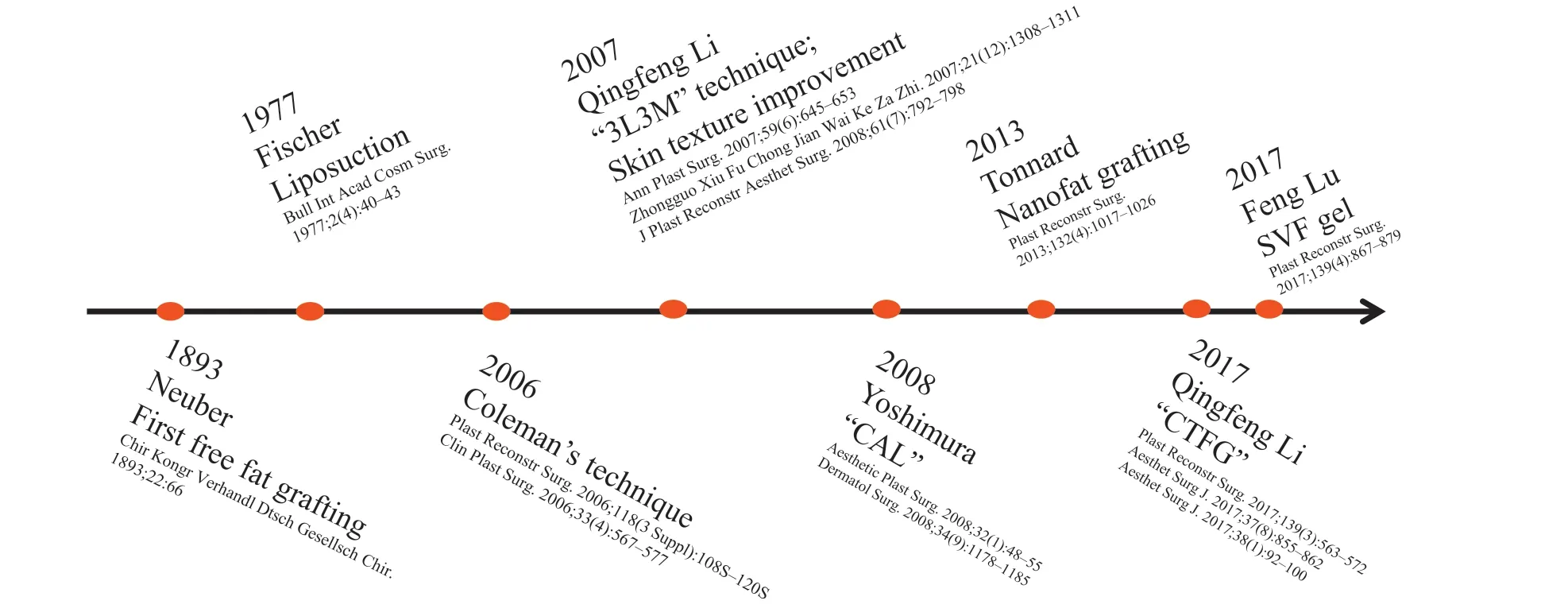
Fig.1. Key time points of fat grafting.The publication time of the representative literature was listed from the first free fat grafting to the recently used technique.3L3M,low-pressure liposuction,low-speed centrifugation, as well as low-volume,multi-point, multi-plane,and multi-tunnel injection; CAL,cell-assisted lipotransfer;CTFG, compartment-based targeted fat grafting; SVF, stromal vascular fraction.
5.Conclusion
In this review, we summarize the key time points for fat grafting.Recent fat grafting is an efficient and safe method for volume enlargement, as well as for regenerative applications through cell-based treatment.As an autologous tissue free of donor site damage, fat grafts have tremendous potential use in plastic and reconstructive surgery.
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interest
The authors declare that they have no competing interests.
Authors’contributions
Cheng C: Writing-Original draft.Xie Y and Li Q: Writing-Reviewing and Editing.
Acknowledgments
This work was supported by the Shanghai Municipal Key Clinical Specialty Project(grant no.shslczdzk00901).
 Chinese Journal of Plastic and Reconstructive Surgery2021年4期
Chinese Journal of Plastic and Reconstructive Surgery2021年4期
- Chinese Journal of Plastic and Reconstructive Surgery的其它文章
- Foreword from Professor Weiguo Hu
- Augmentation mammoplasty with autologous fat grafting
- Progress of laser and light treatments for lower eyelid rejuvenation
- Application of digital technology in nasal reconstruction
- Micro-compound tissue grafting for repairing linear scars
- Nursing care of vascular crisis in a child with neck skin contracture and skin flap transplantation after burn: A case report