
Effect of hospital discharge plan for children with type 1 diabetes on discharge readiness,discharge education quality,and blood glucose control
2021-02-22 07:21
World Journal of Clinical Cases 2021年4期
Hui-Juan Tong,Ling Fan,Department of Nursing,Shengjing Hospital of China Medical University,Shenyang 110004,Liaoning Province,China
Feng Qiu,Department of Ophthalmology,Shenyang Fourth People’s Hospital,Shenyang 110034,Liaoning Province,China
Abstract BACKGROUND Type 1 diabetes is one of the most common chronic diseases in childhood.The number of type 1 diabetes patients in China still ranks fourth in the world.Therefore,children with type 1 diabetes in China are a group that needs attention.The management of type 1 diabetes mellitus (T1DM) involves many aspects of daily life.It is extremely challenging for children and their families.T1DM children have complex medical care needs.Despite the continuous development of therapeutic medicine and treatment technologies,blood glucose control in children with T1DM is still not ideal.They and their parents need to acquire more knowledge and skills before being discharged.AIM To explore the influence of hospital discharge plan based on parental care needs of children with T1DM on discharge readiness,quality of discharge education and blood glucose control level.METHODS In total,102 parents of children with type 1 diabetes were divided into control group and intervention group according to admission time.Fifty cases from February to June 2019 were selected as the control group,and 52 cases from July to October 2019 were selected as the intervention group to implement the discharge plan.The Readiness for Hospital Discharge Scale,Hospital Discharged Education Quality Scale and children's blood glucose metabolism indicators were used to compare the differences in discharge preparation,discharge education quality and blood glucose control between the two groups of children and their parents.RESULTS On the day of discharge,the two groups of children had the following scores of readiness for discharge:The intervention group score was 225.34 ± 32.47,and the control group score was 208.68 ± 29.31.The P value was 0.007,and the difference was statistically significant.The discharge education quality scores were as follows:The intervention group score was 135.11 ± 19.86,the control group score was 124.13 ± 15.56,the P value was 0.002 and the difference was statistically significant.Three months after discharge,the blood glucose metabolism indicator showed that the glycosylated hemoglobin value of the two groups was (7.45% ±1.04%),and that of the control group was (8.04% ± 1.27%),P = 0.012.Therefore,the improvement of parents' readiness for discharge,quality of discharge education and blood glucose metabolism indicators (glycosylated hemoglobin,fasting blood glucose and postprandial blood glucose) in the intervention group were better than those in the control group (P <0.05),and the difference was statistically significant.CONCLUSION The discharge plan for children with T1DM can help the children and their families realize the transition from hospital care to home self-management and improve the parents' readiness for discharge,thereby improving children’s blood glucose control levels.
Key Words:Type 1 diabetes;Hospital discharge plan;Hospital discharge readiness;Blood glucose control;Children;Parents
INTRODUCTION
Type 1 diabetes mellitus (T1DM) is a major pediatric endocrine disease that endangers children’s health.The incidence of T1DM in children is increasing rapidly and is obviously trending towards a younger age[1].The number of T1DM cases in children and adolescents worldwide has reached 110 million,and 132600 new patients are added each year[2].In recent years,the incidence rate in China has been 2/100000 to 5/100000,and the average annual growth rate of children younger than 5 years of age is 5%-34%[3,4].The incidence of T1DM in children is increased 3.8 times than that of 20 years ago,and the number of diseases is fourth in the world,which brings huge social and economic burden[5].Despite the continuous development of therapeutic medicine and treatment technologies,blood glucose control in children with T1DM is still unsatisfied.The single-center glycosylated hemoglobin (HbA1c) compliance rate is only 15%,which is far lower than the 44%-59% compliance rate in the United States,Germany and other European countries[6].The multicenter "3C" study shows that the incidence of acute and chronic complications such as poor blood glucose control,ketoacidosis,blindness and uremia is high,and the average life span is significantly shortened[7,8].Lifelong insulin injection is the only effective treatment for patients with T1DM.Therefore,the daily management of children with T1DM is a complex and demanding task,requiring blood glucose monitoring at least four times a day,insulin injections at least four times a day,insulin pump infusion catheter replacement every 2-3 d,carbohydrate intake calculation and food intake monitoring,insulin dose calculation,physical activity control and hypoglycemia and hyperglycemia prevention and treatment[9,10].Self-management of children with T1DM refers to the process in which the children and their families jointly assume the responsibility of managing the disease,adopt behaviors that are conducive to disease recovery and make health decisions to control the disease or maintain the current state[11,12].
