
Assessment of burden and coping strategies among caregivers of cancer patients in sub-Saharan Africa
2021-01-14 01:37PaulinaAckleyAkpanIdiokIjeomaOnyekachiEhiemereEkaeteFrancisAsuquoJoyAwuUkeunimChaboEasterChukwudiOsuchukwu
World Journal of Clinical Oncology 2020年12期
Paulina Ackley Akpan-Idiok, Ijeoma Onyekachi Ehiemere, Ekaete Francis Asuquo, Joy Awu Ukeunim Chabo,Easter Chukwudi Osuchukwu
Paulina Ackley Akpan-Idiok, Department of Nursing Science, Faculty of Allied Medical Sciences, College of Medicine, University of Calabar, Calabar 540222, Cross River State,Nigeria
Ijeoma Onyekachi Ehiemere, Department of Nursing Sciences, University of Nigeria, Nsukka 410001, Enugu, Nigeria
Ekaete Francis Asuquo, Easter Chukwudi Osuchukwu, Department of Nursing Sciences,University of Calabar, Calabar 54022, Cross River State, Nigeria
Joy Awu Ukeunim Chabo, Department of Public Health, University of Calabar, Calabar 54022,Cross River State, Nigeria
Abstract BACKGROUND Cancer is a devastating and debilitating chronic disease that affects both patients and family members. Available evidence has confirmed that the care of chronically ill relatives by family members can be very challenging. This is because caregiving of cancer patients often presents a high level of burden on the caregivers. Consequently, this leads to a necessity to adopt coping mechanisms to cushion the effect of the burden experienced during caregiving.AIM To determine the burden experienced and coping strategies among caregivers of advanced cancer patients attending University of Calabar Teaching Hospital(UCTH), Cross River State, Nigeria.METHODS The study adopted a descriptive cross-sectional study design and the study population included informal family caregivers providing services to histologically diagnosed advanced cancer patients receiving treatment at the UCTH at the time of this survey. A researcher-developed structured questionnaire, a 22-item standardized validated Zarit Burden Interview (ZBI) and a modified 17-item Coping Orientation to Problems Experienced (COPE)Inventory were used to collect data from 250 eligible informal caregivers who were selected with regard to caregiver’s characteristics, caregivers’ level of burden and caregiver’s coping strategies, respectively. Data gathered from the respondents were collated, coded and analyzed using Statistical Package for Social Sciences (SPSS version 24.0) software and Predictive Analytical Software(PAS version 19.0). Chi-square was used to test for association between categorical variables at the 0.05 level of significance. The results are presented in tables and charts.RESULTS The respondents consisted of more females 132 (62.86%) than males 78 (37.14%). The majority of respondents (46.2%) were aged between 31-50 years with a mean age of 35.9 ± 18.1 years. The assessment of burden level revealed that 97 caregivers (46.19%) experienced severe burden, 37 (17.62%) experienced trivial or no burden, while 76 (36.2%) perceived moderate burden. The coping strategies used by caregivers to ease the level of burden experienced during caregiving included; acceptance, reprioritization, appreciation, family, positive self-view and empathy. Also, it was documented that there was a strong association between caregivers’ level of burden and coping strategies (P = 0.030). Findings also showed that age (P = 0.000), sex (P = 0.000), educational status (P = 0.000), functional ability (P = 0.000), duration of care (P = 0.000), desire to continue caregiving (P =0.000) and type of cancer (P = 0.000) were statistically significantly associated with caregivers’ coping strategies.CONCLUSION There is great recognition of the role of informal caregivers in improving the health of their relatives and family members who are chronically ill. It was recommended that support groups in collaboration with health care providers should organize a symposium for informal caregivers on the intricacies of caregiving in chronically ill patients. This would create a platform for experience sharing, information dissemination and health care professional-caregiver interaction to enhance positive caregiving outcomes.
Key Words: Caregivers’ burden; Coping strategies; Cancer patients; Nigeria; Chronically ill
INTRODUCTION
Cancer is a devastating and debilitating chronic disease that affects both the patient and family members. It is largely characterized by abnormal growth and spreads by the movement of cells to other parts of the bodyviathe blood and lymphatic system.In contrast to normal cells, ’’apoptosis’’ does not apply to cancer cells, as they continuously grow, proliferate and spread[1-3]. Currently, over 100 types of cancers have been identified. Cancer has a multifaceted etiology involving many factors which is largely influenced by a complex process known as carcinogenesis. Statistics have shown that over 50 million cancer deaths occur annually worldwide and 80% of these deaths occur in developing countries[4-5].
Cancer and cancer-related mortality are projected to increase by 50% (from 14 million to 21 million) and 60% (from 8 million to 13 million), respectively, in 2030[6].Available statistics indicated that 32.6 million people were living with cancer during the 5 years of their study in Belgium, while in America, United Kingdom, China, South Africa and Nigeria 1.7 million, 1.3 million, 2.2 million, 2.56 million and 3.47 million persons were living with cancer, respectively[5,7,8]. In Nigeria, 53064 persons died of cancer in 2008[8-9]. Nigeria is also known to have the highest cancer mortality rate in Africa with an annual death toll of 10000 persons; with an incidence of 100000, 300000 and 500000 in 1990, 2010 and 2013, respectively[6,10]and 41000 cancer-related deaths were recorded in 2014 alone[11]. The upsurge in the incidence of cancer may pose serious challenges in caregiving with its attendant burden on the patients and caregivers.
