
子宫内膜样子宫内膜癌中错配修复基因表达与临床病理及相关基因表达的关系
2020-08-10 09:09王露陈思敏赵苏苏章宜芬
医学信息 2020年14期
王露 陈思敏 赵苏苏 章宜芬

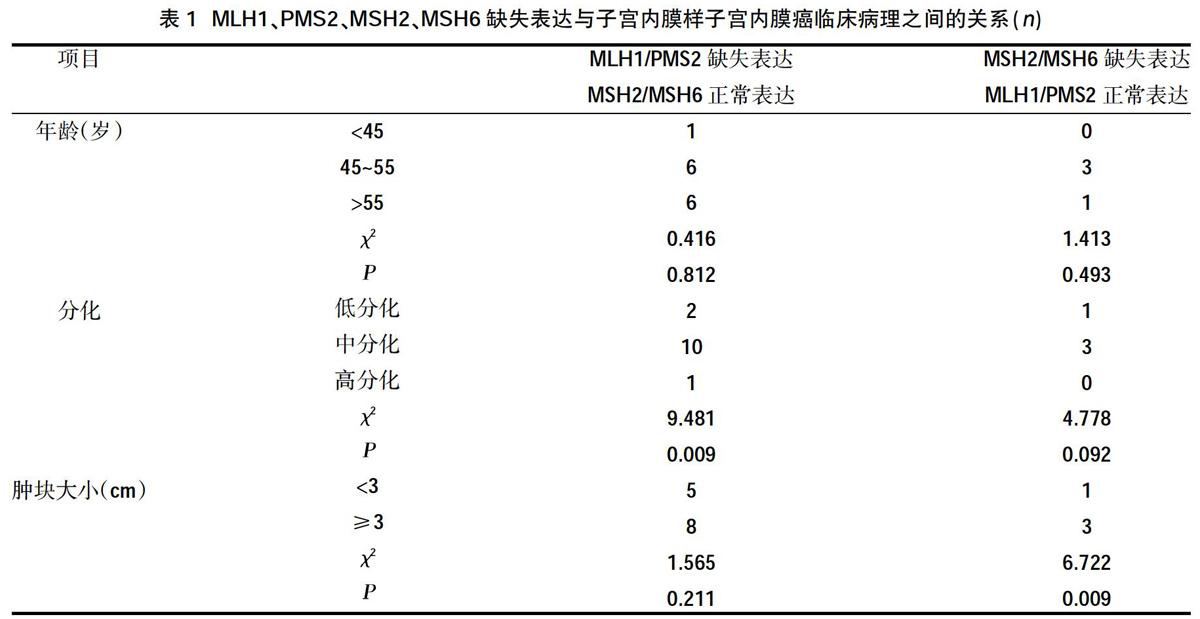
摘要:目的 分析錯配修复(MMR)基因(MLH1、PMS2、MSH2、MSH6)的表达与子宫内膜样子宫内膜癌临床病理及ER、PR、p53、Ki-67、p16蛋白免疫组化表达的关系,探讨MMR基因及其他基因对子宫内膜样子宫内膜癌发生发展的作用。方法 收集2016年8月~2019年10月我院诊治的53例子宫内膜样腺癌患者的临床病理资料,应用免疫组织化学法检测癌组织中MLH1、PMS2、MSH2、MSH6、ER、PR、Ki-67、p16、p53的表达水平,分析癌组织中MLH1、PMS2、MSH2、MSH6的表达及其与临床病理、ER、PR、p53、Ki-67、p16表达的关系。结果 ①53例癌组织样本中MLH1、PMS2、MSH2、MSH6发生缺失表达的模式中,MLH1/PMS2缺失、MSH2/MSH6正常表达者最常见,其次是MSH2/MSH6缺失、MLH1/PMS2正常表达者, MLH1/PMS2/ MSH2/MSH6四个基因全部缺失表达仅1例;②MLH1/PMS2缺失、MSH2/MSH6正常表达者癌组织呈中分化者较多,而MMR基因全部正常表达者癌组织呈低分化者较多,差异有统计学意义(P<0.05);MSH2/MSH6缺失、MLH1/PMS2正常表达者肿块相对较大,p16表达呈阳性者相对较多,差异有统计学意义(P<0.05);MLH1/PMS2/ MSH2/MSH6四个基因全部缺失表达者的癌组织为低分化,ER、PR均阴性表达。结论 发生MMR蛋白缺失的子宫内膜样子宫内膜癌癌组织中,MLH1/PMS2缺失表达及MSH2/MSH6正常表达者最常见,MLH1/PMS2缺失表达及MSH2/MSH6正常表达的患者癌组织多为中分化,MSH2/MSH6缺失、MLH1/PMS2正常表达的患者肿块相对较大,p16表达呈阳性者较多。
关键词:子宫内膜样子宫内膜癌;错配修复基因;ER;PR;Ki-67;p16;p53
中图分类号:R737.33 文献标识码:A DOI:10.3969/j.issn.1006-1959.2020.14.019
文章编号:1006-1959(2020)14-0061-06
Relationship Between Mismatch Repair Gene Expression and Clinicopathology
and Related Gene Expression in Endometrioid Endometrial Carcinoma
WANG Lu,CHEN Si-min,ZHAO Su-su,ZHANG Yi-fen
(Department of Pathology,Jiangsu Provincial Traditional Chinese Medicine Hospital,Nanjing 210000,Jiangsu,China)
Abstract:Objective To analyze the relationship between the expression of mismatch repair (MMR) genes (MLH1, PMS2, MSH2, MSH6) and clinicopathology of endometrioid endometrial cancer and immunohistochemical expression of ER, PR, p53, Ki-67, p16 proteins to explore the role of MMR genes and other genes in the development of endometrioid endometrial cancer.Methods The clinical and pathological