
Open reduction and Herbert screw fixation of Pipkin type IV femoral head fracture in an adolescent:A case report
2021-02-22 07:21:46
World Journal of Clinical Cases 2021年4期
Yao Liu,Jin Dai,Xiao-Dong Wang,Zhi-Xiong Guo,Lun-Qing Zhu,Yun-Fang Zhen,Department of Orthopaedics,Children’s Hospital of Soochow University,Suzhou 215000,Jiangsu Province,China
Abstract BACKGROUND Femoral head fracture is extremely rare in children.This may be the youngest patient with femoral head fracture ever reported in the literature.There are few pediatric studies that focus on cases treated with open reduction via the modified Hardinge approach.CASE SUMMARY A 14-year-old female adolescent suffered a serious traffic accident when she was sitting on the back seat of a motorcycle.A pelvic radiograph and computed tomography revealed a proximal femoral fracture and slight acetabular rim fracture.This was diagnosed as a Pipkin type IV femoral head fracture.An open reduction and Herbert screw fixation was performed via a modified Hardinge approach.After 1-year follow-up,the patient could walk without aid and participate in physical activities.The X-ray results showed that the fractures healed well with no evidence of complications.CONCLUSION Open reduction and Herbert screw fixation is an available therapy to treat Pipkin type IV femoral head fractures in children.
Key Words:Pipkin classification;Femoral head fracture;Adolescent;Fracture fixation;Case report
INTRODUCTION
Femoral head fractures are uncommon injuries in adults and more rarely seen in children and adolescents.With high energy injuries increasing,especially in car accidents,hip traumas are becoming more frequent.The literature shows that about 5%-15% of hip dislocations are accompanied by proximal femoral fractures[1].The most commonly used classification,described by Pipkin,is to use the fracture line location and lesion in the femoral neck or acetabulum to define the type of fracture[2].Patients with a Pipkin type I or II injury have more optimal outcomes than those with a Pipkin type III or IV injury[3].To our knowledge,few articles have reported femoral head fractures in skeletally immature patients.We operated on a 14-year-old female diagnosed with a Pipkin type IV fracture.After one year,excellent clinical function and radiographic fracture healing were observed.
CASE PRESENTATION
Chief complaints
A 14-year-old Chinese female was transferred to our hospital with the chief complaints of severe hip pain and difficult thigh movement after being struck by a car when she was riding pillion on a motor bike 4 d before.
History of present illness
Due to left hip pain and limited movement,radiographic examinations were performed in the emergency room of the local hospital.The patient was diagnosed with “hip dislocation and femoral head fracture.” After 4 d of inpatient observation and skeletal traction the patient was transported to our department.
History of past illness
The patient had a free previous medical history.
Physical examination
The patient exhibited hip tenderness and limitation of motion.No neurovascular injury was observed.
Imaging examinations
A three-dimensional computed tomography (CT) scan demonstrated a femoral head fracture.Axial and sagittal CT scans showed the posterior acetabulum with slight displacement.A coronal CT scan showed the fracture line extending superior to the fovea centralis (Figure 1).
FINAL DIAGNOSIS
The final diagnosis was a femoral head fracture associated with posterior acetabular fracture categorized as a Pipkin type IV fracture.
TREATMENT
Preoperative skeletal traction
The patient underwent skeletal traction for 7 d including 4 d in the local department and 3 d in our hospital.
Surgical procedures
After a general physical check-up and confirmation that vital signs were stable,we opted for surgical intervention on the 7thd after injury.We chose a modified Hardinge approach to expose the operative field with the patient in a side-lying position after general anesthesia.A longitudinal skin incision was made in the middle of the greater trochanter.The inferior fat and fascia were incised and retracted.After blunt dissection and retraction of the anterior third of the gluteus medius,electrosurgical dissection was used to split the tendinous portion of the distal gluteus medius and the anterior part of the vastus lateralis muscles.The capsule was exposed,and a “T”-shaped incision was made.The femoral head was dislocated anteriorly with flexion,extension and adduction.A piece of the large fragment and some smaller articular debris were detected in the nonweight-bearing area (Figure 2).The large fragment comprised 20%of the articular surface and was notably rotated.The ligamentum teres was ruptured from its insertion into the acetabulum.After resection of the torn ligament and articular purge,the major fragment was manipulated carefully back into place and an anatomical reduction of the articular surface was obtained.Three Herbert screws were used to fix the fragment with specific attention to avoiding screw protrusion.Then the hip joint was reduced by gentle abduction and internal rotation.We tested the range of motion and joint stability.The reduced hip demonstrated no limitation of passive activity.The wound was closed,and a drain was inserted.Intraoperative x-rays demonstrated an ideal reduction of the femoral head.