Caregivers are any unpaid persons and include blood relatives, friends and housekeepers that provide a broad range of continuous assistance in performing activities of daily living (ADL) for cancer patients for at least two months in the hospital care setting, home or community. In this study, the term informal caregivers is used interchangeably with family caregivers. Caregiver burden is tailored towards describing the physical, social, financial and psychological impact of caregiving on the caregiver’s life as perceived by the caregiver. Caregivers’ burden in this study is assessed using the Zarit Standardized Scale[12]. Coping on the other hand is an emotion-focusedvsproblem-focused approach that addresses how informal caregivers respond and act both when experiencing burden of care and when the level of exposure to burden increases using diverse adaptive manipulations. The researchers’oncology anecdotal clinical interactions with advanced cancer patients and their family caregivers prompted the assessment of burden and coping strategies among advanced cancer caregivers in Nigeria.
Literature review
Concept of caregiver: The term “caregiver” is as old as Adam[13-14]. Caregivers are specialized assistants by virtue of their role. They provide unaided assistance to people with chronic ailments[15]. It has been documented that relatives are in a better position to provide care for their loved ones during the period of terminal illness (cancer crisis)[16]. This is mostly because cancer is not a respecter of persons, and results in destabilization and burden in the family. Therefore, caregiving entails assisting with activities of daily living in those with lower functional abilities.
Providing care to a seriously ill spouse, parent or other significant person can also restrict a caregiver’s personal, psychological, social, circular and vocational opportunities, as well as create a financial burden[17-20]. The outcome of these strains can be supportive and productive or at the opposite extreme, highly stressful with physical health problems, psychological distress and increased caregiver burden. Of course, no significant difference in the magnitude of these forms of burden are perceived by cancer caregivers[21].
The concept of caregivers’ burden:The American gerontologist, Zarit[22]first defined the burden of care as “the discomfort experienced by the principal caregiver of an older family member, including the caregiver’s health, psychological well-being,finances, and social life”.Since then, there is ample evidence on the burden of caring for the aged population. For instance, O’Neillet al[23]stated that, caregivers provide clinical and supportive care to cancer patients. Caregivers vary in the types of tasks they perform, the amount of time devoted to caregiving and living standards.Caregiving is not limited to elderly persons. Diseases at varying stages such as chronic and other debilitating conditions including cancer can require caregiving. However,different views and perspectives have emerged regarding the conceptualization,definition and measurement of burden. Caregiver burden is also perceived to be “a multidimensional bio-psychosocial reaction”, “resulting from an imbalance of care demands, relative to caregiver’s personal time, social roles, physical and emotional state, financial resources and formal care resources given, and other multiple roles they fulfill”[24]. O’Neillet al[23]classified caregiver distress as caregiver burden or caregiver depression while Fortinskyet al[25]stressed that caregiver distress results from mood disturbance arising from the stress of providing care, which may manifest as a feeling of being easily bothered, fearful, isolated and lonely.
Generally, the conceptualization of burden has been deliberated in three perspectives. First, burden has been defined as “the extent of workload and measured in terms of the number and types of care tasks performed (e.g., assistance with household chores, banking tasks or personal care tasks) and or the number of hours spent performing these tasks”[26]. Secondly, burden has also been defined as “the caregiver’s judgment concerning the distress or difficulty associated with performing the care task”[20]. Thirdly, burden has been further defined as the “perceived impact of this workload on the caregiver’s life”[27]. The variation within these definitions is that burden can be objective or subjective in terms of demand. The third definition of burden is used in this study.
The burden that the diagnosis and treatment of cancer impose on family caregivers appeared in the literature during the 1980s, following the use of diagnostic related groups beginning in 1983[28]. The category of burden bearers include; the patient,family members, the clinicians and medical research personnel, Government Organizations (e.g., National Cancer Centers), spiritual leaders, and international organizations/national bodies (e.g., Cancer Society of Nigeria)[3,29-30].
Family members of cancer patients express distress in exhibiting caregiving roles and this distress can be demonstrated as fear, burden, helplessness, depression,anxiety, weight loss, inability to concentrate,etc.In the Chinese culture, family caregiving is particularly dominant in terminally ill patients. For instance, the practice of familism and filial piety have been associated with the Confucian culture[31]. Thus,children should take care of the aged, sick or even dying parents in return for the parent’s efforts in bringing them up. Also, Chinese/Taiwanese people prefer to die at home which poses significant challenges and adverse consequences for families.Caring for a cancer patient contributes to physical disease, psychiatric morbidity, and increased mortality[27].
Freedman[15]found that while men provide some level of care such as finance and other less burdensome tasks, women caregivers carry out high burden caregiving tasks such as dressing, toileting and bathing. Zarit[13]observed that women exhibit more affection, support, provide time consuming care and other caregiving responsibilities to their chronically ill patients better than their male counterparts. Men primarily support caregiving financially by delaying retirement especially for health conditions that require long-term care. However, a mixed method study carried out among advanced cancer patients reported that out of 30 patients, 80% had pain, 66.7% had vomiting, 73.3% had restlessness, 50% had dyspnea and 20% had cough[5]. These patients were unable to meet their needs by themselves and were often hospitalized for symptom management. The caregiver as the support person is responsible for providing physical, psychological, economic and social support. Actually, due to the dwindling human and material health resources in most health care systems, home health care services are essential to facilitate monitoring, symptom management and treatment of patients requiring long-term care. Therefore, there is a need to measure the burden and coping among advanced cancer family caregivers in Nigeria.
A descriptive and predictive study conducted in the Eastern United States on psychological distress, fatigue, burden of care, and quality of life in primary caregivers of patients with breast cancer undergoing autologous bone marrow transplantation(BMT) found that caregivers of patients with cancer suffer from diverse burdens such as fatigue, anxiety, and low quality of life, moderate to severe levels of burden,subjective and objective levels of burden[32]. A longitudinal study conducted in the United States assessed changes in symptom severity in caregivers of patients with advanced stage cancer and found that caregivers mostly experienced moderate and severe burden[33]. The study further reported that over 40% were at risk of distress and depression as a result of their caregiving role to patients with terminal illness. Hence,the study significantly proved that caregiving in cancer patients is risky and very burdensome.