data of 53 patients with endometrioid adenocarcinoma diagnosed and treated in our hospital from August 2016 to October 2019 were collected. Immunohistochemistry was used to detect MLH1, PMS2, MSH2, MSH6, ER, PR, Ki-67, p16, p53 expression levels, analysis of MLH1, PMS2, MSH2, MSH6 expression in cancer tissues and its relationship with clinicopathology, ER, PR, p53, Ki-67, p16 expression.Results ①Among the 53 cancer tissue samples, MLH1, PMS2, MSH2, and MSH6 were found to be expressed in the missing pattern. MLH1/PMS2 deletion and MSH2/MSH6 normal expression were the most common, followed by MSH2/MSH6 deletion, MLH1/PMS2 normal expression,only one case of MLH1/PMS2/MSH2/MSH6 all four genes were deleted and expressed;②MLH1/PMS2 deletion, MSH2/MSH6 normal expression cancer tissues were more differentiated, and all MMR gene normal expression cancer tissues were poorly differentiated, the difference was statistically significant (P<0.05); MSH2/MSH6 those with deletion and normal expression of MLH1/PMS2 are relatively large, and those with positive expression of p16 are relatively large, the difference was statistically significant (P<0.05); cancer tissues of those with all four genes lacking expression of MLH1/PMS2/MSH2/MSH6 For poor differentiation, ER and PR are negatively expressed.Conclusion Among endometrioid endometrial carcinoma tissues with MMR protein deletion, MLH1/PMS2 deletion expression and MSH2/MSH6 normal expression are the most common. Patients with MLH1/PMS2 deletion expression and MSH2/MSH6 normal expression are mostly in patients with moderate differentiation, MSH2/MSH6 deletion, and normal expression of MLH1/PMS2, the tumor mass is relatively large, and p16 expression is positive.
