
Anti-N-methyl-D-aspartate-receptor antibody encephalitis combined with syphilis:A case report
2020-09-15 08:58
World Journal of Clinical Cases 2020年12期
Xi-Yu Li,Graduate School,Tianjin Medical College,Tianjin 300070,China
Zhi-Hong Shi,Ya-Lin Guan,Yong Ji,Tianjin Key Laboratory of Cerebrovascular and Neurodegenerative Diseases,Tianjin Dementia Institute,Department of Neurology,Tianjin Huanhu Hospital,Tianjin 300350,China
Yong Ji,China National Clinical Research Center for Neurological Diseases,Department of Neurology,Beijing Tiantan Hospital,Capital Medical University,Beijing 100070,China
Abstract
Key words:Anti-N-methyl-D-aspartate receptor encephalitis;Syphilis;Imaging manifestations;Treatment;Methylprednisolone;Immunoglobulin;Case report
INTRODUCTION
Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis may be associated with antibodies against neuronal synaptic proteins.Since the discovery of anti-NMDAR encephalitis in 2007,it has been a popular area of research in the field of neurology.Anti-NMDAR encephalitis is primarily diagnosed in children and young adults,with or without an associated tumor;it responds to treatment but can relapse[1].Malignant tumors associated with anti-NMDAR encephalitis predominantly present between the ages of 12 and 45 years;most cases are ovarian teratomas (94%),followed by extraovarian teratomas (2%) and other tumors (4%)[2].The presence of a tumor(usually an ovarian teratoma)[3]depends on age,gender,and ethnicity and is more common in women over 18 years of age[1].Patients with anti-NMDAR encephalitis can present with a variety of clinical symptoms,such as abnormal (psychiatric) behavior or cognitive dysfunction,speech dysfunction,seizures,movement disorder,dyskinesias,decreased level of consciousness,autonomic dysfunction,or central hypoventilation,among others[4].The most common dyskinesias are orofacial dyskinesias,dance prosthetic deformities,and dystonia[1].
CASE PRESENTATION
Chief complaints
The patient was a 32-year-old man who was admitted to our hospital with complaints of cognitive function decrease,diplopia,and unsteady gait for more than 6 mo.
History of present illness
More than 6 mo prior to admission,he developed diplopia and his right eye showed outward inclination after long-term emotional stress and fatigue.Because the lower limbs were difficult to control when walking,he reported an unstable gait.He also experienced memory loss and personality changes,and his family felt that his personality became naive.
History of past illness
He had a remote history of blood transfusion during leg surgery.He denied a history of infection,diarrhea,fever,or other previous medical history.
Personal and family history
The patient was a married 32-year-old man with a height of 180 cm and weight of 62.5 kg.He had no history of drug use,drinking,or bad sexual life,but had a history of smoking.His parents are both in good health.
Physical examination upon admission
He lost 15 kg in 1 mo.On assessment,his vital signs and eye movement were normal.Clinical neurological examination revealed slow response,right eye abduction,diplopia,personality change,attention and short-term memory impairments,euphoric mood,static and postural tremor of the head and limbs,positive left Babinski sign,and limb ataxia,without any other pathological signs.Our primary clinical consideration was neurosyphilis,followed by intracranial infection.
Laboratory examinations
There were no significant abnormalities on routine blood tests,including biochemistry,coagulation,high-sensitivity C-reactive protein,and pelvic and liver tumor markers.The syphilis rapid plasma responsive ring card test was positive (1:2).Electroencephalogram,brain electrical activity mapping,and electromyography were normal.Oncologic tests,including chest computed tomography,CA199,and carcinoembryonic antigen,were all negative.The patient’s score on the Montreal Cognitive Assessment examination was 24/30.His Mini-Mental State Examination score was 28/30.
Imaging examinations
Brain magnetic resonance imaging (MRI) scans 1 mo before admission showed T2hyperintensity of the brain stem,bilateral internal capsules,and the right frontal lobe;the right ventricle was enlarged (Figure1).Repeat brain MRI scans on admission showed abnormal symmetrical signals in the pons,mesencephalon,bilateral medial temporal lobe,and bilateral basal ganglia (Figure2).
