
Complete response in anaplastic lymphoma kinase–rearranged oncocytic thyroid cancer:A case report and review of literature
2020-09-14 05:20:04
Victoire de Salins,Charlotte Joly,Hélène Boussion,Christophe Tournigand,Emmanuelle Kempf,Department of Medical Oncology,Henri Mondor et Albert Chenevier Teaching Hospital,Assistance Publique – Hôpitaux de Paris,University of Paris-Est Creteil,Créteil 94010,France
Gokoulakrichenane Loganadane,Yazid Belkacemi,Department of Radiation Oncology and Breast Center,Henri Mondor University Hospital,Assistance Publique – Hôpitaux de Paris,University of Paris-Est Creteil and IMRB-INSERM 955 Team 21,Creteil 94010,France
Mukedaisi Abulizi,Department of Nuclear Medicine,Henri Mondor et Albert Chenevier Teaching Hospital,Assistance Publique – Hôpitaux de Paris,University of Paris-Est Creteil,Créteil 94010,France
Maya Nourieh,Department of Pathology,Henri Mondor et Albert Chenevier Teaching Hospital,Assistance Publique – Hôpitaux de Paris,University of Paris-Est Creteil,Créteil 94010,France
Abstract
Key words:Oncocytic tumors of the thyroid;Hürthle cell tumors;Crizotinib;Precision;Medicine;Case report
INTRODUCTION
Since 1980,the incidence of thyroid cancer has strongly increased,despite a recent decrease in the number of female cases.Each year,around 63000 new cases of thyroid cancer are diagnosed worldwide,leading to 2820 deaths.Thanks to initial diagnoses made at an earlier stage,the overall survival (OS) of patients with thyroid cancer has recently improved.The 5-year OS rate expended from 83% to 95% in the early 2000s[1].
Oncocytic tumors of the thyroid,also known as Hürthle cell tumors,are rare.The frequency of this tumor is actually unknown[2].Hürthle (oncocytic) cell tumors are neoplasms composed of oncocytic cells.Non-invasive cases are called Hürthle cell adenomas,and cases with capsular or vascular invasion are called Hürthle cell carcinomas[3].Follicular neoplasms can be composed in part by Hürthle cells and considered as Hürthle cell tumors only if more than 75% of the tumor is composed of Hürthle cells[4].Oncocytic cells are large,polygonal cells with marked eosinophilic,granular cytoplasm reflective of overly abundant mitochondria[5].Metastatic dissemination involves both blood and lymph nodes - contrasting with follicular carcinoma.Oncocytic carcinomas are characterized by a poor prognosis when compared to other differentiated thyroid carcinomas[6-8].
Papillary thyroid carcinoma cases with Hürthle cell changes are likely to have higher rates of recurrence (28%vs11%)[9].A SEER database cohort study showed that 25-year OS rates reached 82.1% and 89.1% in both populations,respectively[10].
In 1994,theanaplastic lymphoma kinase(ALK) gene was discovered through the identification of its fusion withnucleophosmin-1(NPM1) in anaplastic large cell lymphomas[11].In 2007,Hiroyuki Mano and colleagues[12]discovered a novel ALK fusion echinoderm-microtubule-associated protein-like 4 (referred to as EML4) that was found in a small percentage of Japanese lung cancers.ALK can be activated by translocation,as well as by mutation at theALKlocus,most commonly within the kinase domain,as reported in patients with thyroid cancer[13].
Crizotinib is a specific ALK inhibitor,which was initially developed in non-small cell lung cancer (NSCLC).The phase III study PROFILE 1014 compared crizotinib with chemotherapy as a first-line treatment in patients with advancedALK-positive nonsquamous NSCLC.The median progression-free survival was significantly better with crizotinib than chemotherapy [10.9 movs7.0 mo,respectively,with hazard ratio of 0.45 and 95% confidence interval (CI) of 0.35,0.60].The objective response rates reached 74% and 45%,respectively.As compared with chemotherapy,crizotinib was associated with a greater reduction in lung cancer-related symptoms and a greater improvement in quality of life[14,15].