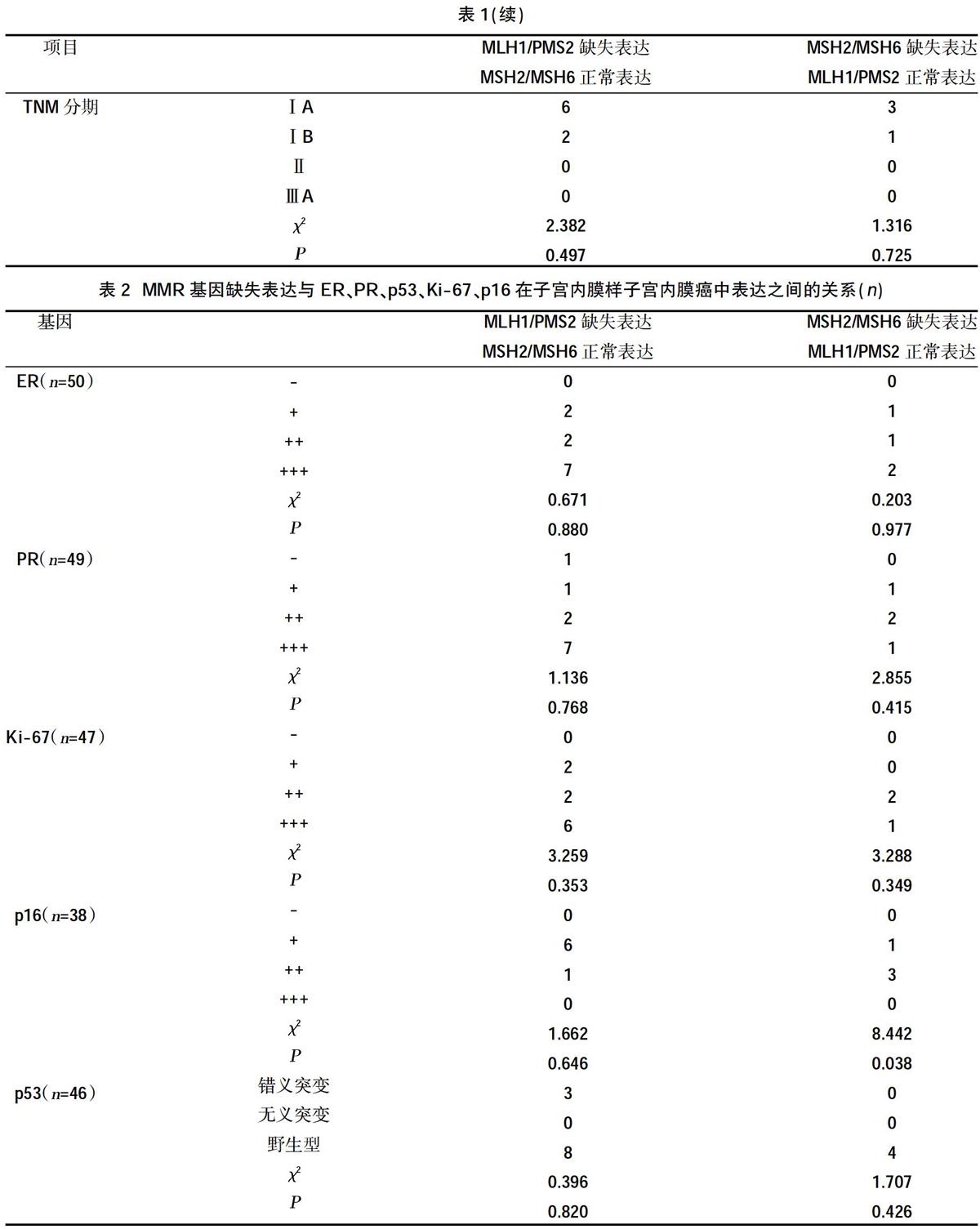
抑癌基因P53有调节转录、抑制细胞生长、诱导调亡的作用,是目前与人类肿瘤研究相关性最高的基因之一,通过多途径参与EC的发生发展。P53可调节细胞生长,使出现DNA损伤的细胞生长停滞于G1期,从而有利细胞启动自身修复机制。本研究中,p53错义突变表达11例,占23.91%,无义突变表达1例,占2.17%,野生型表达34例占73.91%。而在MMR基因缺失表达的标本中,p53错义突变表达占16.67%,野生型占77.78%,提示在子宫内膜样子宫内膜癌中MMR蛋白与P53蛋白可能没有相关性。
抑癌基因p16在许多肿瘤中均有高频率纯合子缺失[5,17],p16故又称为多肿瘤抑制基因(MTSI)。p16基因作用于CDK4、cyclin D1 、Rb 的通路,从而调节Rb蛋白阻止细胞超常增殖。当p16基因发生突变或缺失时可使细胞发生分裂增殖,继发肿瘤形成发展。p16缺失可为肿瘤浸润、转移提供生长优势[18]。本研究中,p16 表达为(-)者3例,占7.89%、(1+)者25例,占65.79%、(2+)者8例,占21.05%、(3+)者2例,占5.26%;在MMR基因缺失表达的标本中,p16 表达为(-)者未见、(1+)者7例,占63.63%、(2+)者4例,占36.36%、(3+)者未见,其中MSH2/MSH6缺失、MLH1/PMS2正常表达者p16表达阳性者(2+)相对较多;根据这一结果,可以推测其发生有两种可能,一种是MSH2/MSH6缺失、MLH1/PMS2正常表达者可能会存在p16代偿性表达的修复从而抑制MMR蛋白导致的细胞异常增殖;另一种是MSH2/MSH6缺失、MLH1/PMS2正常表达者通常p16不会发生缺失。
Ki-67与细胞增殖密切相关,是一种约395 kD 的核抗原[19],是研究细胞增殖活性的最常用的重要指标。除G0期和 G1早期之外的其他各期都有Ki-67的表达,M 期可达高峰。肿瘤组织中Ki-67抗原表达可反映其增殖活性,与肿瘤发展、转移和预后相关[20,21],Ki-67的表达能较好的成为肿瘤发生发展的早期提示指标。本研究发现,最常见的两种MMR蛋白缺失表达模式与Ki-67的表达无统计学意义,提示癌细胞增殖活性强弱与错配修复基因表达是否正常的关系并不是很大,这些增殖活性相对较高的组织并没有错配修复基因的缺失,说明其活性高可能是由于其他基因的改变导致。而其中1例4种MMR蛋白均缺失表达病例的其Ki-67呈强阳性表达,显示出很强的增殖活性,通常差分化的肿瘤增殖活性比较高,而该例患者的分化很差,Ki-67也是表现为强阳性。