Because children with T1DM are only hospitalized for treatment and nursing at the early stage of diagnosis when blood glucose is adjusted or acute metabolic disorder or poor blood glucose control occurs,hospitalization time is generally within 1 wk[13].More than 95% of the time,the children stay at home or go to school.When discharged from the hospital,only the condition has been effectively controlled,blood glucose regulation is stable and family self-management is still required after discharge.Usually,the doctor recommends that the child be evaluated every quarter,but it is only a short communication with the doctor;for the remaining more than 8000 h in a year,the child and his or her parents must carry out diabetes self-management[14].Therefore,the transition from hospital care to family self-care is a critical period for children and their families to adapt to the child’s illness and prepare for long-term self-management.T1DM children have complex medical care needs.They and their parents need to acquire more knowledge and skills before being discharged from the hospital to cope with changes in the children's physical conditions and the impact of the disease on the entire family.The focus of preparation for discharge is to educate children and their families for the transition from hospitalization to family home care.
The hospital discharge plan[15,16],as a main mode of continuous nursing,is a nursing process to promote the smooth transfer of patients from one environment to another,which starts on the day of admission and is automatically continuous after discharge.Studies[17]have shown that discharge plan can improve caregivers’ readiness for discharge and meet their care needs,thereby improving patient health outcomes and increasing patient satisfaction.At present,more and more researchers pay attention to the discharge plan of patients with chronic diseases.However,because the application of discharge plan in China is still in its infancy,there is no standardized discharge plan implementation guide or program.Therefore,combining with the needs and experiences of home care of caregivers of children with T1DM,it is of great significance to construct the intervention contents and intervention strategies of discharge plan to improve the readiness of parents of children with T1DM.
Under the background of specific family,education and medical care in China,based on the needs of caregivers,expert meetings and literature analysis,this study constructed the implementation plan of discharge plan for children with T1DM.Through the implementation of discharge plan for children with T1DM,the impact of the program on the readiness of children and their parents,the quality of discharge education and the health outcomes of children was discussed.
MATERIALS AND METHODS
Research design
This study is a quasi experimental study;using a prospective clinical trial design,the subjects were divided into intervention group and control group according to the order of admission time.
Research object
Children with T1DM who were hospitalized in Shengjing Hospital of China Medical University from February 2019 to October 2019 and their parental caregivers were selected as the research subjects.The parents of 50 children who were hospitalized from February to June 2019 were selected as the control group,and the parents of 52 children from July to October 2019 were selected as the intervention group for hospital discharge plan intervention.The inclusion and exclusion criteria for the research subjects were as follows:(1) Inclusion criteria:Children who met the diagnostic criteria for T1DM[18],14 years of age or younger and parents were primary caregivers;and (2)Exclusion criteria:The child with T1DM also experienced other significant comorbidities or chronic diseases,the child with T1DM was receiving intervention from other health care teams,and T1DM parental caregiver was unable to communication fluently in the local language of the investigator (Mandarin Chinese).
Interventions in the experimental group
Construct the hospital discharge plan for children with T1DM:The construction of the hospital discharge plan included the following steps:(1) Based on the qualitative research results,the content module of the hospital discharge plan for children with T1DM was constructed,including information demands,skill demands,emotional demands and social needs;(2) The results of the demand survey of T1DM after discharge provided a reference for the formulation of the intervention time and dose in the discharge plan;and (3) Based on the four content modules of the discharge plan,combined with a literature analysis,a preliminary discharge plan was formed and revised through expert meetings.After the meeting,the intervention plan was analyzed,modified,supplemented and improved,and finally the implementation plan of T1DM discharge plan was formed.
