
Survey and analysis of anxiety of 804 residents in Hainan during the COVID-19 epidemic
2020-07-10 07:13:34GuoTianLinChanJuanZhaoFanZhangHuaNuoFengLiuTingLinYuFeiZhai
Guo-Tian Lin, Chan-Juan Zhao, Fan Zhang , Hua-Nuo Feng, Liu-Ting Lin, Yu-Fei Zhai
1School of Public Health, Hainan Medical University, Haikou, Hainan, 571199 2Hainan Health School, Haikou, Hainan, 570311
Keywords:COVID-19 Anxiety Psychological counseling
ABSTRACT Objective To understand the cognitive status and anxiety factors of COVID-19 in 804Hainan residents during the epidemic of corona virus disease 2019 (COVID-19). Methods A crosssectional survey was conducted on 804 Hainan residents. A non-randomized convenient sampling method combining with online and snowball recruitment method was used. Results
1. Introduction
At the end of 2019, a novel corona virus (severe acute respiratory syndrome coronavirus, SARS-CoV-2) began to spread in Wuhan, China,, which is one of the causes of severe respiratory infections in humans. The virus can cause fever, cough, and fatigue [1-3]. On January 22th, 2020, the Hainan Provincial Health and Health Commission announced that the first imported cases had occurred in Sanya, Hainan. As of April 22th, 168 confirmed cases had been reported in the province. On 11st February, at the Global Forum on Research and Innovation, held in Geneva, the World Health Organization (WHO) announced that the disease caused by SARS-CoV-2 was named corona virus disease 2019(COVID-19). WHO declared a global pandemic on March 9th. COVID-19 is a major infectious disease emerging after the SARS、MERS and a public safety threat to people's lives. Its incubation period is short, infectious and generally susceptible to the population [4-6]. In order to control the epidemic situation, Hainan had taken various effective measures, such as the implementation of a strict isolation system, the cessation of assembly activities, temporary classes in schools at all levels, temporary employment in entertainment places, and various prevention and control methods reported by the news media. In the early stage of the epidemic situation in Hainan, in order to quickly understand the impact of the epidemic situation on the psychology of the people in the province and provide basic information for the prevention and control of the local epidemic situation, the research group carried out a network investigation for some residents of our province, and now the results are summarized as follows.
2. Research Object and Methods
2.1 Research object
From January 31st to February 8th,2020, using the network "questionnaire star" platform to distribute questionnaires to mobile phone users in Hainan through WeChat, QQ and other social software channels ,901 questionnaires were recovered, of which 804 were valid answers, and the effective rate was 89.2%.
2.2 Research methodology
2.2.1 Sampling methodology
The research team invited friends to fill out the online questionnaire through the online recruitment method, and then they sent the QR code or link of the online questionnaire through snowballing to conduct a survey. A total of 901 questionnaires were collected. Collected questionnaires were cleared out and excluded as invalid if; 1) it was filled in less than 2 minutes, 2) the participant did not live in Hainan Province,3) the mobile phone IP address was duplicated, and the verification had obvious logical errors. Finally, a total of 804 valid questionnaires were used for data analysis, and the questionnaire efficiency rate was 89.2%.
2.2.2 Questionnaire design
The questionnaire was compiled with the health belief model as the framework, referring to the relevant literature at home and abroad, and consulting epidemiologists, after the pre-investigation of the questionnaire was constantly revised to form a formal questionnaire "Hainan Province residents of the COVID-19 cognitive and anxiety status questionnaire". The questionnaire includes three parts:(1)basic demographic characteristics: sex, age, nationality, education, conscious physical condition, etc.; (2) knowledge of SARS-CoV-2 and COVID-19 covering clinical symptoms, transmission routes, protective measures, etc.; (3) self-designed questionnaire of COVID-19 anxiety symptoms[7-8], including the questions of 'If someone has a fever, you feel nervous or anxious ’," if you can't stop or control your worries about an epidemic"," if you worry too much about all sorts of things, it's hard to relax "," because you're afraid, often sleep badly or have nightmares"," because you can't sit still because you're upset, you're prone to worry or impatience" and" if you feel like something terrible happens, you're afraid ".The Alpha of Colognebach was 0.879 after reliability test, which showed the questionnaire with good reliability.
