
Acupuncture for post-stroke dysphagia: An overview of systematic reviews
2020-07-31 09:25:12WeiJingFanShiBingLiangRenYanHuangGuoBinLiu
Journal of Hainan Medical College 2020年11期
Wei-Jing Fan, Shi-Bing Liang, Ren-Yan Huang, Guo-Bin Liu✉
1. Shanghai University of Traditional Chinese Medicine
2. Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine 3. Evidence-based Medicine Center of Beijing University of Chinese Medicine
Keywords:Acupuncture Post-stroke Dysphagia Overview of Systematic Reviews ROBIS AMSTER-2 GRADE
ABSTRACT Objective: To overview the systematic reviews of acupuncture for Post-stroke Dysphagia. Methods: The Chinese and English databases were searched for the systematic reviews of dysphagia after acupuncture treatment. The retrieval time was until October 30, 2019. The final literature was evaluated for bias risk, methodology quality and evidence quality by using ROBIS tool, AMSTER-2 scale and GRADE method. Results: 9 systematic reviews and 36 outcomes were included. ROBIS bias risk assessment results show that all the studies are high bias risk; AMSTER-2 methodology quality assessment results show that all the systems are of very low quality; GRADE grading shows that there are only 7 intermediate evidences in 36 clinical evidences, the rest are low-level evidences or very low-level evidences, and there are multiple intermediate evidences in the clinical efficacy of acupuncture in the treatment of dysphagia after stroke. In addition, acupuncture can significantly improve the scores of all kinds of swallowing function related scales, such as Tengdao food intake swallowing function grade, swallowing disorder specific quality of life score, standard swallowing function evaluation scale, and the incidence of adverse reactions is low. Conclusion: Acupuncture is effective in the treatment of dysphagia after stroke. It can improve the scores of various swallowing function scales and has high safety. However, the risk of systematic evaluation bias is high, the quality of methodology is low, and the level of clinical evidence is low as a whole. In the future, the relevant research design should be more rigorous, and the research report should be written in strict accordance with the PRISMA statement.
1. Introduction
Swallowing disorder is one of the common complications after stroke, and it is also the cause of serious complications such as dehydration, malnutrition, and aspiration pneumonia. Epidemiological data show that more than 70% of stroke patients will suffer from varying degrees of dysphagia. At present, the treatment of dysphagia after stroke is mainly based on basic rehabilitation training and electrical stimulation. Studies have shown that acupuncture treatment can significantly improve patients' respiratory function and promote recovery of swallowing function [1-3].
With the increasing number of clinical studies on acupuncture for post-stroke dysphagia, a number of systematic reviews have also been published to provide corresponding evidence support for clinical decision-making. However, preliminary studies have found that the results of different systematic reviews are not Exactly the same, the quality of the research is not the same, the level of clinical evidence cannot be determined, and it does not guide clinical work well. This study used a systematic review and re-evaluation to assess the methodological quality of a systematic review of acupuncture for post-stroke dysphagia, and to grade the quality of evidence for its common outcome indicators.
2. Materials and methods
2.1 Inclusion and exclusion criteria
2.1.1 Research Type
Based on a randomized controlled trial (RCT), a systematic review / meta analysis of acupuncture for post-stroke dysphagia has been published. The language is not limited and the country of publication is not limited.
2.1.2 Research objects
Patients with dysphagia after stroke have unlimited course, unlimited nationality, and unlimited gender.
2.1.3 Interventions
The experimental group was treated with acupuncture or acupuncture combined with conventional treatment, and the control group was treated with conventional treatment, blank group or placebo.