Form a multidisciplinary team:A medical integration team for the discharge plan for children with T1DM was constructed.The multidisciplinary team participated in the discharge plan and included one attending endocrinologist,one nutritionist,one pharmacist,one psychologist,one continuing care nurse,one ward nurse and the researchers.
Implement the intervention plan:The research plan adopted thematic education,skill training and psychological intervention in the hospital.After discharge,we took telephone follow-up and Wechat intervention.Thematic education for children with T1DM and their families focused on problem-solving and coping abilities and required their active participation to cultivate their self-management skills and decision-making capabilities.Therefore,health education and skill training adopted the teaching-back method.According to the different education contents,the topic education adopted the talk-back and demo-back.
According to the qualitative research on the theme of care demands and the results of continuing nursing demands after discharge,three times of thematic education were set up,about 30 min each time,one skill training,one operation demonstration,one psychological intervention and the specific forms and time cut-off points of intervention are shown in Table 1.
Interventions in the control group
The interventions of the control group were carried out in accordance with the hospital's regular discharge guidance,including routine health education during hospitalization.The discharge guidance,which involved medication,diet,activities,condition monitoring and follow-up visits,was conducted by the responsible nurse 1 d before discharge.Within 1 wk after discharge from the hospital,the responsible nurse conducted a telephone follow-up,which involved assessment of the medical condition and satisfaction during hospitalization.
Evaluation indicators
Our research took individual and family self-management theory as the theoretical framework[19]and used process indicators and outcome indicators to evaluate the effect of intervention.Discharge readiness,education quality and blood glucose metabolism were used as evaluation indicators.Among them,the quality of discharge education and readiness of the children's parents were measured on the discharge day;the blood glucose metabolism indicators of the children were collected during admission and 3 mo after discharge.
Readiness for hospital discharge scale
The parent form of the Readiness for Hospital Discharge Scale (RHDS) was developed by Weisset al[20]to measure the preparation of children’s parents for discharge[20].There are a total of 29 items,21 of which are general items and 8 of which are parent-only additional items.The RHDS has the following four dimensions:Personal Status,knowledge,coping ability,and expected support.Each item is rated on a 10-point scale.The higher the score is,the better the preparation for discharge.Cronbach's alpha coefficient of the scale is 0.85,and the reliability of the dimensions of personal status,knowledge,coping ability and expected support are 0.71,0.85,0.86 and 0.84,respectively.Chenet al[21]translated this scale into Chinese in 2017 and found thatCronbach's alpha coefficient of the overall scale is 0.91,and Cronbach's alpha coefficient of each dimension is 0.78-0.92.
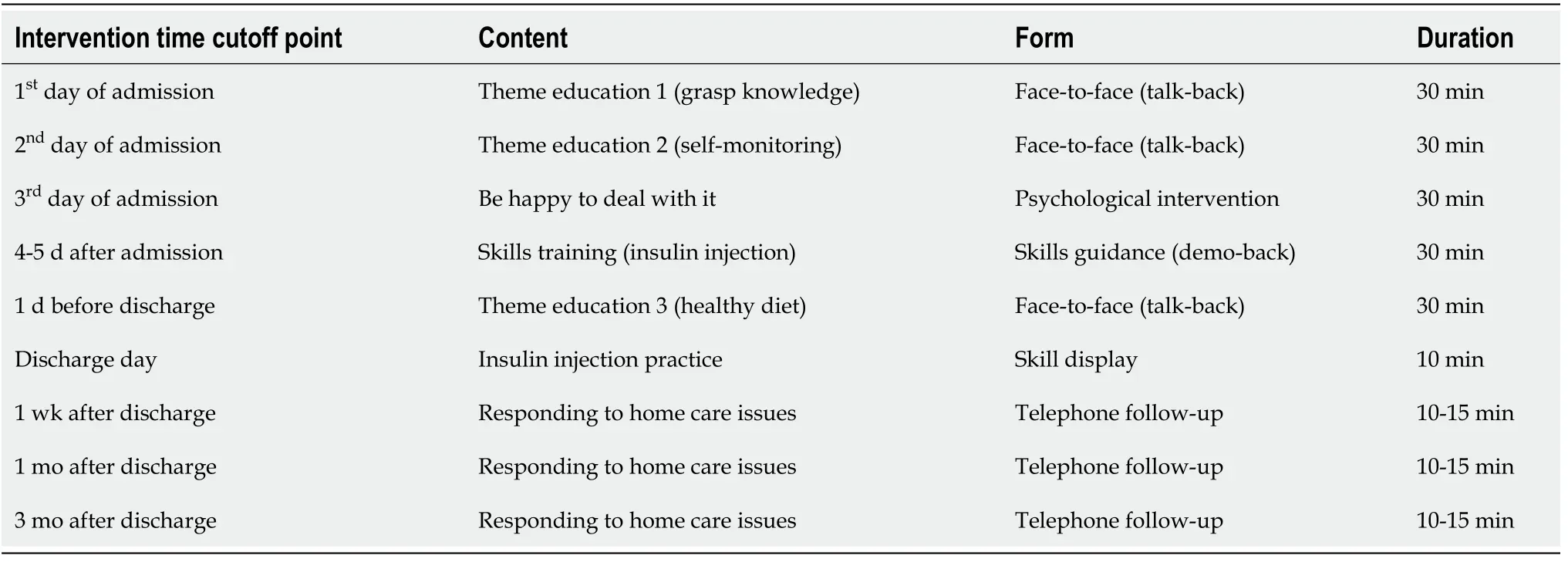