Other solid tumors harboring a translocation inALKhave been described,such as renal carcinoma,thyroid,colorectal,ovarian cancers,and spitzoid melanomas[16].The identification ofALKrearrangements in thyroid tumors is highly promising.It has been reported that administration of crizotinib led to tumor stability in 1 case of advanced aggressive papillary cancer and to a response rate of 90% in 1 case of anaplastic thyroid cancer;both tumor responses lasted more than 6 mo[17,18].We will present herein the case of a complete tumor response in 1 case of metastatic oncocytic thyroid cancer.Informed written consent was obtained from the patient for publication of this report and any accompanying images.
CASE PRESENTATION
Chief complaints
A 76-year-old woman,former personal assistant,was hospitalized because of an impaired general condition.
History of present illness
The patient suffered from an impaired general condition,associated with a body weight loss of 15 kg over 7 mo.
History of past illness
In 2008,the patient had received a diagnosis of multinodular goiter.She currently suffered from type 2 diabetes,hypertension,and dyslipidemia,and had undergone an appendectomy in 1960.Her daily drug medicine routine was 500 mg metformin three times a day,120 mg gliclazide,100 mg sitagliptin,50 mg fosinopril,12.5 mg hydrochlorothiazide,300 mg piascledine in the morning,and 20 mg lercanidipine,10 mg simvastatin and 2.5 mg bisoprolol at night.
Personal and family history
The patient had no medical history other than arterial hypertension.Her family reported no other cases of cancer.
Physical examination upon admission
Physical examination found an altered patient with a moderate goiter without clinical signs of compression,and a suspect left sub-clavicular adenopathy.The remainder of the medical examination,including palpation of the breast,showed no anomalies.
Imaging examinations
A chest-abdomen-pelvis computed tomography (CT) revealed a multinodular thyroid associated with multiple mediastinal lymphadenopathies,lytic bone lesions and bilateral mammary lumps.The positron emission tomography (PET) scan found no FDG uptake in the thyroid while hypermetabolic activity was observed in the left inferior jugular and the supra-clavicular lymphadenopathies.Several bilateral mediastinal hypermetabolic lymphadenopathies and a right upper outer mammary lesion were also hypermetabolic.
Laboratory examinations
The blood tests showed normal thyroid function and inflammatory anemia.Fine needle aspiration of the right thyroid nodule was contributive and revealed a category V lesion according to The Bethesda System for Reporting Thyroid Cytopathology(suspicious for malignancy),isolated cells,a cluster of large cells with oncocytic features,and scanty colloid.Metastasis from a distant organ malignancy could not be ruled out solely based on this exam.The supra-clavicular biopsy revealed a metastasis from carcinoma with an oncocytic feature,as well as cytokeratin 7 andTTF1expression in immunohistochemistry.We found moderate cytoplasmic staining (2+) of ALK protein (clone 5A4).A bronchoscopy with a bronchial biopsy showed carcinoma cells that expressedTTF1within lymphatic vessels.Similar type of cells were observed in bronchoalveolar lavage.The 9 mm and 5 mm right mammary nodules were classified as ACR4 and the biopsies showed an infiltrating carcinoma with oncocytic features,without vascular and perineural invasion.Complementary immunohistochemical assessments showed that tumor cells in the breast biopsy also presented nuclear staining for TTF1 and no staining for estrogen receptor,androgen receptor,GATA3 or HER2.Interestingly,strong cytoplasmic staining (3+) of ALK protein (clone D5F3) was observed (Figure 1).Fluorescencein situhybridization analysis revealed a rearrangement ofALKin 61% of the cells.We found no mutations in theEGFR,BRAF,RAS,ERBB2,andPIK3CAgenes within the lymph node metastasis.
FINAL DIAGNOSIS
Based on the molecular and anatomical features found,we made a diagnosis of oncocytic carcinoma of the thyroid with nodes,breast and bone metastasis,with a rearrangement ofALK.
TREATMENT
A multidisciplinary tumor board discussion,based on molecular characteristics of the tumor,suggested initiating a daily treatment of crizotinib (500 mg per day,taken as 250 mg in the morning and the night).The treatment was well tolerated,and the physical condition improved.No vision disorder,nausea,diarrhea,pneumonitis,hepatotoxicity or skin toxicity was reported.The patient complained of grade 2 constipation.No dose reduction or interruption was required.