Caregiver burden is a term used to describe the physical, social, financial and psychological impact of caregiving on the caregiver’s life as perceived by the caregiver. Caregivers in this study were assessed using the Zarit Standardized Scale[12]. This scale comprises of: Physical - bodily structures, psychological -functioning, social - interactions, and financial - funds. Caregiver burden is a condition that affects many family caregivers globally[13]. It is the physical, emotional, social and financial problems experienced by a family member caring for physically and/or mentally/terminally ill patients[2,5,34]. A large body of literature supports the fact that the caregiver’s physical, emotional, psychological, and social well-being can significantly be affected by the burden experienced during caregiving. Consequently,health care providers need to understand the burdensome nature of caregiving and which coping mechanisms can best cushion the effect of the burden which is geared towards counselling, educating and supporting care receivers in Nigeria.
It has been shown that the longer the caregiving of patients with advanced cancer,the higher the level of caregiver burden reported. Besides the limitations of cancer caregiving, developing strategies to withstand cancer patient caregiving include the following: Provision of social support, positive self-view (psychological adjustment),and religious beliefs (spiritual growth and prayers), in order to meet the social needs of the patients and enhance positive health outcomes. The development of these coping strategies in cancer caregiving have been summarized in terms of changes in spirituality, attitude to life, interpersonal relationships and change in self-view[2,35].
Caregiving experience is burdensome when patients cannot cope with the symptoms they are experiencing. Family caregivers develop numerous symptoms during the caregiving process ranging from pain, nausea, vomiting, exhaustion,fatigue, sleeplessness and weight loss, dyspnea, depression, fatigue, cough,restlessness due to low socio-economic status as well as dwindling human and material health resources. Caregiving responsibilities fall on family members in Nigeria as advanced cancer patients may require optimal care and monitoring both at home and in the hospital setting. Families of advanced cancer patients also physically,socially, psychologically and spiritually experience significant distress during caregiving.
The physical, psychological, social, spiritual and financial impact of caring and coping among primary caregivers is considerable and often negative. Ample evidence has shown that caring for an advanced cancer patient may be associated with physical problems such weight loss, sleeplessness, fatigue and exhaustion. Also, psychological symptoms such as depression, anxiety, feeling of isolation and reduced self-esteem may be experienced. They are often confronted with social burden resulting in restriction of time, disturbances in routines, diminished opportunities for leisure activities and loss of income. Recent descriptive surveys and qualitative studies of caregivers’ cancer care experiences in India and Nigeria depicts that 38.9% of caregivers of cancer patients reported symptoms of depression. 41% to 62% of the caregivers of advanced cancer patients experienced a high level of psychological burden compared to 19.2% of the general population. This high burden index was significantly associated with age and the patients’ symptoms[2-3,34,36].
The enormous problems and coping strategies encountered by caregivers of cancer patients are unknown in cancer patients. Communication with health care providers might affect caregiver burden, and less research has focused on the burden and coping (if any) with cancer care giving among caregivers generally and those treated in the University of Calabar Teaching Hospital, Calabar in Cross River State specifically. This is the reason for this research.
Coping strategies/skills among advanced cancer caregivers:Folkmanet al[37], Lazaruset al[38], Antonyet al[39], Akpan-Idiok[3]and Rahmaniet al[40]perceived ’’coping’’ as a process that explains how an individual (caregiver) responds during increased exposure to stress and when experiencing stressful stimuli (appraisal of burden). In the same studies, coping strategies were categorized as problem-focused and emotionfocused coping strategies. While emotion-focused coping strategies involve effortful strategies (interpretation of burden) that caregivers adopt to mitigate the adverse emotional outcomes instigated by stressful events, problem-focused coping strategies on the other hand, are aimed at ameliorating the negative impact of the burden using problem-solving mechanisms or eliminating the sources of stress by building up positive/negative coping such as adaptive or maladaptive coping strategies. In advanced cancer caregiving, caregivers use both adaptive and maladaptive coping strategies which can affect families’ caregiving outcomes[41]. Rahmaniet al[40]in their study also pinpointed that repudiation of patients/family members with terminal illness (e.g., mental illness) was identified as a major predictor of caregivers’ burden.As a result, such patients may be abandoned to psychiatric services. Furthermore,cultural roles, religious beliefs and social structure are strongly associated with family caregiving and the cancer disease process that involves the family system and acts as coping precursors among advanced cancer family caregivers. These forms of coping strategies based on whether they are harmful or helpful (e.g., emotion-focusedvsproblem-focused coping; approachvsavoidance) are related to cultural context.Osundinaet al[42]found no statistically significant relationship between burden and coping styles among schizophrenic family caregivers. Groveret al[4]also argued that caregivers’ coping strategies can directly or indirectly influence patient health outcomes.
Turnbullet al[43]documented that the caregivers’ burden level was high and that the extent to which caregivers experience symptoms depends largely on their coping skills, energy level, health status, belief system and personality. Also, Sisk[20]observed that as the burden of caregiving increases, it disrupts daily activities, social relationships and negatively affects resources. According to the cancer palliative care module, “participating in a network of caring and reciprocal relationships with others and creating a sense of belonging and reason for living that transcends one’s individual self or social support, has been found to be one of the most important coping mechanisms”[44]. The understudy of burden and the coping strategies employed by family caregivers in their caregiving roles can enhance needs assessment for designing family—centered interventions to ameliorate cancer caregiving burden in Nigeria. To meet the gaps, this study was directed by role and stress theories to answer the research questions: What are the perceived challenges that deter family members and relations from cancer caregiving? What are the perceived sustaining factors to cancer caregiving in Nigeria and in the University of Calabar Teaching Hospital, Calabar?