Table 1 Time cut-off point and content of intervention
Hospital discharge education quality scale
The Hospital Discharge Education Quality Scale was developed by Weisset al[20],and it includes two dimensions of discharge education content and education teaching skills,with a total of 18 items.The items of the education content dimension are six pairs of parallel items,which respectively reflect the two parallel items of the required content and the received content;each item uses a 0-10 scoring method.The higher the total score of the scale,the better the quality of patients’ discharge guidance.Cronbach's alpha coefficients of the total scale,discharge education content dimension and teaching skill dimension are 0.92,0.85 and 0.93,respectively.
Blood glucose metabolism indicators
HbA1c and blood glucose monitoring was used as the blood glucose metabolism indicators.HbA1c reflects the average blood glucose concentration for 2 to 3 wk previously and is used for short-term blood glucose control level evaluation[22].
Data analysis
SPSS (IBM 20.0,Armonk,NY,United States) software was used for statistical analysis.For normally distributed measurement data,the results were reported as the mean and standard deviation,and the two independent samplest-test was used for comparison.Count data were described by rates and percentages.The X2test or rank-sum test was used for comparison.All statistical tests in this study used a two-sided test,andP<0.05 indicated that the difference was statistically significant.
RESULTS
Baseline data
A total of 102 children were included in this study,including 52 children in the intervention group and 50 children in the control group.There was no significant difference between the two groups in gender,age,length of hospital stay,duration of illness and parental education level (P>0.05) (Table 2).
Comparison of discharge readiness scores between intervention group and control group in T1DM patients
On the day of discharge,the scores of discharge readiness of the two groups were 225.34 ± 32.47 in the intervention group and 208.68 ± 29.31 in the control group (P=0.007,P<0.05).The scores of discharge readiness in the intervention group were higher than those in the control group;the difference was statistically significant(Table 3).

Table 2 Comparison of baseline data between the two groups of children and parents

Table 3 Comparison of hospital discharge readiness between the two groups of children and parents
Comparison of discharge education quality between intervention group and control group in T1DM children
The scores of discharge education quality of the two groups were 135.11 ± 19.86 in the intervention group and 124.13 ± 15.56 in the control group (P= 0.002,P<0.05);the difference was statistically significant.The scores of discharge education quality of parents in the intervention group were higher than those in the control group(Table 4).
Comparison of blood glucose metabolism indicators between intervention group and control group
Before the intervention,there was no significant difference in blood glucose metabolism indicators between the two groups,including HbA1c (%),fasting blood glucose (mmoL/L) and 2-h postprandial blood glucose (mmoL/L) (P>0.05),but there was a significant difference in blood glucose metabolism indicators 3 mo after intervention (P<0.05),as shown in Table 5.