OUTCOME AND FOLLOW-UP
The PET scan performed 4 mo after the initiation of crizotinib showed a complete metabolic response with no thyroid,pulmonary,nodal or visceral hypermetabolic spot but with multiple condensing bone metastases on most of the skeleton without significant hypermetabolism (scar lesions) (Figure 2).The patient presented a complete response according to RECIST criteria.
Two months later,the patient experienced a loss of balance that caused multiple falling episodes and a frontal syndrome with logorrhea and disinhibition.The cerebral scan revealed multiple supra and infra tentorial nodules suggestive of brain metastases for which whole brain radiotherapy (WBRT) has been indicated.Crizotinib was stopped during WBRT delivering 30 Gy in 10 fractions that resulted in a stability of the cerebral lesions.However,the patient’s condition stayed fragile with remaining walking and behavioral disorders,which prevented us from starting a new line of anticancer treatment.The patient died after 3 mo of palliative care.
DISCUSSION
To the best of our knowledge,we report herein the first complete metabolic response in an ALK-rearranged oncocytic tumor of the thyroid (Figure 3).
This new approach is interesting,as the current recommended treatment for disseminated oncocytic tumors is radioiodine,which is associated with a lower response rate than other thyroid carcinomas[19,20].Oncocytic carcinoma is a rare type of cancer with a higher postoperative recurrence rate (28%vs11%,P<0.0001) and a poorer cause-specific mortality rate than papillary thyroid carcinoma (1.7%vs4%,P<0.0005)[16,19].The cumulative rate of recurrence or death within 5 years after initial diagnosis of a stage III–IV disease reaches 74% in women and 91% in men,respectively[21].
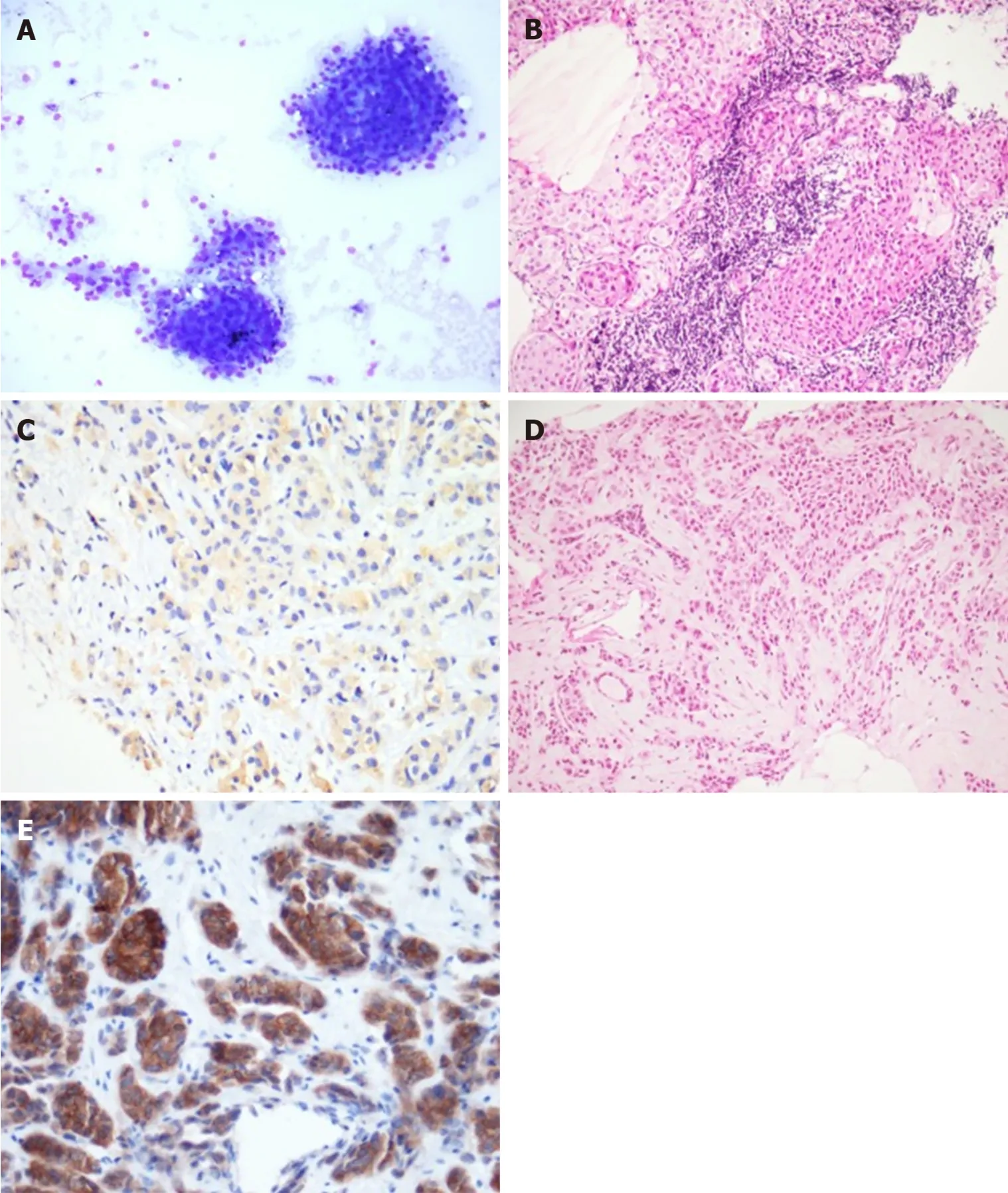
Figure1 Pathological findings of biopsies and ALK positive pictures.