OUTCOME AND FOLLOW-UP
The patient was compliant with physical exercises and partial weight-bearing with crutches after surgery.The postoperative hospitalization time was 2 wk.Follow-up occurred 4,8 and 12 wk postoperatively.At 6 mo after discharged from hospital she returned to school and could walk without crutches.One year after the surgery the patient had no left hip pain and was playing partial-contact sports without difficulty.Her left hip range of motion demonstrated hip flexion range of 0° to 100°,internal rotation to 20°,external rotation to 40°,abduction to 30° and adduction to 30°.Radiographs 12 mo after the injury demonstrated fracture healing with no evidence of osteonecrosis (Figure 3A and 3B).
DISCUSSION
Pipkin fractures are rare injuries,especially in the pediatric population.There are few papers in the literature that describe femoral head fractures in skeletally immature patients.The previous literature has reported an incidence of two in a million per year[4].With the growing incidence of traffic accidents,the occurrence of hip fracturedislocation has increased[5].The mechanism of this injury is very complicated due to the indirect force intensity to the hip caused by impact transmitted along the femoral shaft[6].Compared with adults,associated fractures are more uncommon in children with traumatic hip dislocation[7].Cartilaginous pliability and ligamentous laxity in children provide increased elasticity,which could explain the rarity of this type of fracture in children.
The Pipkin system is the typical classification for femoral head fracture dislocations[2,8].Type IV lesions,which are characterized by lesions of both the femoral head and acetabular rim,usually have a poor prognosis[9].Treatment options for Pipkin type IV fractures include fragment excision,internal fixation and arthroplasty[10-12].The primary goals of open reduction are to remove loose fragments,to restore stability to the hip joint and to ensure concentric hip reduction.
The optimal timing of surgery is still controversial.Some literature indicated worse outcomes for Pipkin fractures with delayed surgery compared with those who had immediate surgery[13].However,other studies showed no statistically significant differences in outcome when comparing time of surgery with hip reduction,definitive operative intervention or the anatomic operative approach to injury[3].
Skeletal traction is a temporary measure in acetabular and proximal femoral fractures when surgical intervention is delayed[14].In our case,bony traction was performed immediately in the local hospital so that a prompt concentrated hip reduction and temporary immobilization were achieved.This may be one reason for the absence of complications.
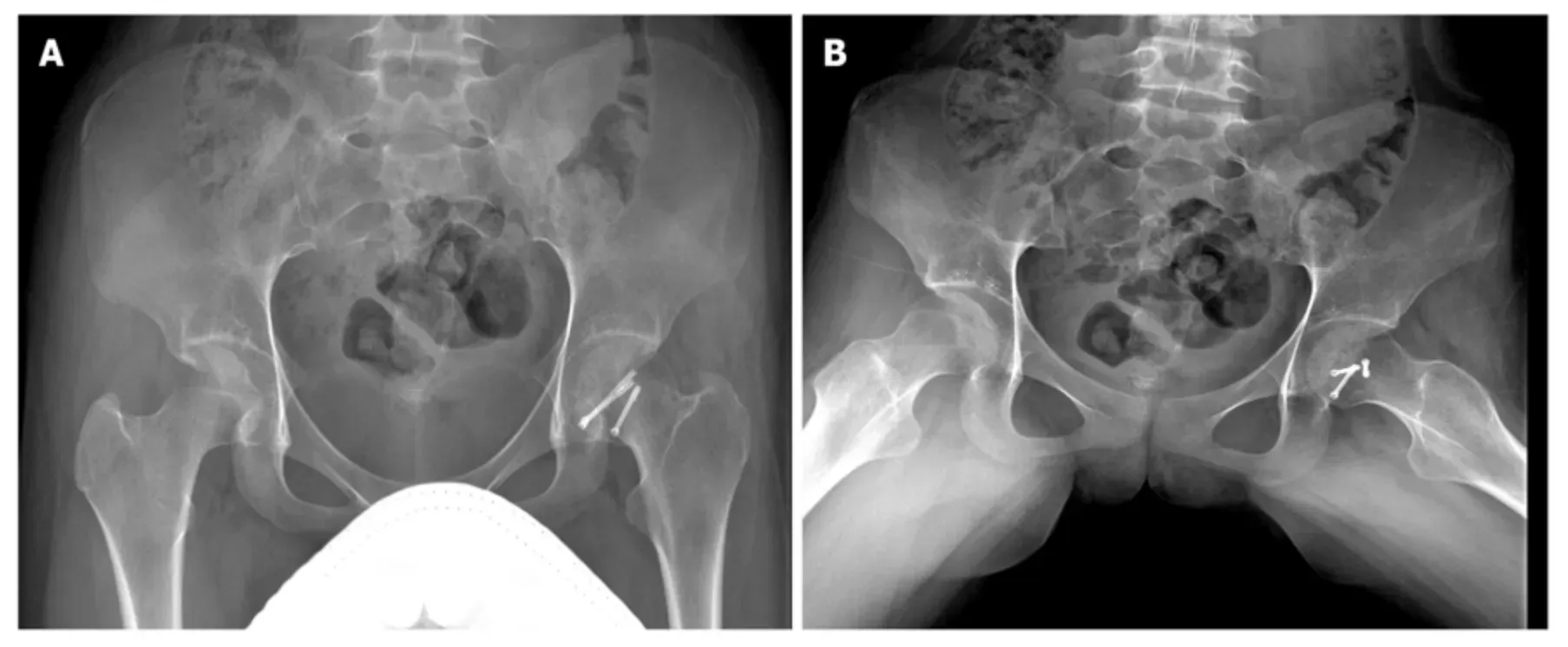
Figure 3 Pelvic radiographs 1 year after operation.