综上所述,本研究发现发生MMR蛋白缺失的子宫内膜样子宫内膜癌癌组织中,MLH1/PMS2缺失表达及MSH2/MSH6正常表达者最常见。MLH1/PMS2缺失表达及MSH2/MSH6正常表达这一模式的病例的癌组织多为中分化;MSH2/MSH6缺失、MLH1/PMS2正常表达者肿块相对较大以及p16表达呈明显阳性者相对较多;提示癌组织为中等分化的病例发生MLH1/PMS2缺失表达及MSH2/MSH6正常表达的几率较大,肿块越大以及p16呈明显表达者发生MSH2/MSH6缺失、MLH1/PMS2正常表达的机率越大。4个MMR基因同时缺失表达的癌组织为低分化、ER及PR均阴性表达;可能提示子宫内膜样子宫内膜癌分化程度越低及癌组织ER、PR 阴性表达时,4种MMR基因同时缺失表达发生机率越高,需要进一步扩大样本进行验证。
参考文献:
[1]Parkin DM,Bray MF,Ferlay MJ,et al.Global cancer statistics,2002[J].Ca A Cancer Journal for Clinicians,2005,55(2):74.
[2]Le S,Ansari U,Mumtaz A,et al.Lynch Syndrome and Muir-Torre Syndrome:An update and review on the genetics,epidemiology,and management of two related disorders[J].Dermatology Online Journal,2017,23(11) :13030.
[3]Sorbe B.Prognostic importance of DNA ploidy in non-endometrioid,high-risk endometrial carcinomas[J].Oncology Letters,2016,11(3):2283-2289.
[4]Bartley AN,Hamilton SR,Alsabeh R,et al.Template for Reporting Results of Biomarker Testing of Specimens From Patients With Carcinoma of the Colon and Rectum[J].Archives of pathology&laboratory medicine,2013,138(2):166-170.
[5]鄭清存,陈瑞英,杨超.绝经前乳腺癌ER、PR、c-erbB-2的表达与血清E2水平及临床病理相关性分析[J].中国误诊学杂志,2010,10(21):5047-5049.
[6]Gao Y,Li L,Song L.Expression of p16 and Survivin in gliomas and their correlation with cell proliferation[J].Oncology Letters,2015,10(1):301-306.