2.2.3 Scoring criteria
There were 5 multiple-choice questions about the knowledge of COVID-19, 20 points for each questions, and 0 points for less or wrong choices, a total of 100 points. The P75 of the overall cognitive score was used as the cut-off [9], that is, the total score 80 is divided into high cognition, otherwise it was low cognition; the anxiety symptom questionnaire has a total of 6 questions. The main evaluation was based on the frequency of the symptoms defined by the question, which was divided into 4 levels: no, several days, more than a week, and almost every day, and the score of which were respectively marked as 1, 2, 3, 4 in order. The higher the score, the higher the degree of anxiety. The P75 of the overall anxiety score was used as the cut-off value for the presence or absence of anxiety symptoms. is the total score of this part 15 was defined as anxiety symptoms, otherwise was none[9].
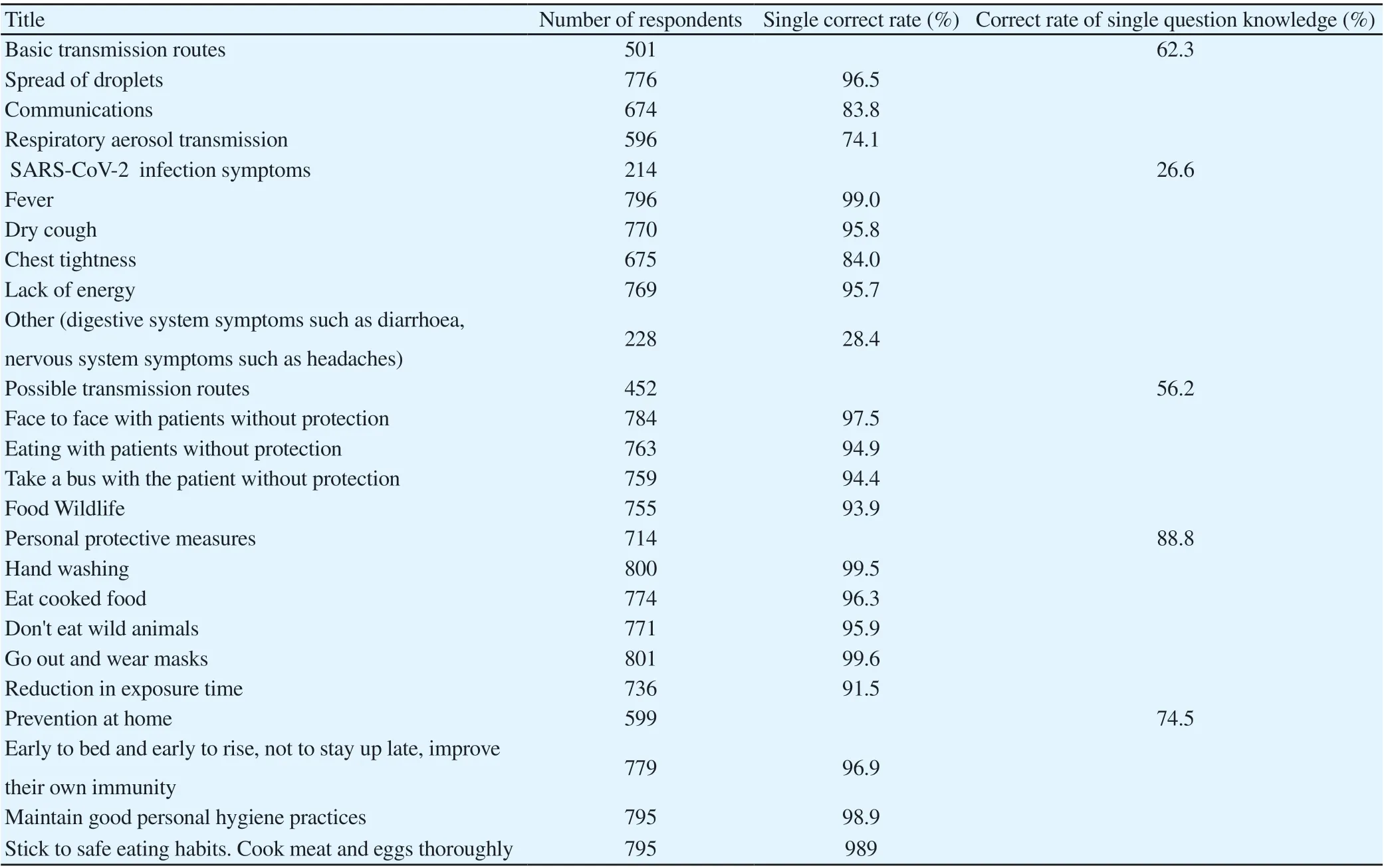
Table 1. COVID-19 related knowledge awareness
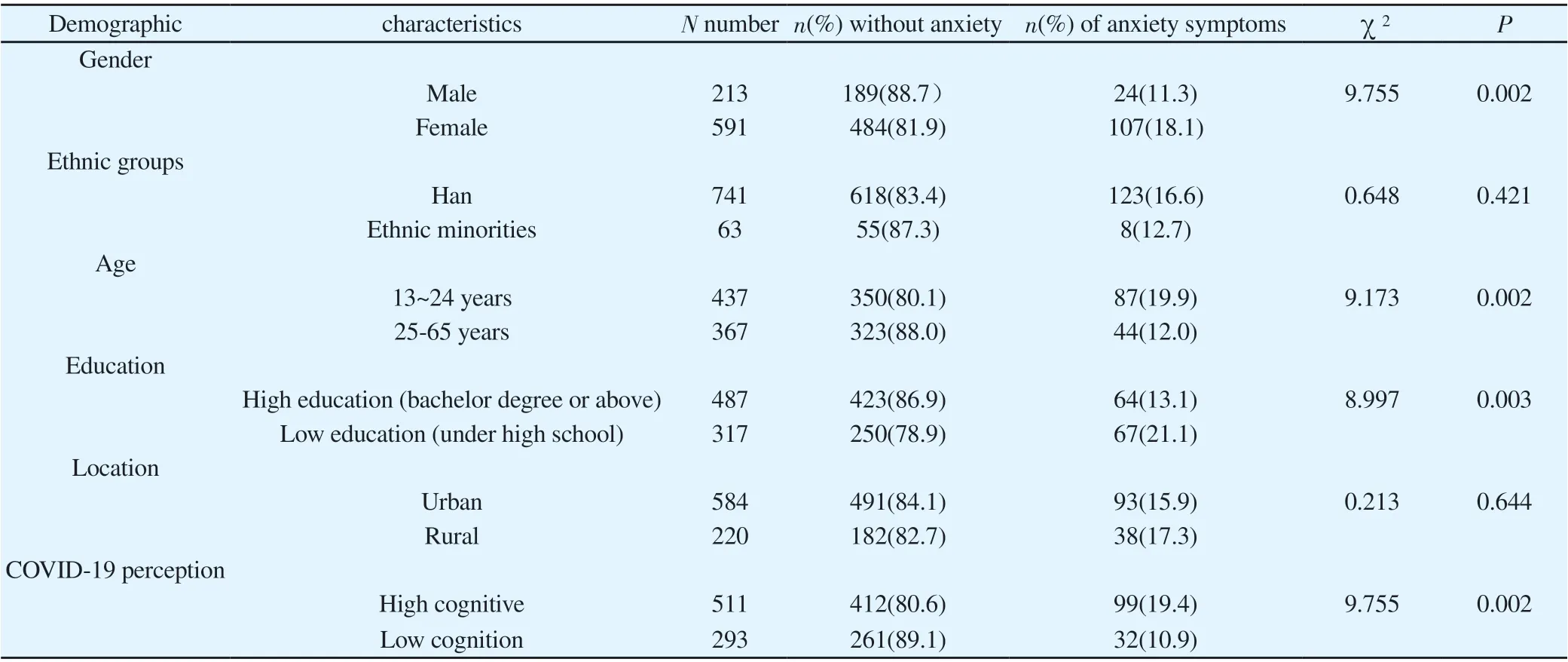
Table 2 Anxiety scores among different demographic characteristics
2.2.4 Assessment indicators
The awareness rate of COVID-19 related knowledge was calculation as: single question knowledge correct rate =(answer the question number / total answer number) 100%, total awareness rate =(total score 60 points number / total answer number)100%; anxiety total score 24 points, anxiety value 15 points defined as anxiety symptoms.