Recently,understanding of the molecular pathogenesis of thyroid cancer leads to increased interest in tyrosine kinase-targeted therapy.Mutations in several oncogenes and tumor suppressor genes have been described,including theBRAF,RAS,PIK3CA,andAPCgenes[22,23].In 2014,a patient diagnosed with anaplastic thyroid cancer showing anALKrearrangement experienced an excellent response rate to crizotinib,reaching up to a 90% reduction in tumor size across all pulmonary lesions[18].Oncocytic tumors with anALKrearrangement have not been described extensively in the literature.Our rationale for using crizotinib in this situation was based on the following arguments.
First,disseminated oncocytic thyroid cancers are known to have poor prognoses and are likely less avid to radioactive iodine compared to papillary thyroid cancer[10,20].The SEER study from 1988 to 2009 identified 3311 patients with oncocytic tumors who were less likely to undergo total thyroidectomy than patients with other thyroid carcinomas (P= 0.028).Absence of surgery and an existence of metastatic disease were factors independently associated with a worse prognosis in this population (hazard ratio of >3.0,95%CI of 1.89-6.38)[10].A study published in 2003 showed that radioactive iodine therapy may confer a survival benefit when it is used for adjuvant ablation therapy but not when residual or metastatic disease is present.Survival benefits for the use of extensive surgery,external beam radiation therapy,or chemotherapy by doxorubicin,cisplatin or the two drugs together could not be demonstrated[24].
Second,we followed the “AcSé crizotinib” phase II study,promoted by the French National Cancer Institute,which encouraged secure access to innovative treatments for 235 patients with malignant disease harboring a molecular target such asALK,METorROS1[25].