MATERIALS AND METHODS
Study area
The study area is the University of Calabar Teaching Hospital (UCTH) situated in the southern part of Nigeria. UCTH is a tertiary health institution that is poised to provide highly specialized health care services. It also serves as a research and training center for health care professionals. The hospital serves as a referral center to other health centers, clinics and health institutions where cancer patients are admitted and managed. The hospital is compartmentalized into major wards which include;medical, surgical, orthopedic, pediatrics, obstetrics and gynecology wards. Although there is no specific section for management of cancer patients in the hospital, the gynecological ward, female/male surgical ward and medical out-patient department(MOPD) have been designated to provide care to cancer patients.
Study design, study population and sample size
The study adopted a descriptive cross-sectional study as used by other authors to conduct similar studies[23-24]. The study population consisted of informal family caregivers providing services to histologically diagnosed cancer patients receiving treatment at UCTH at the time of the survey. As the population size was unknown,this study adopted the Power Analysis Calculation by Cohen[45]to deduce the required sample size. The power analysis was used to determine the minimum sample size for inferential statistical analysis (given that, the level of significance α = 0.05; expected effect size = 0.95). Using the Sample size Power Analysis software (G. Power 3.1.5) the calculated sample size was 210. However, to account for attrition, wrongly filled and incomplete questionnaires, the sample size was increased by 16% to obtain an actual sample size of 250 informal family caregivers for the study. The current study is a follow-up from a previous key research on caregiver’s perceptions of advanced cancer caregiving burden in Nigeria[2]. Eligible caregivers from the previous research who gave their consent to participate in the study were recruited. The inclusion criteria consisted of; all advanced cancer family caregivers aged 18 years and above who demonstrated enthusiasm to participate in the study, who resided within the study area and have provided care to the patient for two months or more. The current study describes family cancer caregivers’ as unpaid persons (blood relatives, friends and house-keepers) aged 18 years and above who provide assistance to cancer patients for a minimum of two months in the study location[2].
Instruments used for data collection
The instruments used for data collection were a researcher-developed structured questionnaire, adopted 22-item standardized validated Zarit Burden Interview (ZBI)and 17-item adapted modified Coping Orientation to Problems Experienced (COPE)Inventory. The questionnaire consisted of 67 items divided into the following five sections: Section A: Socio-demographic, characteristics and duration of caregiving,Section B: Functional level of caregivers, Section C: Coping strategies of caregivers,Section D: Desire to continue with caregiving and Section E: Level of burden of caregivers. For functional ability of care receivers, a score of ≥ 50% indicates low functional ability and vice versa for high functional ability (reliability coefficient =0.87-0.93).
The modified ZBI scale is made up of 22 items which reflects how people sometimes feel when caring for other people. The ZBI scale is a 22-item questionnaire with each item rated from 0-88 (higher score denotes higher burden for a particular item). The total burden for a subject is the sum of the scores in all the items endorsed. The total score for the scale ranges from 0 to 88 on a five-point Likert scale. To measure the burden level of caregivers, the following scale was used; 0-20 represented little or no burden; 21-30 signified mild burden; 31-40 denoted moderate burden and 41-88 represented severe burden level. The psychometric properties of the ZBI scale include an acceptable inter-item reliability and convergent validity indicated by a Cronbach alpha of 0.79 and a correlation coefficient of 0.71 between caregiver global evaluation and scores was reported[46]. A test-retest reliability of 0.71 and internal consistency(Cronbach alpha = 0.91) was also reported[2-3,22,34].
The modified COPE Inventory was adopted to analyze the coping mechanism used by caregivers when confronted with the burden of caregiving. The inventory was designed using a four-point Likert scale. The COPE Inventory has been validated and widely used in Nigeria and shows evidence of factor replicability[47-50]. A validity and reliability test of the COPE inventory showed high internal consistency of 0.83 and 0.72, respectively.
Validity and reliability
The researcher adopted the face and content validity approach to establish the validity of the instrument as asserted by Politet al[51]who stated that “the face validation of a standardized instrument is appropriate for any measuring scale”. This was achieved by engaging two experts with similar research experience especially in relation to care for cancer patients for scrutiny, examination and useful inputs. Their inputs were noted and harnessed into the instruments before using it for data collection.
The researcher also adopted a test-retest method to establish the reliability of the instruments. The instruments were administered to 20 male and 20 female informal caregivers in Port Harcourt, River State, Nigeria on two different occasions with a two week interval. Thereafter, their responses were collated and analyzed using the Pearson Product Moment Correlation Coefficient to obtain a reliability score ranging from 0.85 to 0.96 across all items of the variables. However, Kerlinger[52]noted that a reliability coefficient of 0.50 and above is appropriate for any measuring scale, hence,the instruments in the current study were considered appropriate for use.
Method of data analysis
Data gathered from the respondents were collated, coded and analyzed using Statistical Package for Social Sciences (SPSS version 20.0) software and Predictive Analytical Software (PAS version 19.0). Descriptive statistics such as percentages,mean, and standard deviation were used to analyze the variables highlighted in the research objectives. Chi-square was used to test for association between categorical variables at the 0.05 level of significance. Results are presented in tables and charts.
Ethical consideration
Ethical approval was obtained from the UCTH Research Ethics Committee. Thereafter,written informed consent was obtained from the study participants after adequately informing them about the nature, purpose and significance of the study. The study participants were also assured of strict anonymity and confidentiality regarding the information they would provide. The study participants were informed that participation in this study was on a voluntary basis and they had the right to withdraw at any stage of the study without victimization or coercion.
RESULTS
Socio-demographic characteristics of the respondents
Of the 250 questionnaires distributed, 210 were completely filled and returned for analysis giving a response rate of 84%. The results which are presented in Table 1 show that 132 (62.9%) respondents were female and 78 (37.1%) were male. Almost half of the respondents 97 (46.2%) were aged between 31-50 years, 98 (46.7%) were married, 83 (39.6%) had secondary education, 81 (38.6%) were unemployed and almost two-thirds [132 (62.9%)] were the parents of caregivers.