2.2.5 Quality control
An electronic questionnaire by using the App of 'questionnaire star’ was completed and submitted by mobile phone for no less than 2 minutes. The non-conforming questionnaire was eliminated by checking the collected questionnaire according to the location, time, address IP mobile phone and logic of the questionnaire.
2.3 Statistical analysis
the data were derived through the ‘questionnaire star’ platform, collated by Excel 2016, and SPSS 25.0 software was used for statistical analysis. The statistical analysis methods included descriptive analysis, two independent samples of knowledge, anxiety score t test, variance analysis, knowledge, anxiety classification variables test, and binary Logistic regression analysis. The test level was set as 0.05. After normality test, the known scores and anxiety values were normally distributed (P>0.05).
3. Results
3.1 Demographic characteristics
The survey collected 804 valid questionnaires, including 213 males and 591 females, with a ratio of 1:2.8 males ;The Han nationality account for 92.2%; average age (27.7 ± 10.90) years old, the maximum age was 65 years old, and the minimum age was 13 years old. The age 24 years old [10]account for45.6%(367/804);Bachelor degree or above accounted for 60.6% (487/804); urban work accounted for 72.6% (584/804).
3.2 COVID-19 Knowledge Awareness
The scores of 804 objects on COVID-19 related knowledge were (61.2±22.45) point, and the total awareness rate was 71.5%(575/804). According to the scoring standard of SARS-CoV-2 related knowledge questionnaire, the high cognition (total score ≥80) accounted for 63.6%(511/804). Among them, the correct rate of personal protective measures was the highest, which was 88.81%, followed by home prevention measures (74.50%), basic transmission routes (62.30%), possible routes of infection (56.22%), and low awareness of infection symptoms (26.62%), as shown in Table 1.
3.3 Anxiety distribution in 804 subjects
As a result ,804 residents had a score of anxiety (10.39±4.574) during the epidemic, and the incidence of anxiety symptoms was 16.3%(131/804). The differences were statistically significant among the population of different sex, age, education and cognitive level (P <0.05), and the incidence of anxiety symptoms was higher among women ,13~24 years old, low education and high cognition of COVID-19, as detailed in Table 2.
3.4 Survey of Anxiety Symptoms
Of the 804 subjects surveyed, the scores for "someone with a fever, you feel nervous, anxious, or anxious" and "you can't stop or control worries for an outbreak" were higher, at (2.0±1.04) and (2.2±1.19), and the scores for "feeling almost daily" were 16.7% and 25.0%, respectively, compared to other anxiety symptom entries, see Table 3.