2.1.4 Outcome indicators
Main outcome measures: clinical effectiveness; Watian drinking water score; swallowing disorder-specific quality of life score SWAL-QOL; swallowing function scale score
Secondary Outcome Indicators: Fujishima Ingestion-Swallowing Function Grade Score; TV Fluoroscopy for Swallowing Function VFSS: Adverse Reaction
2.1.5 Exclusion criteria
Results of no quantitative analysis (meta analysis) in systematic reviews; literature with duplicate data published
2.2 Literature search strategies
Cochrane library, PubMed, SCI, Embase and four Chinese databases of ChinaNet, Weipu, Wanfang, and Chinese Biomedical Literature Service are searched by computer. On October 31, 2010, through the search method of subject words combined with free words, the Chinese search keywords were "acupuncture", "electroacupuncture", "acupuncture", "acupoint", "stroke", "stroke", "swallowing" Obstacles "," Swallowing difficulties "," Swallowing "," System reviews "," Meta-analysis "," Meta-analysis "," Metaanalysis ", English search keywords are" acupuncture "," needling "," prodding "," electro -acupuncture "," Post-stroke Dysphagia "," Dysphagia "," Deglutition Disorders "," Swallowing Disorder "," meta "," Systematic review ". In addition, by re-searching the references of the retrieved documents, and searching for missing documents through mainstream search engines, the integrity of the search is guaranteed. The Pubmed retrieval strategy is shown in Figure 1:

Figure 1 Pubmed retrieval strategy diagram
2.2.1 Literature screening
According to the conditions set in the research plan, after the training, the two researchers (Fan Weijing and Liang soldier) determined the subject words and free words according to their respective search habits, and independently searched the relevant literature. The two conducted cross-checks, the two of them agreed to resolve or consulted a third-party expert (Liu Guobin).
2.2.2 Data extraction
Two researchers (Fan Weijing and Huang Renyan) extracted the data, including the author, article title, keywords, publication time, publication period, the baseline condition of the study, intervention measures, quality evaluation tools, and outcome indicators. The lack of information in the literature should be supplemented by the original authors as far as possible.
2.3 Quality Evaluation and Statistical Analysis
2.3.1 Methodological Quality Evaluation
The AMSTER-2 scale was used to assess the methodological quality of the included studies; the ROBIS tool was used to assess the risk of bias in the included systematic reviews [4-6].
2.3.2 Evaluation of the quality of evidence
Grad [7-8] was used to grade the quality of evidence for the outcome indicators of the included studies.
3. Results
3.1 Literature search process
After a preliminary search, a total of 148 Chinese and English literatures were retrieved. Through the elimination of duplicate literatures, the exclusion of acupuncture stimulation, moxibustion and other non-acupuncture interventions, and finally included in the systematic review of acupuncture treatment of stroke after stroke There are 9 meta analyses, and the specific search process is shown in Figure 2:

Figure 2 Literature screening process (PRISMA 2009)
3.2 Including the basic characteristics of systematic reviews
The nine systematic reviews included were published from 2016 to 2019, of which one was in English and eight were in Chinese. The original studies that were included in the systematic review were 71, the least were 9 and the most included were 6010 patients, at least 577 patients; the specific basic characteristics of the study are shown in Table 1:
3.3 Methodological quality evaluation of the included literature
3.3.1 AMSTER-2 Methodological Quality Evaluation Results
The AMSTER-2 scale was used to evaluate the methodological quality of 9 systematic reviews. Because all the studies had more than 1 key entry non-conformance and 1 or more non-key entry non-conformances, all systematic review methodological quality Both are extremely low quality. In the systematic review included in this study, item 1 “Include the elements of the standard PICO”, item 5 “Literature screening”, item 8 “Basic information included in the study”, and item 11 “Statistical analysis methods” report are complete and the report is not good Key items include Item 2 "Previous Research Protocol", Item 15 "Publishing Bias Analysis", and non-key items include Item 16 "Potential Conflict of Interest". The specific report is shown in Table 1:

Table 1 Basic characteristics of included studies
3.3.2 ROBIS bias risk assessment results
Using the ROBIS tool to conduct a bias risk assessment of 9 systematic reviews, the assessment is divided into three stages:
Phase one:
In the 9 systematic reviews / meta analyses, the target population, intervention measures, control measures, outcome indicators, and the exact match rate of the target were all 100%, as shown in Table 2: Phase two:
Domain 1: 0 systematic reviews / meta analysis followed predetermined goals and inclusion criteria, 9 systematic reviews / meta analysis may follow; 4 systematic reviews / meta analysis [9-11, 14] Questions, 5 systematic reviews / meta analysis [12-13, 15-17] may be suitable; 9 systematic reviews / meta analysis include clear criteria; 9 systematic reviews / meta analysis are suitable based on the characteristics of the study; 9 systems Evaluation / meta analysis is appropriate in relation to the source of the study. In this area, all the systematic review / meta analysis answers all the landmark questions with "yes" or "maybe", and the risk of bias is "low risk".