In theory,treatment through surgical hip dislocation or a posterior approach to fix both the acetabulum and femoral head is advocated in dealing with Pipkin type IV fractures[15,16].However,we chose a modified Hardinge approach for the following reasons.First,the patient was skeletally immature with an obvious greater trochanteric epiphyseal line on the CT scan.A digastric trochanteric flip osteotomy might cause growth disorders of the proximal femur.Second,the larger fragment was located on the inferior and anterior portion of the femoral head,which would be difficult to fix through a posterior approach.Third,there were slight fractures with no displacement in the posterior acetabular rim that had no need for reconstruction.Additionally,the modified Hardinge approach was the most familiar approach for us and is widely used in the treatment of pediatric hip septic arthritis and femoral neck fracture[17].This modified approach compromised little of the abductor function;most of the gluteus medius retained function[18].Also,the literature showed there was no significant statistical difference in the therapeutic effect among anterior,posterior or trochanteric-flip approaches for repair of femoral head fractures[5].
There is still disagreement over whether fragments should be fixed or removed[19].Most surgeons agree that large fracture fragments and those located in the loadbearing area should be retained and anatomically repositioned[20].The diameter of the large fragment in this case was about two centimeters;we chose to operate using Herbert screw fixation.Other small debris and the severed ligamentum teres were removed to facilitate the reduction of hip joint.Radiographs of the pelvis were obtained after manipulation to check concentric reduction.The most common complications are nonunion,femoral head avascular necrosis,heterotopic ossification,osteoarthritis and stiffness[5].None of these sequelae were seen after early exercise and partial weight-bearing.It is particularly important to point out that the follow-up time is relatively short.Long term clinical follow-up is needed to fully evaluate the prognosis.
CONCLUSION
This case report describes a rare case of Pipkin type IV fracture in a 14-year-old female.With open reduction and Herbert screw fixationviaa modified Hardinge approach,satisfactory patient outcomes were observed without major complications.
 World Journal of Clinical Cases2021年4期
World Journal of Clinical Cases2021年4期
- World Journal of Clinical Cases的其它文章
- Isolated interrupted aortic arch in an adult:A case report
- Fertility-sparing surgeries without adjuvant therapy through term pregnancies in a patient with low-grade endometrial stromal sarcoma:A case report
- Primary nonkeratinizing squamous cell carcinoma of the scapular bone:A case report
- Acute inferior wall myocardial infarction induced by aortic dissection in a young adult with Marfan syndrome:A case report
- Immediate implant placement in combination with platelet rich-fibrin into extraction sites with periapical infection in the esthetic zone:A case report and review of literature
- Pheochromocytoma as a cause of repeated acute myocardial infarctions,heart failure,and transient erythrocytosis:A case report and review of the literature