
Classic Ehlers-Danlos syndrome and cardiac transplantation-Is there a connection?
2020-11-05 00:21:22MerlinButler
World Journal of Cardiology 2020年8期
Merlin G Butler
Abstract
Key words:Ehlers-Danlos syndrome;Next-generation sequencing;Surgical complications;Beighton hypermobility scale;Cardiac failure and transplantation
INTRODUCTION
Ehlers-Danlos syndrome(EDS)is a connective tissue disorder comprised of several types due to mutations in genes encoding proteins(e.g.,collagen)such as COL5A1 and COL5A2 accounting for 50% of patients with a clinical diagnosis of classic EDS[1].Classic EDS is an autosomal dominant disorder identified in one in 20000 individuals with stretchable skin,delayed wound healing with poor scarring,joint hypermobility with subluxations or dislocations,pes planus,easy bruisability,hernias,aneurysms,and cardiac abnormalities[2-4].Historically,EDS is grouped into six categories(classic,hypermobile,vascular,kyphoscoliosis,arthrochalasia and dermatosparaxis)with different genetic causes and inheritance patterns[4,5].In 2017,EDS was assigned into 13 heritable disorders that affects an estimated 10 million people worldwide.These disorders are:Autosomal dominant classic(cEDS);autosomal recessive classic-like(clEDS);autosomal recessive cardiac-valvular(cvEDS),autosomal dominant vascular(vEDS),autosomal dominant hypermobile(hEDS),autosomal dominant arthrochalasia(aEDS),autosomal recessive dermatosparaxis(dEDS),autosomal recessive kyphoscoliosis(kEDS),autosomal recessive brittle cornea syndrome(BCS),autosomal recessive spondylodysplastic(spEDS),autosomal recessive musculocontractural(mcEDS),autosomal dominant or recessive myopathic(mEDS),and autosomal dominant periodontal[6].
Advances in genomics technology using next-generation sequencing(NGS)has led to the discovery of causative genes along with candidate gene approaches,disease specific panels or whole-exome analysis in patients presenting with features of a connective tissue disorder with newer classifications.Applying genomics to the field of cardiovascular-related disorders has identified over 80 genes causing connective tissue disorders using available comprehensive NGS gene testing panels.Over 150 genes have been identified playing a role in hereditary cardiomyopathies including hypertrophic,dilated or left ventricular non-compaction cardiomyopathy and hereditary arrhythmogenic right ventricular cardiomyopathy but do not include collagen genes.In addition,over 250 genes are found on commercially available comprehensive cardiovascular disease NGS panels with at least three collagen(i.e.,COL3A1,COL5A1,COL5A2)genes(e.g.,Fulgent Diagnostics,Irvine,CA,United States)and advanced genetic testing should be applied to interrogate gene panels for cardiology services including for heart transplantation[7].
A 13-year-old son with features of a connective tissue disorder was identified previously based on a physical examination with hypermobility assessed using the Beighton scale[8,9].His numerical rating score was high at 8 out of 9 with scores greater than 5 indicative of a connective tissue disorder.The score comprised passive dorsiflexion of the fifth finger beyond 90°(one point),passive bilateral apposition of both thumbs to the flexor aspects of forearms(two points),hyperextension of the elbows beyond 180°(two points),hyperextension of the knees beyond 180°(two points),and forward flexion of the trunk with palms of hands resting on the floor(one point).He had no heart murmur and a previous echocardiogram showed normal intra-cardiac anatomy and size,but his aortic root was dilated.A comprehensive connective tissue disorder NGS gene panel consisting of 50 genes was ordered and performed at the University of Nebraska Medical Center(Omaha,NE,United States).A heterozygous missenseCOL5A1gene variant was found involving exon 3 at nucleotide c:305T>A with an amino acid position change at p.Ile102Asn.This gene variant was also found in his 55-year-old father exhibiting similar clinical features of thin stretchable skin with poor atrophic scars,hypermobility,joint pain and easy bruising with increased pigment on the anterior surface of both lower legs.Due to multiple knee surgeries in the past,bilateral knee movement or range could not be assessed,none-the-less his Beighton hyperflexibility score was 6 out of 7(excluding knee mobility measures)(see Figure 1).Interestingly,his father had a heart transplant at 43 years of age due to cardiac failure with no known cause identified including infections,anatomic defects or metabolic problems.There was also no evidence of a spontaneous dissection or closure of a main coronary vessel causing infarction and subsequent heart failure.