Domain 2: 0 systematic reviews / meta analysis The scope of searching related databases and electronic resources is appropriate, 9 systematic reviews / meta analysis is not suitable; 1 systematic review / meta analysis [10] uses methods other than databases Relevant studies were identified, 8 systematic reviews / meta analyses were not used; 0 systematic reviews / meta analysis terms and structures could search for as many matching studies as possible, 9 systematic reviews / meta analyses may not; 9 systems Evaluation / meta analysis is appropriate based on time, language, and publication restrictions; 9 systematic evaluation / meta analysis screens minimize errors. In this field, all the systematic review / meta analysis search scopes are not comprehensive, neither methods other than databases are used, nor the search structure is perfect, the comprehensiveness of the search cannot be guaranteed, and the risk of bias is "high risk".
Domain 3: 2 systematic reviews / meta analysis [11, 14] Minimized errors in data extraction, 7 systematic reviews / meta analysis did not reduce; 9 systematic reviews / meta analysis had sufficient research characteristics to interpret the results ; 9 systematic reviews / meta analyses may have extracted all research results for data synthesis; 7 systematic reviews / meta analyses used appropriate tools to assess the risk of bias, and 2 systematic reviews / meta analyses [14, 17] were not used; Nine systematic review / meta analysis bias risk assessments did not minimize errors. In this field, 7 systematic reviews / meta analysis could not know whether the data extraction and quality evaluation reduced errors. Another 2 articles did not use appropriate tools to evaluate the risk of bias, and 1 article [11] the risk of bias was "uncertain". The risk of 8 biases was "high risk".
Domain 4: 6 systematic reviews / meta analyses [9-11, 14, 16-17] Data synthesis may include all studies that should be included; 0 systematic reviews / meta analyses follow all pre-set data analyses, 9 No systematic review / meta analysis related information; 9 systematic review / meta analysis data synthesis methods are appropriate; 9 systematic review / meta analysis have minimal or heterogeneous heterogeneity; 3 systematic review / meta analysis [9, 11, 14] The results were stable or sensitive; zero systematic review / meta analysis bias was minimal or processed in data synthesis. Inthis field, all the original studies of systematic review / meta analysis have obvious bias. The synthesis of six systematic review / meta analysis data may ignore some research results, and the results are unstable or insensitive. Therefore, three articles [9, 11 14] The risk of bias is "uncertain", and the risk of 6 articles is "high risk".
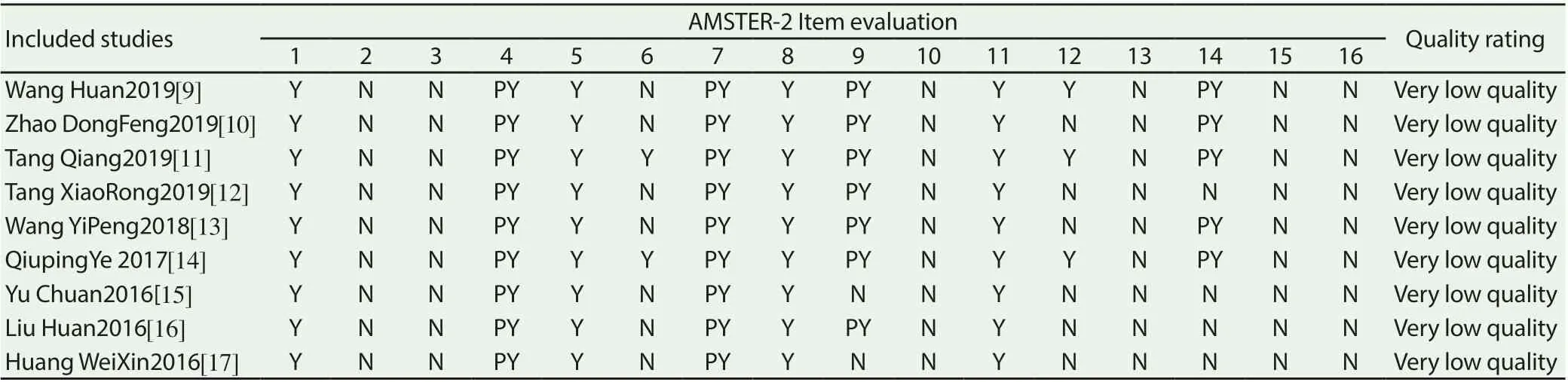
Table 2 AMSTER-2 methodological quality evaluation results

Table 3 ROBIS bias risk assessment stage one
Phase three:
0 systematic reviews / meta analyses dealt with all the risks of bias in stage two, 9 systematic reviews / meta analyses considered the relevance of the included studies and systematic review studies more reasonably, and 9 systematic reviews / meta analyses avoided emphasizing statistics Meaningful results. Based on the above 3 questions, none of the 9 systematic reviews / meta analyses have explained and dealt with all the biases in Phase 2. Therefore, they are “high-risk biases”. As shown in Table 3:
3.4 Outcome indicators efficacy and evidence quality grading
A total of 9 systematic reviews and 36 outcome indicators are shown in Table 4, Table 5, and Table 6:
3.4.1 Clinical effectiveness
A total of 9 studies reported on clinical effectiveness. All studies have concluded that acupuncture has improved the symptoms of dysphagia after stroke significantly better than the control group, of which 4 [9, 11, 12, 13] the quality of evidence is intermediate ( RR = 3.64,95% CI: 2.31 ~ 5.73, P <0.00001; OR = 3.66,95% CI: 2.66 ~ 5.05, P <0.00001; RR = 1.22,95% CI: 1.16 ~ 1.28, P <0.00001; OR = 4.05,95% CI: 3.03 ~ 5.42, P <0.00001), the quality of 4 items [10, 15-17] was low, and the quality of 1 item [14] was very low.
3.4.2 Fujishima Ingestion-Swallowing Function Rating
A total of 2 studies reported Fujishima's feeding-swallowing function grade scores. All studies concluded that acupuncture treatment of post-stroke dysphagia improved Fujishima's feedingswallowing function score significantly better than the control group, one of which [9] The quality of evidence was intermediate (MD = 2.00, 95% CI: 1.80 ~ 2.20, P <0.00001), and one item [17] was of low quality.
3.4.3 Rating of Dysphagia Scale
A total of 4 studies reported dysphagia scale scores. All studies concluded that acupuncture for dysphagia after stroke had improved dysphagia scale scores significantly better than the control group, of which 3 [12-14] the quality of evidence was Low level (MD = 2.01, 95% CI: 1.78 ~ 2.24, P <0.00001) (MD = 1.30, 95% CI: 0.56 ~ 2.05, P <0.00001), the quality of one item [16] was extremely low.
3.4.4 SWAL-QOL Specific Quality of Life Score for Dysphagia
A total of 2 studies reported dysphagia-specific quality of life scores, and all studies concluded that acupuncture treatment of stroke-related dysphagia-specific improvements in dysphagiaspecific quality of life scores was significantly better than the control group, one of which [10] evidence The quality was intermediate (MD = 14.50, 95% CI: 8.64 ~ 20.36, P <0.00001), and the quality of one item [9] was extremely low.
3.4.5 VFSS for swallowing function TV fluoroscopy
A total of 3 studies reported on fluoroscopy of swallowing function. All studies concluded that acupuncture treatment of swallowing disorders after stroke improved the fluoroscopy of swallowing function significantly better than the control group, of which 2 [11, 17] evidence The quality is low (MD = 2.31, 95% CI: 1.75 ~ 2.87, P <0.00001) (MD = 1.24, 95% CI: 0.28 ~ 2.21, P <0.00001), and the quality of one item [13] is very low.
3.4.6 Standard Swallowing Function Rating Scale SSA
A total of 2 studies reported on the standard swallowing function evaluation scale, and all studies believed that acupuncture treatment of stroke swallowing disorders after stroke improved the standard swallowing function evaluation scale significantly better than the control group, of which one item [11] was Intermediate level (MD = -3.20, 95% CI: -3.78 ~ -2.61, P <0.00001), 1 item [14] was of low quality.