[7]卢朝辉,陈杰.WHO女性生殖器官肿瘤学分类(第4版)解读[J].中华病理学杂志,2014,43(10):649-650.
[8]徐少婷,郑艳,滕晓东,等.p16INK4、p21ras及p185C-erbB-2蛋白在子宫内膜癌的表达及临床病理意义[J].实用妇产科杂志,2005,21(4):220-222.
[9]Swisher,Elizabeth,Garcia,et al.Evaluation of a Universal Mismatch Repair Protein Immunohistochemistry Screening Strategy in Women with Endometrial Carcinoma 60 Years of Age or Younger[J].Laboratory Investigation,2017.
[10]曾桢,董颖,张岩,等.子宫内膜癌中错配修复(MMR)蛋白表达缺失筛查Lynch综合征及其临床病理特点[J].现代妇产科进,2017,26(4):241-245.
[11]吴颖虹,王仁杰,贾志红,等.Lynch综合征相关遗传基因及病理诊断对临床的指导价值[J].中国当代医药,2019,26(1):8-10.
[12]毕蕊,涂小予,肖遥星,等.子宫内膜癌错配修复蛋白表达的临床病理分析[J].中华病理学杂志,2016,45(5):302-307.
[13]Westenend PJ,Dinjens WN.Somatic polymerase epsilon mutations as another route leading to loss of DNA MMR protein expression in endometrial carcinoma[J].Human Pathology,2018:S0046817718301114.
[14]Wei C,Wendy LF.A practical guide to biomarkers for the evaluation of colorectal cancer[J].Mod Pathol,2019,32(Suppl 1):1-15.
[15]Sylwia Mtapińska-Szumczyk,Supernat AM,Majewska HI,et al.Immunohistochemical characterisation of molecular subtypes in endometrial cancer[J].International Journal of Clinical and Experimental Medicine,2016,8(11):21981-21990.
[16]Aneta CP,Anita CG,Ewa PS,et al.Clinical importance of serum HE4 and MMP2 levels in endometrial cancer patients[J].Oncotargets&Therapy,2017(10):3169-3175.
[17]K?bel M,Ronnett BM,Singh N,et al.Interpretation of P53Immunohistochemistry in Endometrial Carcinomas:Toward IncreasedReproducibility[J].International Journal of Gynecological pathology,2019,38(1):S123-S131.
[18]陆萍,王一,张燕,等.子宫内膜癌标志物表达及其临床意义研究[J].中国实用妇科与产科杂志,2017(6):88-92.
[19]Yu CG,Jiang XY,Li B,et al.Expression of ER,PR,C-erbB-2 and Ki-67 in Endometrial Carcinoma and their Relationships with the Clinicopathological Features[J].Asian Pacific Journal of Cancer Prevention,2015,16(15):6789-6794.
[20]宁海丹,杜杨君,梁科庆,等.Maspin和Ki67在子宮内膜癌中的表达及其相关性分析[J].现代肿瘤医学,2017(20):87-90.
[21]Hong F,Sun J,Li C,et al.Expressions of Maspin and Ki67 in extranodal nasal type NK/T-cell lymphoma and the significance[J].Journal of Clinical Otorhinolaryngology,head,and neck Surgery,2015,29(13):1184.
收稿日期:2020-04-14;修回日期:2020-05-03
编辑/成森
作者简介:王露(1984.11-),女,江苏镇江人,硕士,主治医师,主要从事临床病理诊断工作
通讯作者:章宜芬(1971.10-),女,安徽安庆人,博士,主任医师,副教授,主要从事临床病理诊断工作
猜你喜欢
清华金融评论(2022年4期)2022-04-13
保健医苑(2021年7期)2021-08-13
国际放射医学核医学杂志(2021年10期)2021-02-28
中国毕业后医学教育(2020年5期)2020-12-06
房地产导刊(2020年7期)2020-08-24
中华老年多器官疾病杂志(2016年9期)2016-04-28
山东医药(2015年14期)2016-01-12
中国药理学通报(2014年2期)2014-05-09
当代畜禽养殖业(2014年10期)2014-02-27
生殖医学杂志(2013年4期)2013-03-11