Further diagnostic work-up
Lumbar puncture showed normal cerebrospinal fluid (CSF) with routine testing,including biochemistry and cytology.The immunoglobulin G (IgG) index was 2.95 mg/dL.Because neurosyphilis was considered,ceftriaxone 1.0 g im QD was given for 15 d,but the patient's condition was not improved.Repeat lumbar puncture showed normal CSF (glucose,2.71 mmol/L;protein,0.2 g/L;cytology,3 /mm3).CSF bacterial culture was negative.Central nervous system demyelinating disease serology tests,including anti-aquaporin 4 antibodies,NMO-IgG,anti-MOG-IgG,and anti-MBP-IgG,were negative.His CSF IgG test was positive and oligoclonal bands were present,suggesting intrathecal antibody production.Serum IgG test was negative.Anti-NMDAR CSF test was positive,but serum testing was negative.Other autoimmune encephalitis antibodies were negative in both CSF and serum.Repeat syphilis confirmatory and rapid tests were positive.Repeat lumbar puncture after 1 mo of treatment with immunoglobulin and methylprednisolone therapy showed CSF that was almost acellular (6/mm3) with normal protein (0.43 g/L) and glucose (2.82 mmol/L).CSF bacterial culture was normal.CSF IgG index was elevated (50.6 mg/L).Paraneoplastic tests including Hu,Yo,Ri,CV2,Ma2,Amphiphysin,ANNA-3,Tr,PCA-2,and GAD were negative,except for anti-NMDAR antibody positivity (+1:1) in CSF and negativity in serum.Repeat serum syphilis rapid plasma responsive ring card test was positive and treponemal antibody was elevated (33.4).
FINAL DIAGNOSIS
Based on the detection of anti-NMDAR antibodies in the CSF,we finally diagnosed the patient with anti-NMDAR encephalitis.
TREATMENT
Based on the detection of NMDAR antibody in CSF,combined with the clinical and imaging features of the patient,we considered that the patient may have anti-NMDAR encephalitis.According to the patient’s weight,we treated him with intravenous methylprednisolone 1 g QD and immunoglobulin 25 g QD for 5 d,and his symptoms improved.Five days after immunoglobulin and methylprednisolone therapy,his unsteady gait and cognitive impairment were greatly improved.Diplopia completely resolved,and head and neck tremors improved.After discharge from the hospital,he continued treatment with prednisone 60 mg once per day.
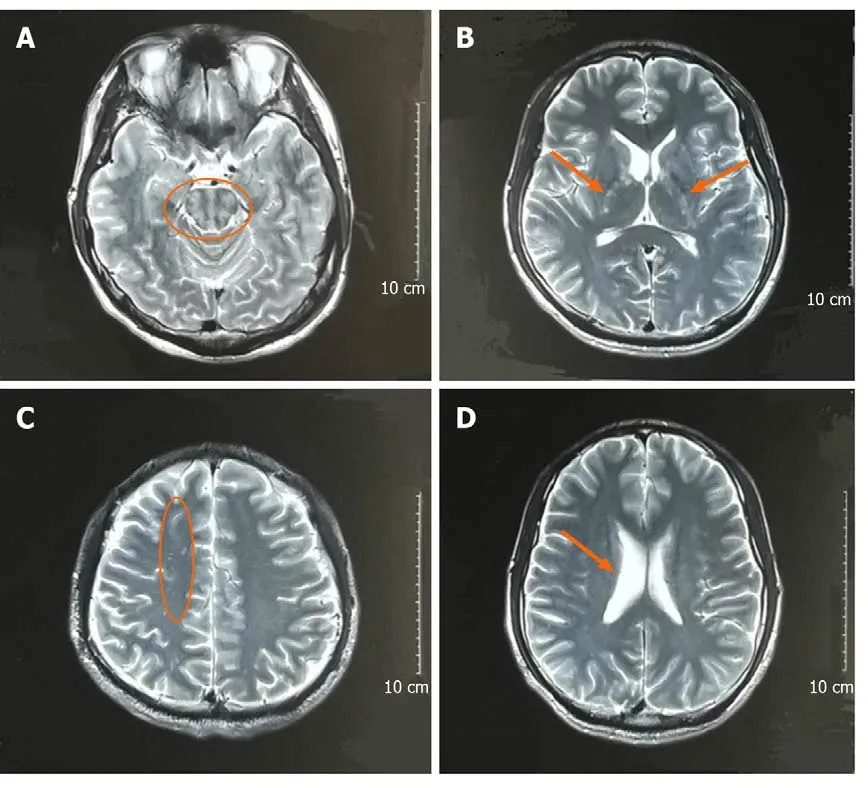
Figure1 Brain magnetic resonance imaging scans 1 mo before admission.A:T2 weighted image shows high signal of the brain stem (orange circle);B:T2 weighted image shows high signal of bilateral internal capsules (orange arrows);C:T2 weighted image shows high signal of the right of frontal lobe (orange circle);D:T2 weighted image shows that the right ventricle is enlarged (orange arrow).