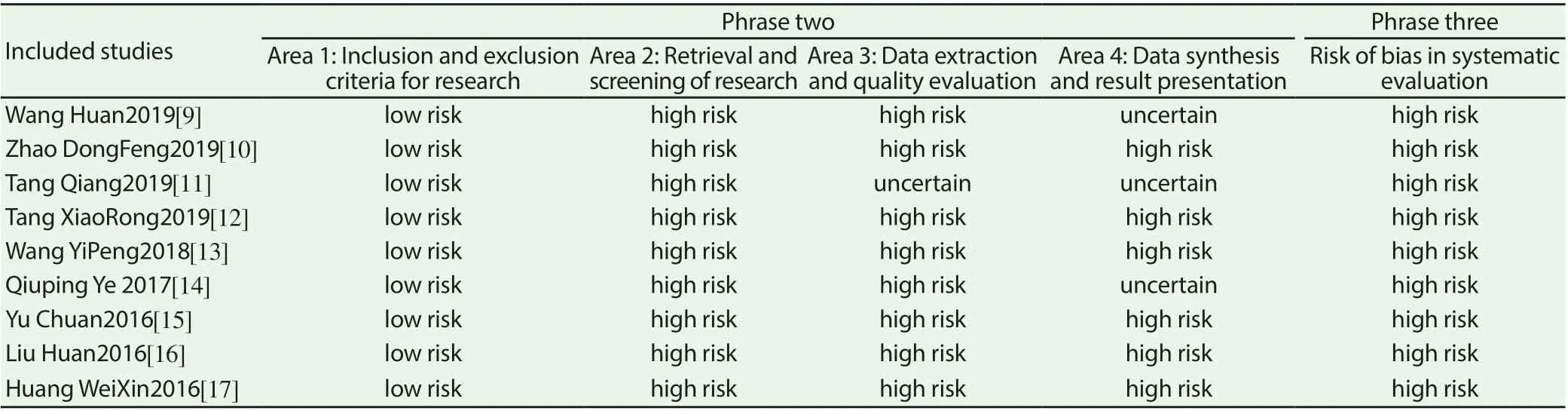
Table 4 ROBIS Bias Risk Assessment Phases 2 and 3

Table 5 GRADE grades included in the system review (1)

Table 6 GRADE grades included in the system review (2)

Table 7 GRADE grades included in the system review (3)
3.4.7 Watian drinking water score
A total of 7 studies reported the Watian drinking water score, and all studies believed that acupuncture treatment of swallowing disorders after stroke improved the Watian drinking water score significantly better than the control group, of which 4 [11-14] the quality of evidence was low-grade ( MD = -5.98,95% CI: -7.04 ~ -4.91, P <0.00001) (MD = -0.65,95% CI: -0.91 ~ -0.39, P <0.00001) (MD = -0.66,95% CI:- 0.78 ~ -0.53, P <0.00001) (MD = -0.61,95% CI: -0.80 ~ -0.43, P <0.00001), the quality of 3 items [9, 16-17] was extremely low.
3.4.8 Improved Barthel Index
A total of 1 studies [10] reported the modified Barthel index. The study suggested that acupuncture treatment of stroke after stroke had improved the modified Barthel index significantly better than the control group, and the quality of evidence was low (WMD = 12.36, 95% CI: 9.17 ~ 15.55, P <0.00001).
3.4.9 Adverse reactions
A total of 4 studies [9-10,14,17] reported adverse reactions. All studies believed that acupuncture treatment of stroke after stroke had significantly better adverse reactions than the control group, and the quality of evidence was low.
3.4.10 Swallowing Function Rating
A total of 1 studies [14] reported the scores of the swallowing function scale. The study suggested that acupuncture treatment of stroke swelling disorders after stroke improved the score of the swallowing function scale significantly better than the control group. % CI: 1.18 ~ 1.79, P <0.00001).
3.4.11 Activity scores for daily living
A total of 1 studies [14] reported the daily living activity ability scores. The study found that acupuncture treatment of post-stroke dysphagia was significantly better than the control group in daily life activity scores, and the quality of evidence was low (MD = 7.46, 95% CI: 5.49 ~ 9.47, P <0.00001).
Not downgraded to high-level evidence, downgraded to intermediate-level evidence, downgraded to two-level evidence, downgraded to third-level evidence
4. Discussion
Swallowing disorder, as a serious complication after stroke, has received widespread clinical attention in recent years. Modern medicine believes that the central nervous system has structural and functional plasticity and reorganization capabilities. Acupuncture at acupoints such as Fengfu, Lianquan, Yifeng, Jinjin, and Yuye can stimulate and regulate the function of the pharyngeal nerve, thereby helping to repair the reflex arc of swallowing [18].