Table 1 Socio-demographic characteristics of the respondents (n = 210)
Caregivers’ perceived level of caregiving to advanced cancer patients
The results presented in Figure 1 were analyzed using the Zarit Burden Scale analytical guideline and the respondents’ scores were categorized as trivial or no burden (0-20), mild (21-30), moderate (31-40) and severe burden (41-88). The results showed that a significant proportion of the respondents [97 (46.2%)] experienced severe burden, 76 (36.2%) experienced moderate burden and 37 (17.6%) experienced trivial or no burden.

Figure 1 Burden level of caregivers.
Coping styles adopted by caregivers to care for advanced cancer patients
The coping styles highlighted in Table 2 were analyzed using the COPE inventory which is often used to assess the psycho-social characteristics of caregiving and other stressful events experienced by individuals (Osundinaet al[42], 2017). The coping strategies were then categorized into two parts: Problem-focused coping strategies(acceptance, appreciation and reprioritization) and emotion-focused coping strategies(family, positive self-view and empathy) (Table 2). From the results, it was observed that higher means were reported for nearly all the assertions except for two which recorded lower mean values.
To measure the level of effectiveness of coping styles adopted by caregivers in providing care for advanced cancer patients, responses from the respondents were assessed based on their individualized mean score where a mean score between 0-2.99 denoted ineffective coping strategies while a mean score of ≥ 3.00 denoted effective coping strategies. The results in Figure 2 show that 185 (88.1%) caregivers indicated that the coping strategies used were effective in caregiving while 25 (11.9%) indicated that the coping strategies used was ineffective.
Relationship between caregivers’ characteristics and coping strategies
The results presented in Table 3 show the relationship between caregivers’characteristics and effectiveness of coping strategies adopted. These results show that sex (χ2= 14.77;P= 0.000), age (χ2= 17.79;P= 0.000) and educational status (χ2= 48.45;P= 0.000) were all statistically significantly associated with caregivers’ coping strategies.This implies that age, sex and educational status have a significant influence on the level of effectiveness of coping strategies used by caregivers. From the table, it can be observed that middle-aged female caregivers with higher educational status attest to the fact that their choice of coping strategies was very effective compared to their counterparts.
Association between caregivers’ perceived burden level and coping strategies
The results presented in Table 4 show the association between caregivers’ perceived burden level and coping strategies. It can be seen that there is a strong association between caregivers’ perceived burden level and coping strategies (χ2= 6.94;P= 0.030).This implies that the more effective the coping strategies, the lesser the burden andvice versaas demonstrated in Table 4.
Relationship between functional level of the care receiver (cancer patient) and caregivers’ coping strategies
Functional ability was measured with simple percentages using a 15-item questionnaire (physical status assessment tool) designed by the researcher. From the analysis, the results show that care receivers are highly dependent on caregivers inperforming their routine daily activities except for grooming (brushing hair, teeth),taking medication, using the telephone and wandering which needs less supportive care (Table 5). It was further observed that 137 (65%) exhibited low functional ability while 73 (35.0%) showed high functional ability.

Table 2 Coping styles adopted by caregivers to care for advanced cancer patients
The results in Table 6 show that the relationship between functional ability and the caregivers coping strategies was statistically significant (χ2= 17.35;P= 0.000). This implies that coping strategies were more effective amongst caregivers providing care to patients with low functional ability (Table 6).
Relationship between duration of care and caregivers’ coping strategies
The results presented in Table 7 show that the relationship between duration of care and caregivers’ coping strategies was statistically significant (χ2= 17.72;P= 0.000). This analysis implies that the longer the duration of care, the higher the need to adopt more effective coping strategies.
Relationship between desire to continue caregiving and caregivers’ coping strategies
The results presented in Table 8 show that the desire to continue caregiving was statistically significantly associated with caregivers’ coping strategies (χ2= 21.19;P=0.000). It was further observed that effective coping strategies serve as an impetus to continue providing care to cancer patients. The desire to continue with care was significantly dependent on the level of efficacy of the coping strategies used.
Test of association between type of cancer and caregivers’ perceived burden level
The results presented in Table 9 show that types of cancer were statistically significantly associated with caregivers’ burden level (χ2= 59.01;P= 0.000). It wasfurther observed that caregivers experience severe burden mostly during caregiving of prostate [44 (72.1%)] and colorectal cancer patients [9 (60.0%)], while moderate burden was higher for those with breast cancer [44 (62.8%)] and cervical cancer [15 (34.8%)].No burden was mostly reported for those with human immunodeficiency virus (HIV)-related cancers [5 (62.5%)].