OUTCOME AND FOLLOW-UP
After discharge,the patient continued to take prednisone orally.Prednisone was gradually reduced and his condition remained stable without further aggravation.On follow-up assessment 6 mo later,his gait instability had improved significantly;diplopia was still present,and tremor was alleviated.
文献报道,其发病率在千分之以左右。男孩略多于女孩。可以单足或双足同时发生。由于一出生就会被发现,因此疏忽的病例较少见,多能及早治疗,效果也较好,但畸形也易复发,应定期随访至骨骼成熟(约14岁以后)。
DISCUSSION
The diagnostic criteria[4]for and treatment[5]of anti-NMDAR have been reported[6].We report a case of anti-NMDAR encephalitis combined with syphilis,which has rarely been reported.Anti-NMDAR encephalitis is autoimmune encephalitis mediated by the NMDA receptor[7].NMDAR is an important excitatory amino acid in the central nervous system,which regulates neuronal survival and participates in synaptic signaling and plasticity formation.Excessive activation of the NMDAR can lead to excitotoxicity,which may be the underlying pathogenesis of epilepsy,dementia,and stroke[8];conversely,schizophrenia-like symptoms may occur[9].At present,the etiology of anti-NMDAR encephalitis is unclear,but it has been reported that IgG antibody can be found in patients with herpes simplex encephalitis[10].Autoimmune encephalitis should be investigated in cases of atypical herpes simplex encephalitis or other types of viral encephalitis[10].
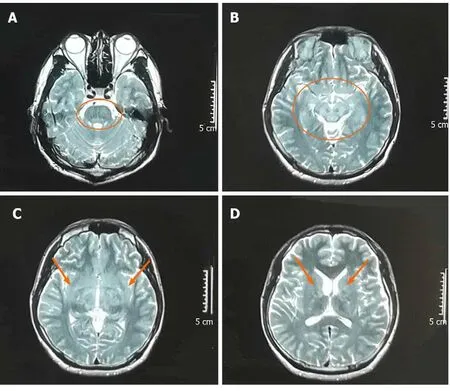
Figure2 Brain magnetic resonance imaging scans on admission.A:T2 weighted image shows high signal of the pons (orange circle);B:T2 weighted image shows high signal of the mesencephalon and bilateral medial temporal lobes (orange circle);C:T2 weighted image shows high signal of bilateral basal ganglia (orange arrows);D:T2 weighted image shows high signal of bilateral basal ganglia (orange arrows).
There are many clinical features of anti-NMDAR encephalitis,but each patient has different symptoms.Our patient’s findings were primarily characterized by cognitive impairment,unsteady gait,diplopia,and tremors.It has been reported that in the course of the disease,adults show more frequent memory impairment and inadequate ventilation than children,and less focal defects (paraplegia and ataxia) and speech or motor disorders[11].Some patients show symptoms of microcephaly ataxia[12].In a single-center,longitudinal study in China,the most common clinical manifestations of anti-NMDAR encephalitis were psychosis (82.7%) and epilepsy (80.9%)[13].Anti-NMDAR encephalitis can show early symptoms of psychosis[14]and be easily misdiagnosed as mental illness[15].Our patient was initially diagnosed with depression,but there was no improvement in his condition.Therefore,when we evaluate patients with mental disorders,we should recognize the possibility of underlying diagnoses producing psychiatric symptoms.Anti-NMDAR encephalitis showing psychiatric symptoms has been specifically reported[16].In China,the patients often suffer from mental illness and epilepsy,but the proportion of potential tumors is very low[13].Our patient showed no abnormality in the whole tumor and chest and abdomen computed tomography,but the patient was requested to undergo additional examination for potential tumors in the future.Tumors are recognized to be associated with anti-NMDAR encephalitis[14,17,18].