Table 4 Comparison of hospital discharge education quality between the two groups of children and parents
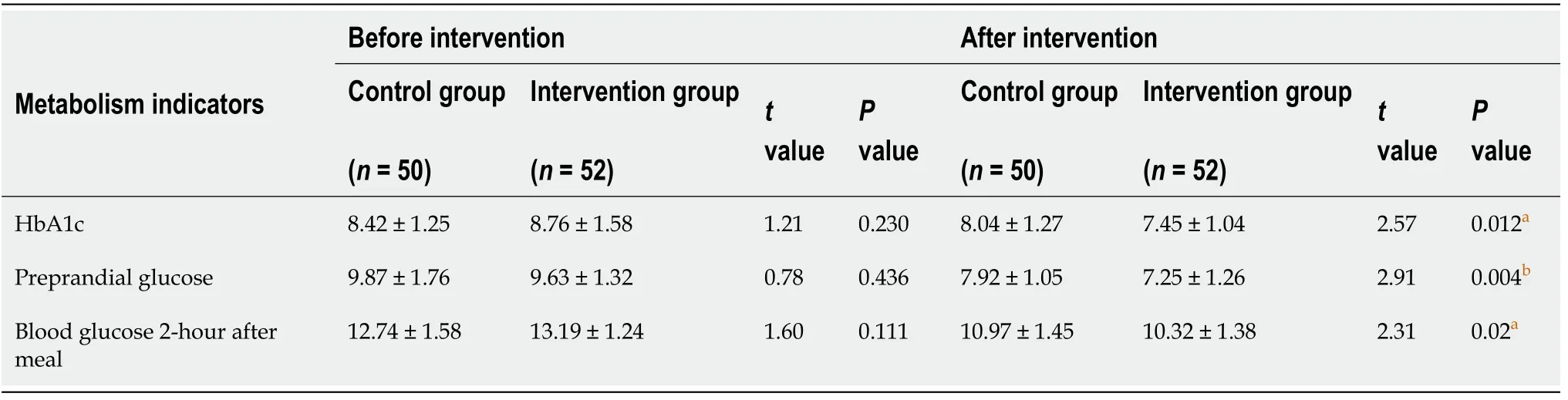
Table 5 Comparison of blood glucose metabolism indicators between the two groups of children
DISCUSSION
Hospital discharge intervention plan can improve the discharge readiness of parents of children with T1DM
Medical resources in China are not balanced,and the community health system is not well developed.Patients flock to tertiary hospitals in large cities for medical resources.Therefore,discharge education and guidance are mainly carried out in hospitals.Discharge readiness is an important predictor of whether a patient can effectively recover after discharge from the hospital[17].Through the evaluation of patients'readiness for discharge and targeted intervention measures,the discharge readiness and the ability of home care management after discharge can be improved.Parents’readiness for discharge is significantly related to the health of children with chronic diseases,parents’ satisfaction and the family’s physical,emotional,psychological and social health.Improving parents' readiness for discharge can reduce the risk of children's readmission and the incidence of complications[23].The discharge plan is an effective factor that affects parents’ discharge readiness.
Hospital discharge intervention plan can improve the quality of discharge education for children with T1DM
The focus of discharge preparation is to prepare children and their families for the transition from hospitalization to family and home care.Although preparation for hospital discharge is a multidisciplinary task,nurses have the primary responsibility for discharge education.Education intervention should be carried out for children and their families so that parents or caregivers can have the knowledge and skills needed to undertake the care responsibility and be prepared for the task of self-care at home during the transition from the hospital to the family.It is clearly pointed out in the diagnosis and treatment guidelines that a team composed of multiple professionals should be established to provide diabetes self-management education to patients and their families[24].Hospital discharge education aims to provide patients and their families with important medical care information so that they can master self-care methods and related precautions after discharge.Studies[25,26]have shown that highquality discharge education is beneficial to increase the cure rate,prevent complications,ensure that patients can be taken care of at home after discharge and continue to recover and reduce the rate of readmission.Therefore,nurses should master the skills of knowledge transfer related to discharge,thereby increasing the patient’s perception of readiness for discharge.Combined with the physical and mental development characteristics of children with T1DM and the need for disease management,parents not only need disease-related care knowledge but also need to master the corresponding operating skills.Therefore,it is recommended to use a combination of oral lectures and skill training to improve the quality of patient discharge education.