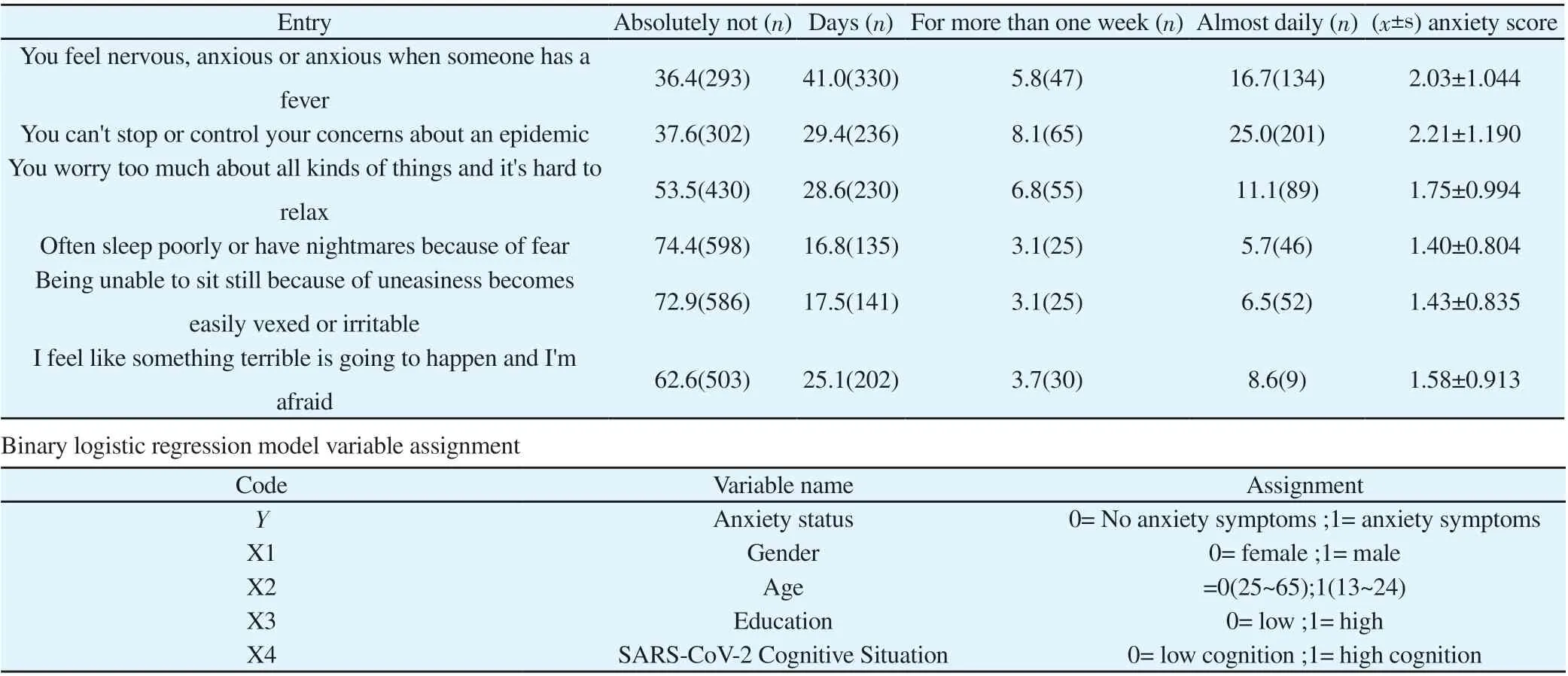
Table 3. Anxiety symptom entries for subjects surveyed
3.5 Analysis of multi factors affecting anxiety
Using anxiety status as dependent variable, four single-factor analysis of meaningful variables, such as sex, age, education and cognitive status of COVID-19-related knowledge, were introduced into the binary logistic regression model, and the selected variable standardα=0.05. The coding and assignment of independent variables are shown in Table 4. The results showed that the model was meaningful (=18.476, P <0.001). The main influencing factors of anxiety among 804 Hainan residents are age, gender and knowledge about COVID-19, and men are 0.563 times more likely to have anxiety symptoms than women (95% CI, 0.348 ~ 0.911), and 13-24 years old 1.76 times (95% CI, 1.124 ~ 2.499) 25 to 65 years old, 1.53 times higher anxiety symptoms than low cognition (95% CI, 1.022 ~ 2.296), Table 5.