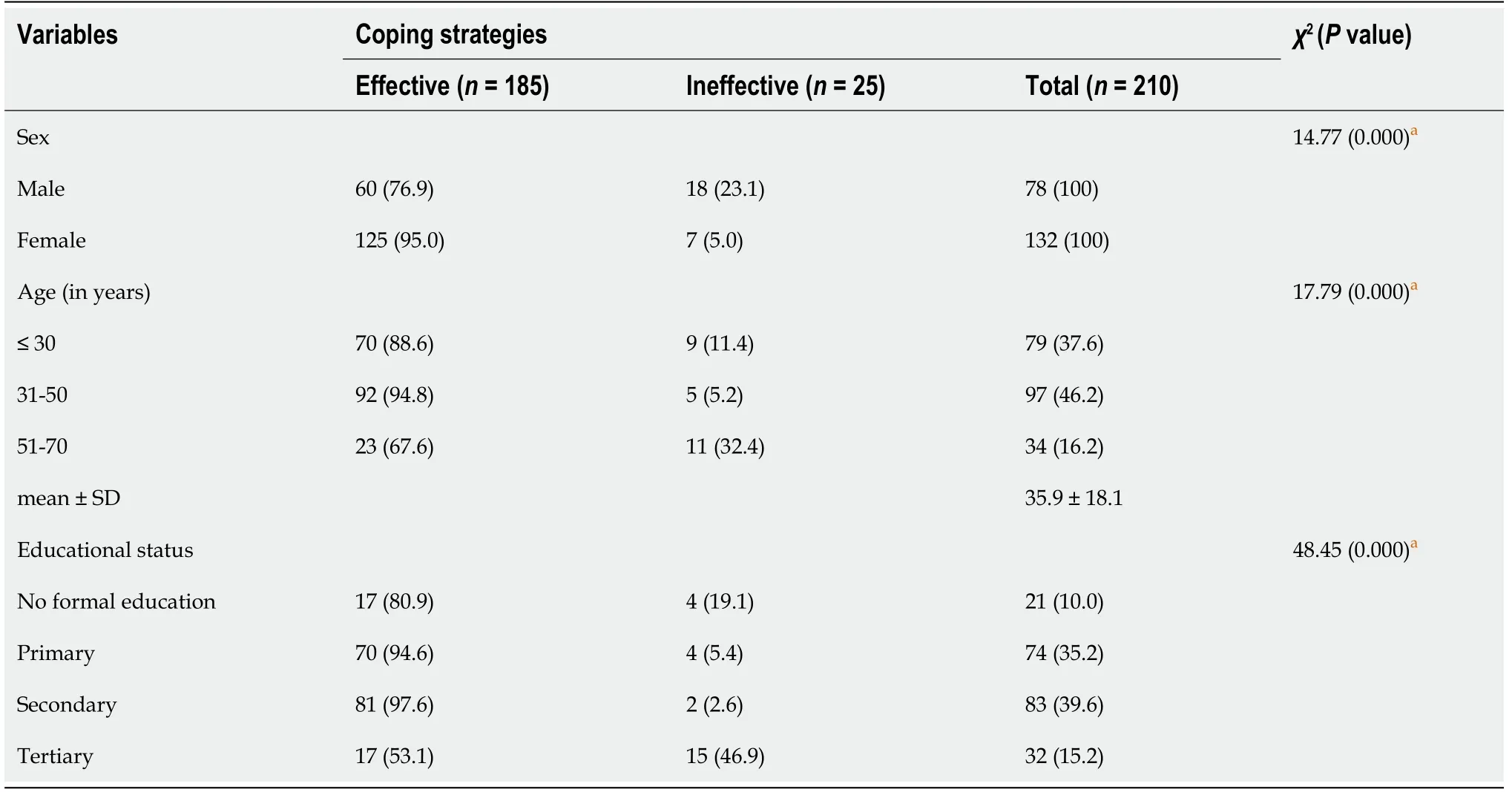
Table 3 Relationship between caregivers’ characteristics and coping strategies

Table 4 Association between caregivers’ perceived burden level and coping strategies
Test of association between type of cancer and caregivers’ coping strategies
The results presented in Table 10 show that types of cancer were not statistically significantly associated with caregivers’ coping strategies (χ2= 7.00;P= 0.320). It was further observed that caregivers’ coping strategies were more effective for patients with breast cancer, Hodgkin’s lymphoma and HIV-related cancer than other types of cancer.
DISCUSSION
In Nigeria, it has been reported that family members often serve as informal caregivers mostly at home to their relatives with chronic health conditions during the management, treatment and recovery process[2,42]. However, this role of caregiving consequently places a huge demand on the caregivers’ social, financial and personal resources which becomes onerous. Hence, for continuous caregiving of cancerpatients, it has become imperative for caregivers to adopt suitable coping strategies that would serve as an impetus for optimal caregiving. The findings in the current study showed that nearly two-thirds of the study participants were female (Table 1).These results are in accordance with a similar study conducted by Akpan-Idioket al[2],where female caregivers dominated in their study. Female dominance in caregiving islinked to the fact that they are mostly in charge of indoor activities especially with regard to providing care and support to family members/relatives in all aspects,whereas males tend to lead in out-door activities (e.g., providing financial resources).Historically, it can also be argued that women have a natural gift for caregiving than their male counterparts[32,53]. Almost 50% of the respondents were married and young.These results is in accordance with other studies that confirmed that most caregivers to patients with chronic health problems are middle aged[12,31,34]. Givenet al[24]asserted that since most cancer patients are aged 40 years and above, it is appropriate that younger and active persons care for them. Also, experience in providing emotional and psychological support to family members with ill-health may also account for the high number of caregivers who are married. From the results in Table 1, parents of caregivers were the largest category of care receivers. This is not surprising as cancer affects mostly older adults. As a result, their children and other relatives care for them.This finding is congruent with other studies which reported that care receivers were mainly parents and a partner/spouse[33,54].