Hospital discharge intervention plan can improve blood glucose control in children with T1DM
Poor blood glucose control is an important factor leading to long-term complications such as diabetic nephropathy,diabetic eye disease,diabetic neuropathy,macrovascular complications and acute complications such as hypoglycemia and ketoacidosis[27],which seriously threaten children’s physical and mental health.Therefore,the main purpose of children's T1DM disease management is to achieve the best possible blood glucose concentration,minimize the occurrence of hypoglycemic events and prevent the occurrence of long-term complications.Our research results showed that the improvement in blood glucose metabolism indicators in children with T1DM in the intervention group was better than that in the control group,which further proved the effectiveness of the implementation of hospital discharge plans based on the care needs of parents of T1DM children.
CONCLUSION
The hospital discharge plan for children with T1DM was constructed based on the needs of children's caregivers,and it can improve the discharge preparation,the quality of discharge education and the outcome of blood glucose control for children with T1DM.Therefore,nurses can implement the T1DM discharge plan in a targeted manner to help children and their families realize an effective transition from hospital care to home self-management and improve the personal and family self-management capabilities of the children and their parents,thereby improving the health outcomes of the children.
ARTICLE HIGHLIGHTS
Research background
Type 1 diabetes is one of the most common chronic diseases in childhood.The number of type 1 diabetes patients in China still ranks fourth in the world.Therefore,children with type 1 diabetes in China are a group that needs attention.The management of type 1 diabetes mellitus (T1DM) involves many aspects of daily life.It is extremely challenging for children and their families.T1DM children have complex medical care needs.Despite the continuous development of therapeutic medicine and treatment technologies,blood glucose control in children with T1DM is still not ideal.They and their parents need to acquire more knowledge and skills before being discharged.
Research motivation
The discharge plan can improve caregivers’ readiness for discharge and meet their care needs,thereby improving patient health outcomes and increasing patient satisfaction.combining the needs and experience of home care by caregivers of children with T1DM,constructing a discharge plan for the purpose of improving the discharge preparation of parents of T1DM children has important clinical significance.
Research objectives
This research aimed to explore the impact of hospital discharge plan based on the needs of parents of children with T1DM on discharge readiness,discharge education quality and blood glucose control.
Research methods
A quasi experimental research study was performed.It adopted a prospective clinical experimental design and divided the research subjects into an intervention group and a control group in the order of admission time.The interventions of the control group were carried out in accordance with the hospital's regular discharge guidance;the intervention group was given hospital discharge plan intervention,including thematic education,skill training and psychological intervention in the hospital and adopted telephone follow-up and WeChat intervention after discharge.
Research results
The improvement in parents' discharge readiness,discharge education quality and blood glucose metabolism indicators (glycated hemoglobin,fasting blood glucose and postprandial blood glucose) of children in the intervention group were better than those in the control group,and the difference was statistically significant.
Research conclusions
The hospital discharge plan for children with type 1 diabetes can help children and their families realize the transition from hospital care to self-management at home and improve the preparation of children’s parents for discharge,thereby improving children’s blood glucose control levels.
Research perspectives
Our research results showed that the hospital discharge plan for children with type 1 diabetes could effectively improve the preparation of children’s parents for discharge and children’s blood glucose control levels.If the long-term intervention effect is to be observed,the follow-up time should be extended.
 World Journal of Clinical Cases2021年4期
World Journal of Clinical Cases2021年4期
- World Journal of Clinical Cases的其它文章
- Chiari malformations in children:An overview
- Effect of biofeedback combined with high-quality nursing in treatment of functional constipation
- Radioactive 125I seed implantation for pancreatic cancer with unexpected liver metastasis:A preliminary experience with 26 patients
- Biliary stent combined with iodine-125 seed strand implantation in malignant obstructive jaundice
- Usefulness of prenatal magnetic resonance imaging in differential diagnosis of fetal congenital cystic adenomatoid malformation and bronchopulmonary sequestration
- Reciprocal hematogenous osteomyelitis of the femurs caused by Anaerococcus prevotii:A case report