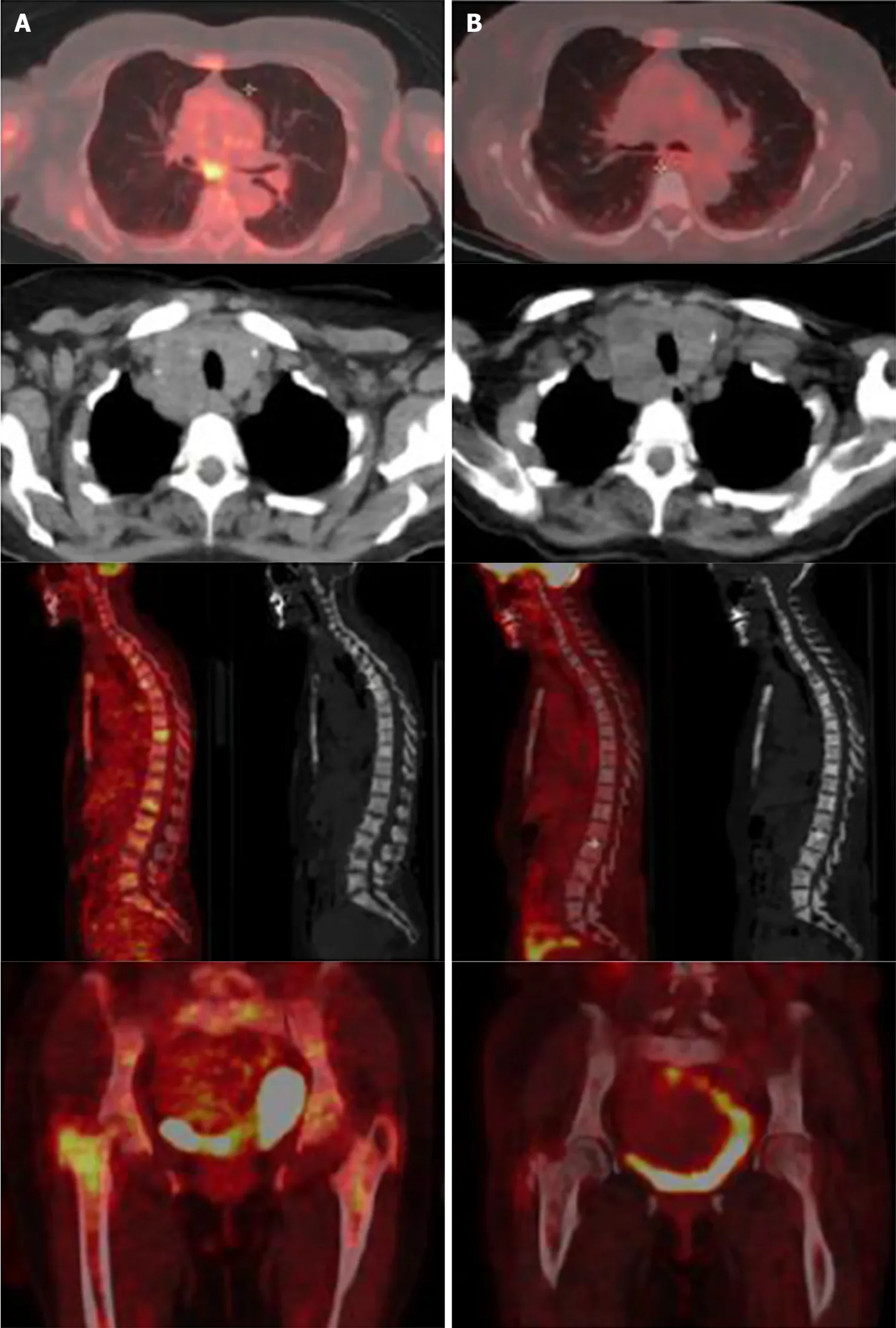
Figure2 Comparison between baseline positron emission tomography scans (A,left) and after 4 mo of crizotinib treatment (B,right).
Third,crizotinib is a specific ALK inhibitor recommended at that time as a first-line treatment in NSCLC withALKrearrangement[14].Finally,this targeted therapy showed unexpected responses in 2 cases of aggressive papillary and anaplastic thyroid cancers,respectively[17,18].
Despite this encouraging response,this case report presents some limitations.On this unique case,there is a lack of evidence to generalize and no possibility to establish cause-effect relationship.
Biology-driven decisions should be enhanced,especially for patients suffering from rare tumors with bad clinical prognosis who could benefit from the screening of oncogenic molecular targets.Further studies are warranted to confirm our findings,with comparison with standard of care treatment.