Table 5 Functional status of care receivers

Table 6 Relationship between functional level of the care receiver (cancer patient) and caregivers’ coping strategies

Table 7 Relationship between duration of care and caregivers’ coping strategies

Table 8 Relationship between desire to continue caregiving and caregivers’ coping strategies
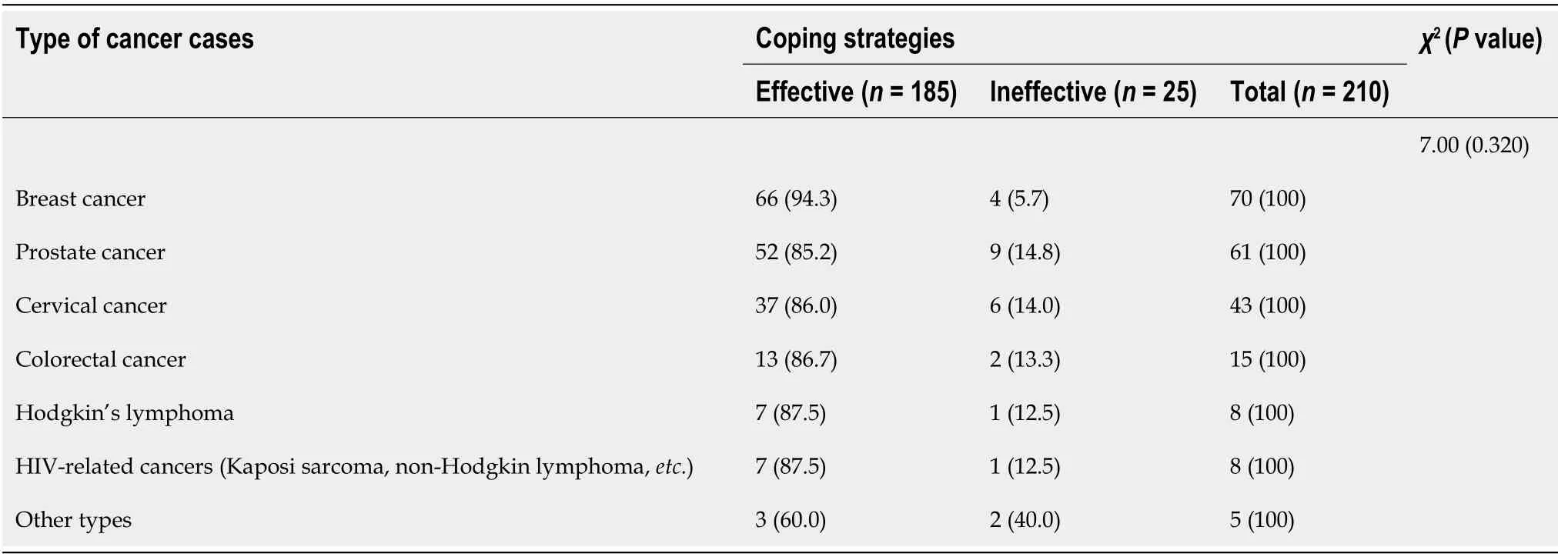
Table 10 Association between type of cancer and caregivers’ coping strategies

Figure 2 Effectiveness of caregivers’ coping strategies.
The findings in the current study also showed that nearly 50% of the respondents[97 (46.2%)] experienced severe burden, while another 113 (53.8%) experienced moderate or no burden (Figure 1). These results were similar to those reported in other studies where most caregivers experienced severe burden[32,55]. This implies that most caregivers bear all the responsibilities of caring for their patients (which in most cases are their parents) and as such their personal, financial and social support places a huge burden on them. This is different for others who experience a moderate or trivial burden where responsibilities may be shared amongst other family members. This means that there is access to all forms of human and material resources to provide optimum care for cancer patients. It was observed that there is a strong association between caregivers’ perceived burden level and coping strategies. This implies that the level of burden experienced by caregivers is significantly dependent on the coping strategies adopted. As shown in Table 4, caregivers with effective coping strategies can diminish their level of burden. This finding contradicts a Nigerian study where the relationship between level of burden and caregivers’ coping strategies was not statistically significant[42].
Coping strategies adopted by caregivers, as presented in Table 2, include both problem-focused coping strategies (acceptance, appreciation and reprioritization) and emotion-focused coping strategies (family, positive self-view and empathy). Analysis showed that over two-thirds of caregivers [185 (88.1%)] indicated that the coping strategies used were effective (Figure 2). The efficacy of the caregivers’ coping strategies may largely be determined by their impact on reducing the level of burden experienced during caregiving. Thus, the more effective the coping strategies, the lesser the burden. These results were similarly documented by Osundinaet al[42]where a number of coping styles were identified including appreciation, emotional support,acceptance, planning, suppression, mental disengagement, religious coping,etc.Coping strategies are designed to motivate and encourage caregivers in providing care to cancer patients despite the challenges they often encounter.
The relationship between caregivers’ characteristics (age, sex and educational status) was significantly associated with the caregivers’ coping strategies. As shown in Table 3, it was also observed that middle-aged female caregivers with higher educational status tend to have more effective coping strategies compared to their counterparts. In Nigeria, middle-aged individuals (31-50 years) are considered the most economically active group compared to other age groups. As such, they often demonstrate the capacity to deal with other forms of burden experienced during caregiving with an expedient coping mechanism. This explains why caregivers aged 31-50 years deal with the burden of caregiving better than other age groups as reported in other studies[2,34]. The results also showed that females demonstrated better coping strategies than their male counterparts. This is principally linked to the fact that about two-thirds of the respondents were female. Besides the current study, ample evidence has also confirmed that informal caregivers are mostly female and experience higher levels of burden compared to their male counterparts[2,3,46,56,57,60]. This is primarily because females are delegated to perform cultural subservient roles irrespective of age.As a result, they experience high levels of burden which require the adoption of effective coping strategies to continue providing care to cancer patients. It was also observed that caregivers with higher educational status adopted more effective coping strategies than their counterparts. The demonstration of adequate knowledge and skills in coping with the burden experienced during caregiving may be why caregivers with effective coping strategies were mostly those with higher educational status. As opined by Akpan-Idioket al[14], caregivers with higher educational status are equipped with a broader repertoire of coping strategies geared towards solving problems rather than assessing the onerous nature of caregiving.
With regard to functional ability, the results showed that about two-thirds of the care receivers [137 (65%)] had low functional ability. As such, caregivers are susceptible to a higher burden during caregiving. This was also observed in other studies where functional impairment significantly contributed to the burden level of caregivers[24,27,39,54,58]. This explains why they demonstrated better coping strategies compared to other caregivers. In the current study, it was also documented that the relationship between functional ability and caregivers’ coping strategies was statistically significant (P= 0.000) (Table 6). This implies that care receivers with low functional ability present a high level of burden to caregivers; thus, adopting expedient coping strategies would guarantee continuous caregiving by these caregivers.