4.1 Acupuncture is effective in treating swallowing disorders after stroke, and the quality of evidence needs to be further improved
This study used the GRADE scale to evaluate the quality of evidence for 36 outcome indicators, of which 7 outcome indicators were intermediate evidence, 22 outcome indicators were low-level evidence, and 7 outcome indicators were very low-level evidence. Four of the seven intermediate evidences were clinical effectiveness, one was Fujishima's feeding-swallowing function score, one was swallowing disorder-specific quality of life score, and one was the standard swallowing function assessment scale. The results show that the clinical efficacy of acupuncture in the treatment of dysphagia after stroke is practical and effective, and the outcome indicators of various swallowing functions and adverse reactions have been improved to varying degrees, but in addition to a high proportion of clinical effectiveness Intermediate evidence, other outcome indicators did not have much evidence of intermediate quality and above, mostly low-level or even very low-level evidence.
4.2 Acupuncture is low in the quality of systematic reviews related to dysphagia after stroke and the risk of bias is high
The AMSTER-2 scale and ROBIS tools were used in this study. The results show that the quality of all systematic review methodologies is extremely low, and the risk of bias is high. All the systematic reviews included did not explain the registration of the previous research plan; all the systematic reviews only searched the database, and did not explain the search methods and other search methods of the gray literature; all the systematic reviews were not included in the article or A detailed list of excluded literature is provided in the supporting materials, which reduces the repeatability of the research process. The lack of the above key items seriously affects the quality of the included studies and causes a high risk of bias. In addition, all studies are made to explain conflicts of interest. 2. All studies did not explain the specific types of studies included, which affected the rigor of the study.
4.3 Systematic review of acupuncture treatment of dysphagia after stroke should pay attention to the standardization of research report writing
Through this re-evaluation of the systematic review of dysphagia after acupuncture treatment of stroke, the reason that affects the systematic review methodological quality score is largely not due to errors and deficiencies in the research protocol or research implementation in the research report, but because The research report is incomplete. Many items were not stated in the research report, and after contacting some researchers, it was found that the reason for this result was that the researcher did not have a systematic understanding of the writing of the systematic review research report, especially the Chinese report. Writing one by one in accordance with the PRISMA statement led to the inability to evaluate the correct methodological quality of the report, which not only reduced the credibility of the study, but also interfered with the clinician's judgment of the evidence.
4.4 Limitations
This study still has certain limitations. First, this study only searches databases and network engines. It does not search conference papers and dissertations that are not on the Internet. The research results may have selective bias. Second, In this study, only the AMSTER-2 scale and ROBIS tools were used to evaluate the systematic review methodological quality and bias risk. The comprehensive evaluation of multiple assessment scales in the same aspect was not used. The scale itself may have limitations. Sex.
4.5 Summary
A systematic review of acupuncture for post-stroke dysphagia was re-evaluated. Acupuncture is effective in treating post-stroke dysphagia. There are multiple intermediate levels of evidence. In addition, acupuncture has fewer adverse reactions and scores on the swallowing function scale. , Fujishima Ingestion-Swallowing Function Rating Score, Standard Swallowing Function Rating Scale Score, Swallowing Specific Quality of Life Score, Swallowing Difficulty Scale Score, Swallowing Function TV Fluoroscopy Results, Improved Barthel Index, Watian Drinking Water Score, Daily Life activity ability scores all improved, but the level of clinical evidence was low, both low-level and very low-level. The methodological quality evaluation results of all systematic reviews are extremely low-quality and the risk of bias is high. It is recommended that future acupuncture treatment of post-stroke dysphagia-related systematic review design be more rigorous, and that attention be paid to the registration of research protocols. In terms of research, researchers should write research reports strictly in accordance with the PRISMA statement, and all items should be reported in detail whether they are implemented or not.
This research report has no conflicts of interest
 Journal of Hainan Medical College2020年11期
Journal of Hainan Medical College2020年11期
- Journal of Hainan Medical College的其它文章
- The potential mechanism of prevention and treatment of COVID-19 by shufeng jiedu capsule was studied based on network pharmacology
- A case of recurrent PMT caused by poor atrial pacing
- Experience of Professor Shao Mingxi in treating knee osteoarthritis based on "Bin Si Xue" acupuncture
- Meta analysis of Masquelet technology and Llizarov technology in the treatment of infectious bone defects
- Effect of TGIF1 expression on epithelial cadherin and Twist1 protein expression in breast cancer cells
- Establishment and evaluation of Type 2 Diabetes Mellitus andits complications induced by low dose of multiple streptozotocin