4. Discussion
4.1 Low awareness of atypical symptoms of COVID-19
Women accounted for 73.5%(591/804) of the total study subjects, and the female response was relatively high. Women may be more concerned about trends in the epidemic, and studies had shown that women are less psychologically resilient than men and are more likely to develop anxiety than men[11-14]. The total awareness rate was 74.5%, among which the awareness rate was relatively high for personal protective measures (88.8%) and home-based measures to prevent infection (74.5%), while the awareness of COVID-19 atypical clinical symptoms such as diarrhea and headache was relatively low (28.4%). This indicates that during COVID-19 epidemic period, COVID-19 typical clinical symptoms and personal protection propaganda by the news media were much larger than those of atypical clinical symptoms, mainly due to the early stage of the epidemic, and the clinical symptoms of most patients in COVID-19 were mainly fever and respiratory symptoms[1]As some atypical and even asymptomatic infections are the most easily neglected source of infection, the relevant departments should strengthen the correct guidance and publicity of COVID-19, especially the publicity of atypical clinical symptoms.
4.2 Increased anxiety among Hainan residents during the epidemics
COVID-19 epidemic is another major public health crisis after SARS、MERS, each public health crisis will have an impact on people's lives and mental health. This survey showed that the incidence of anxiety symptoms in 804 Hainan residents was 16.3%(131/804), which was higher than that in the general population during the SARS epidemic (12.5%, =7.138, P=0.008).[15]Because the outbreak severely endangered human health and the number of infections continued to increase during the investigation, and the vaccines and special drugs have not yet been successfully developed, people often have many feelings of uncertainty and insecurity, so they show varying degrees of anxiety [16]. In the survey results, the incidence of anxiety symptoms was relatively high among females, 13-24 years old, and low-education populations. It may be that women are more concerned about the development of the epidemic than men, and women are generally more vulnerable than men to mental tolerance [17],and it may be related to the higher response rate of women in this survey. The incidence of anxiety symptoms in people aged 13-24 was higher than that in people 25-65 years old probably because most people aged 25-65 years had experienced major epidemics of SARS, MERS and other infectious diseases, and there are certain empirical effects on psychological response. Multi-factor results showed that the main factors affecting the anxiety of 804 Hainan residents during the COVID-19 epidemicare age, gender, and related knowledge of the COVID-19 , which prompts relevant departments to promote content Fully consider the needs of key populations [18].

Table 5 Results of Regression Analysis of Two Logisitic Affecting Anxious Smoking in Hainan Province during COVID-19 Period
From a psychological point of view, in the early stage of a major public health crisis, the people to produce appropriate stress psychology to help prevent and control the epidemic, but excessive tension may be counterproductive, not only may affect the autoimmune function, resulting in a decline in the body's immunity, increasing the risk of infection [19], but also not conducive to social stability and overall prevention and control. As a result, government departments should continue to strengthen the guidelines and publicity for the prevention and control of the epidemic, especially the discovery of asymptomatic infections, before COVID-19 vaccines and specific drugs are available[3].At the same time, we should pay attention to mental health care and maintain mental health[20],In order to overcome the epidemic situation, it is particularly important to carry out special propaganda on psychological guidance and face the epidemic situation with a good attitude.
 Journal of Hainan Medical College2020年9期
Journal of Hainan Medical College2020年9期
- Journal of Hainan Medical College的其它文章
- Effect of aripiprazole and olanzapine on the cognitive function in patients with schizophrenia
- Evaluation of hepatic fibrosis parameter model and elastic modulus of liver and spleen for the diagnosis of hepatic fibrosis in chronic hepatitis b
- Mid-term follow-up of one-stage posterior debridement, intertransverse process bone grafting and screw-rod system fixation for Brucella spondylitis of the lumbar spine
- Effects of virtual reality balance games combined with muscle strength training on balance function and motor ability of Parkinson's patients
- Analysis of treatment strategies of traditional Chinese medicine for COVID-19 in tropical regions based on the pathogens of dampness and heat
- Epidemiological characteristics of 168 cases of COVID-19 in Hainan Island, tropical China: A descriptive study