The results presented in Table 7 show that the relationship between duration of care and caregivers’ coping strategies was statistically significant (P= 0.000). This implies that the longer the duration of care, the higher the need to adopt more effective coping strategies. This is because, longer duration of care demonstrated a strong correlation with higher burden level as confirmed in previous studies[34,39,58]. Hence, the more time spent on caregiving, the higher the burden and the higher the need for effective coping strategies. The results also documented that the desire to continue caregiving was statistically significantly associated with caregivers’ coping strategies (P= 0.000). It was further observed that effective coping strategies serve as an impetus to continue providing care to cancer patients. The desire to continue in care may largely be dependent on the level of efficacy of coping strategies used. With regard to the types of cancer and caregivers’ burden level, caregiving in prostate and colorectal cancer patients resulted in a much greater burden than other types of cancer (Table 9). This may be linked to the extent of discomfort, stage of cancer and health status of the patients. This implies that the severity of caregiver’ burden level can be assessed by the type of cancer involved.
CONCLUSION
There is great recognition of the role of informal caregivers in improving the health of their relatives and family members who are chronically ill. Findings in the current study identified coping strategies used by caregivers to ease the level of burden experienced during caregiving and these mechanisms include; acceptance,reprioritization, appreciation, family, positive self-view and empathy. Also, it was documented that there is a strong association between caregivers’ level of burden and coping strategies (P= 0.030). It was also observed that age, sex, educational status,functional ability, duration of care and desire to continue caregiving were statistically significantly associated with caregivers’ coping strategies. Based on the above findings, it was recommended that support groups in collaboration with health care providers should organize a symposium for informal caregivers on the intricacies of caregiving to chronically ill patients. This would create a platform for experience sharing, information dissemination and health care professional-caregiver interaction.To mitigate the burden of caregiving, it was also recommended that policy makers enact policies that would ensure that chronically ill patients have access to material and financial support and should be the collaborative responsibilities of the government, non-governmental organizations and other support groups. Further studies on caregiver’s burden level and coping strategies among patients with comorbidities should also be carried out.
ARTICLE HIGHLIGHTS
Research background
Nigeria is known to have the highest cancer mortality rate in Africa with an annual death toll of 10000 persons; with a cancer incidence of 100000, 300000 and 500000 in 1990, 2010 and 2013, respectively, and 41000 cancer-related deaths were recorded in 2014 alone. The upsurge in the incidence of cancer may pose serious challenges in caregiving with its attendant burden on the patients and caregivers. The physical,psychological, social, spiritual and financial impact of caregiving is considerable and often negative. Ample evidence has shown that caring for an advanced cancer patient may be associated with physical problems such as weight loss, sleeplessness, fatigue and exhaustion. Also, psychological symptoms such as depression, anxiety, feeling of isolation and reduced self-esteem may be experienced. They often cause a social burden resulting in restriction of time, disturbances in routines, diminished opportunities for leisure activities and loss of income. Recent descriptive surveys and qualitative studies of caregivers’ cancer care experiences in India and Nigeria show that 38.9% of caregivers of cancer patients reported symptoms of depression. 41% to 62% of caregivers of advanced cancer patients experienced a high level of psychological burden compared to 19.2% of the general population.
Research motivation
Cancer is a devastating and debilitating chronic disease that affects both the patient and family members. Available evidence has confirmed that the care of chronically ill relatives by family members can be very challenging. This is because caregiving of cancer patients often presents a high level of burden on the caregivers. Consequently,this requires the adoption of coping mechanisms to cushion the effect of the burden experienced during caregiving.
Research objectives
To determine the burden experienced and coping strategies among caregivers of advanced cancer patients attending University of Calabar Teaching Hospital (UCTH),Cross River State, Nigeria.
Research methods
The study adopted a descriptive cross-sectional study design and the study population consisted of informal family caregivers providing services to histologically diagnosed advanced cancer patients receiving treatment at the UCTH as at the time of the survey.A researcher-developed structured questionnaire, a 22-item standardized validated Zarit Burden Interview (ZBI) and a modified 17-item Coping Orientation to Problems Experienced (COPE) Inventory were used to collect data from 250 eligible informal caregivers who were selected with regard to caregiver’s characteristics, caregivers’level of burden and caregivers’ coping strategies, respectively. Data gathered from the respondents were collated, coded and analyzed using Statistical Package for Social Sciences (SPSS version 20.0) software and Predictive Analytical Software (PAS version 19.0). Chi-square was used to test for associations between categorical variables at the 0.05 level of significance. Results are presented in tables and charts.
Research results
Assessment of burden level revealed that a reasonable proportion of the caregivers [97(46.19%)] experienced severe burden, and 37 (17.62%) experienced trivial or no burden, while 76 (36.2%) perceived moderate burden. The results showed that the coping strategies used by caregivers to ease the level of burden experienced during caregiving included; acceptance, reprioritization, appreciation, family, positive selfview and empathy. It was also found that there was a strong association between caregivers’ level of burden and coping strategies (P = 0.030).
Research conclusions
There was a strong association between socio-demographic characteristics (age,education, functional ability, desire to continue caregiving, types of cancer) and caregivers’ coping strategies
Research perspectives
Further studies on caregiver’s burden level and coping strategies in patients with comorbidities should also be carried out.
 World Journal of Clinical Oncology2020年12期
World Journal of Clinical Oncology2020年12期
- World Journal of Clinical Oncology的其它文章
- COVID-19 and information and communication technology in radiation oncology: A new paradigm
- Practice change in the management of metastatic urothelial carcinoma after ASCO 2020
- Stereotactic body radiation therapy: A good dance partner of oligometastatic non-small cell lung cancer to the sound of SINDAS study
- New standard in locally advanced rectal cancer
- Predictive indicators of successful tyrosine kinase inhibitor discontinuation in patients with chronic myeloid leukemia
- Fluoropyrimidine-induced cardiotoxicity