TheCOL5A1gene encodes one of the low abundant fibrillar collagens related to connective tissue abnormalities and when disturbed leads to autosomal dominant classic EDS[6].The gene variant seen in the father and his son has not been described previously and the amino acid substitution was considered harmful by computer in silica prediction programs impacting protein structure.
The father’s cardiac failure was of unknown cause and required a heart transplant,potentially attributable to a connective tissue disorder that should be brought to medical attention as congestive heart failure affects 23 million people worldwide including 7.5 million in North America.It has a prevalence of 2.6% in the United States population in those greater than 20 years of age[10].It is estimated that about 90000 heart transplants have occurred worldwide since 1983 with a current median survival rate of 50% at 12 years[11,12].
The clinical presentation and autosomal dominant inheritance pattern in this family involving a disturbed connective tissue gene leading to classic Ehlers-Danlos syndrome should be of interest to cardiologists,heart transplant specialists and surgeons with a possible relationship to cardiac involvement and heart failure requiring transplantation.Complications of connective tissue disorders should be recognized early and avoided in those patients due to their poor wound healing,scarring and other tissue involvement(e.g.,vascular anomalies,blood pressure instability,aneurysms)and taken into consideration prior to surgical intervention.
CONCLUSION
Patients with unexplained heart failure should be checked for hypermobility(e.g.,use of the Beighton scale)and genetically tested for connective tissue disorders using readily available comprehensive NGS gene panels prior to seeking heart transplantation.Evaluating and reporting of other similarly affected patients with genetic testing is encouraged to further elucidate whether connective tissue disorders may play a role in a subset with heart failure requiring transplantation as seen in this patient.In addition,complications of those having connective tissue disorders such as Ehlers-Danlos syndrome may necessitate closer surveillance and monitoring during and after surgical intervention with prolonged recovery and healing,as well as counseling of at-risk family members requiring screening and advanced genetic testing.
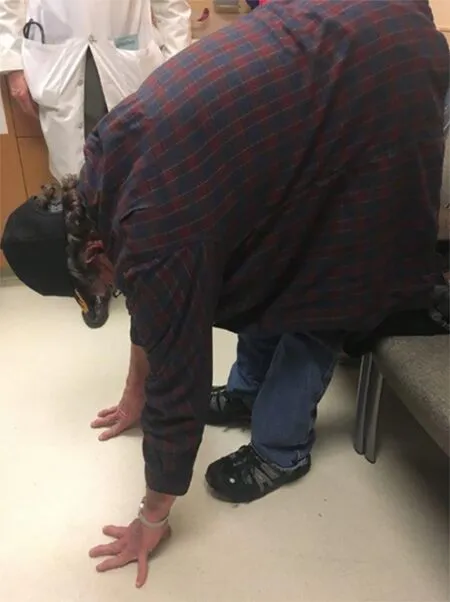
Figure 1 The 55-year-old father with classic Ehlers-Danlos syndrome and hypermobility is illustrated by placing palms on the floor.
ACKNOWLEDGEMENTS
The author recognizes Waheeda Hossain,MD for expert preparation of the manuscript.
 World Journal of Cardiology2020年8期
World Journal of Cardiology2020年8期
- World Journal of Cardiology的其它文章
- Oliver Wendell Holmes’1836 doctorate dissertation and his journey in medicine
- Systematic review and meta-analysis of outcomes of anatomic repair in congenitally corrected transposition of great arteries
- Impact of cardiologist intervention on guideline-directed use of statin therapy
- Forensic interrogation of diabetic endothelitis in cardiovascular diseases and clinical translation in heart failure
- Sympathetic nervous system activation and heart failure:Current state of evidence and the pathophysiology in the light of novel biomarkers