Although he was diagnosed with syphilis,the symptoms did not improve after treatment with anti-syphilis medication,indicating that these lesions may not be directly related to syphilis.Despite this,we suspected that this autoimmune encephalitis may be due to irreversible damage to the nervous immune system caused by syphilis;thus it is likely that syphilis and autoimmune encephalitis coexist.Recently,cases of anti-NMDAR encephalitis and neurosyphilis have been published.It is reported that anti-NMDAR encephalitis may be related to neurosyphilis[19].Although cases of anti-NMDAR encephalitis coexistent with syphilis are rare,we cannot ignore the potential link.
Head MRI in patients with anti-NMDAR encephalitis is not necessarily abnormal,and its imaging findings are not specific.Anti-NMDAR encephalitis is related to extensive superficial white matter damage in patients with incomplete recovery[20].Data from the largest cohort of patients with anti-NMDAR encephalitis included extensive multimodal MRI findings,which suggest that hippocampal structural damage and related memory loss are important long-term sequelae of encephalitis[21].Our patients’ brain MRI showed abnormal symmetrical signals in the pons,mesencephalon,bilateral medial temporal lobe,and bilateral basal ganglia.Recently,it has been reported that the head MRI in a patient with anti-NMDAR encephalitis showed extensive lesions in the frontal lobe,temporal lobe,and basal ganglia,with mild mass effect[22].
At present,there are not many methods to treat anti-NMDAR encephalitis,and the curative effect of available treatments is uncertain.Some literature outlined the best treatment for anti-NMDAR encephalitis,including the combination of tumor resection,immunotherapy,intensive care,and rehabilitation including physical therapy[23].It has been reported that alemtuzumab and methotrexate are used to maintain immunosuppression across the blood-brain barrier,according to the pathogenesis[24,25]of anti-NMDAR,and these treatments have achieved considerable positive effect[26].After immunoglobulin and hormone therapy,the symptoms of our patient were temporarily relieved during hospitalization,and at the 6-mo follow-up,his walking instability had improved significantly and his tremor was alleviated;his diplopia continued.It has been reported that the disease is characterized by recurrence and incurability[27,28].We asked the patient to come to the hospital for reexamination every 3-6 mo.Data in the literature showed that immunoglobulin and hormone therapy are effective in the treatment of anti-NMDAR encephaliti[19,29].It has been reported that the dysfunction of postsynaptic glutamate transmission at the synapse leads to increased release of γ-aminobutyric acid and decreased secretion of glutamate in anti-NMDAR encephalitis,so glutamate therapy can be used in anti-NMDAR encephalitis[30].In the future,we can try the glutamate therapy in more patients with anti-NMDAR encephalitis to observe the clinical effect.
CONCLUSION
At present,there are few reported cases of anti-NMDAR encephalitis coexistent with syphilis,and the correlation between the two diseases is unclear.When we understand the characteristics of anti-NMDAR encephalitis combined with syphilis,we can recognize,diagnose,and treat these patients earlier.Additionally,the unique imaging manifestations of anti-NMDAR encephalitis and the clinical manifestations caused by injury of certain parts of the brain,such as the pons,midbrain,and basal ganglia,cannot be ignored.
ACKNOWLEDGEMENTS
We are very grateful to the patient and his family.
猜你喜欢
品牌研究(2022年21期)2022-07-28
品牌研究(2022年20期)2022-07-21
世界博览(2021年7期)2021-04-19
房地产导刊(2020年10期)2020-11-16
故事作文·低年级(2017年3期)2017-04-04
为了孩子(孕0~3岁)(2017年1期)2017-01-13
幸福·悦读(2016年11期)2016-12-21
智能计算机与应用(2016年5期)2016-11-19
小学生时代·综合版(2014年11期)2015-01-17
小学生时代·大嘴英语(2012年5期)2012-05-23
 World Journal of Clinical Cases2020年12期
World Journal of Clinical Cases2020年12期
- World Journal of Clinical Cases的其它文章
- Assessment of diaphragmatic function by ultrasonography:Current approach and perspectives
- Computer navigation-assisted minimally invasive percutaneous screw placement for pelvic fractures
- Research on diagnosis-related group grouping of inpatient medical expenditure in colorectal cancer patients based on a decision tree model
- Evaluation of internal and shell stiffness in the differential diagnosis of breast non-mass lesions by shear wave elastography
- Real-time three-dimensional echocardiography predicts cardiotoxicity induced by postoperative chemotherapy in breast cancer patients
- Lenvatinib for large hepatocellular carcinomas with portal trunk invasion:Two case reports