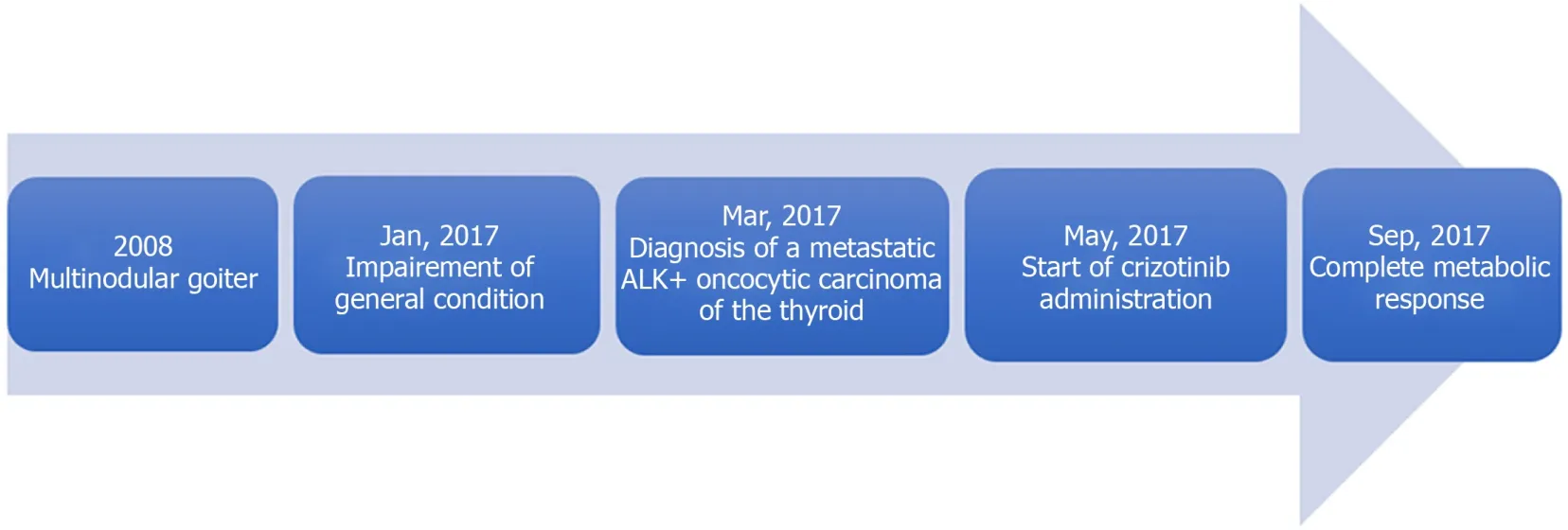
Figure3 Timeline of the case history,treatment,and clinical outcome.
In this case report,the patient developed secondary cerebral lesions after 7 mo under crizotinib.A study showed that crizotinib was associated with systemic and intracranial disease control in patients withALK-rearranged NSCLC who were ALK inhibitor-naïve and had asymptomatic brain metastases (systemic disease control:63%,95%CI:54%,72%,intracranial disease control;56%,95%CI:46%,66% at 12 wk).However,progression of pre-existing or development of new intracranial lesions while receiving therapy was a common manifestation of acquired resistance to crizotinib.Twenty percent of the patients without baseline brain metastases and whose tumor progressed under crizotinib were finally diagnosed with brain metastases[26,27].A new approach could be undertaken with alectinib,which recently showed better intracranial responsiveness[28],superior efficacy and lower toxicity[29,30]compared to crizotinib (central nervous system response rate for alectinib of 81% with 95%CI:58-95 and for crizotinib of 50% with 95%CI:28-72) in primary treatment of ALK-positive NSCLCs.
CONCLUSION
This case reports unexpected and dramatic efficacy of crizotinib in a thyroid tumor with anALKrearrangement.A comparison of crizotinib with standard radio iodine as a first therapeutic option in this indication still needs to be assessed.More studies are required to confirm clinical treatments for this rare and aggressive disease.
ACKNOWLEDGEMENTS
We thank Mrs.Fabienne Vaillant for her help in editing the manuscript.
 World Journal of Clinical Oncology2020年7期
World Journal of Clinical Oncology2020年7期
- World Journal of Clinical Oncology的其它文章
- Mechanisms and anatomical risk factors of pneumothorax after Bevacizumab use:A case report
- Is there a role for treatment-oriented surgery in liver metastases from gastric cancer?
- Why natural killer cells in triple negative breast cancer?
- Circulating cell-free nucleic acids as prognostic and therapy predictive tools for metastatic castrate-resistant prostate cancer
- MUTYH:Not just polyposis
- Role of imaging biomarkers in mutation-driven non-small cell lung cancer