
Single-balloon and spiral enteroscopy may have similar diagnostic and therapeutic yields to double-balloon enteroscopy:Results from a meta-analysis of randomized controlled trials and prospective studies
2020-05-19 06:22:32YongGuXinShiYanYangXiaoFeiYeQiongWuZhiPingYangShuiXiangHe
World Journal of Meta-Analysis 2020年2期
Yong Gu, Xin Shi, Yan Yang, Xiao-Fei Ye, Qiong Wu, Zhi-Ping Yang, Shui-Xiang He
Yong Gu, Shui-Xiang He, Department of Gastroenterology, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an 710061, Shaanxi Province, China
Yong Gu, Department of Digestive System Diseases, Shaanxi Provincial Crops Hospital of Chinese People's Armed Police Force, Xi'an 710054, Shaanxi Province, China
Xin Shi, Yan Yang, Qiong Wu, Zhi-Ping Yang, State Key Laboratory of Cancer Biology, National Clinical Research Center for Digestive Diseases and Xijing Hospital of Digestive Diseases,Fourth Military Medical University, Xi'an 710032, Shaanxi Province, China
Xiao-Fei Ye, Department of Health Statistics, Second Military Medical University, Shanghai 200433, China
Abstract
Key words: Double-balloon enteroscopy; Single-balloon enteroscopy; Spiral enteroscopy;Meta-analysis; Randomized controlled trials
INTRODUCTION
When double-balloon enteroscopy (DBE) was introduced into the clinic by Yamamoto in 2001[1], dramatic changes have happened in the diagnosis and management of disorders in the distant part of small bowel, which were dependent on surgically assisted enteroscopy or rope guided enteroscopy before.Currently, there are another two different systems:Single-balloon enteroscopy (SBE) and spiral enteroscopy (SE).Although the balloon-assisted enteroscopy techniques follow the push-and-pull principle, SE is dependent on a new system:Pleating of the small bowelviarotation[2].
There have been several randomized controlled trials (RCTs) comparing DBE with SBE[3-6].In these studies, DBE has been shown to be similar to SBE with regard to diagnostic/therapeutic yield, depth of maximal insertion, and procedure time, but superior to SBE in terms of total enteroscopy.There have been seven studies including four RCTs and three prospective studies comparing DBE with SE[2,7-12].In these studies,diagnostic yield was supposed to be similar between DBE and SE.Two recent metaanalyses only compared DBE with SBE, and did not evaluate SE[13,14].Another metaanalysis compared balloon enteroscpy (combined DBE with SBE) with SE[15].Moreover, these three meta-analyses included May’s study, in which SBE was not really applied but by detaching one balloon from double-balloon enteroscope[16,17].In addition, they did not include Chinese studies due to language barrage.
Therefore, we conducted a meta-analysis aimed to evaluate the efficacy of DBE,SBE, and SE for the management of small bowel diseases.
MATERIALS AND METHODS
The methodology and reporting of this study followed the PRISMA statement guidelines recommended by Cochrane collaboration for meta-analysis[18].
Data sources and searches
A comprehensive literature search was independently performed by two authors.The search was performed on MEDLINE, PubMed, EMBASE, Cochrane Library, and Chinese CQVIP database (http://en.cqvip.com/) from January 2008 to October 2018,using the search terms “balloon enteroscopy”, “single balloon enteroscopy”, “double balloon enteroscopy”, and “spiral enteroscopy”.Boolean operators AND, OR, and NOT were used.Meanwhile, abstracts from the conference proceedings were also retrieved.
Study selection
RCTs and prospective studies comparing DBE, SBE, and SE were eligible for inclusion.Retrospective studies and non-comparative studies that used only DBE,SBE, or SE were excluded.The studies were restricted to studies performed in human and published in English and Chinese.And a manual search of the references of all retrieved studies was performed in case of omission of the ongoing or completed trials.Two investigators independently assessed the eligibility and validity of each study.Queries concerning inclusion were resolved by discussion and consensus between the two reviewers.
Outcome measures
The primary outcome evaluated in this study was diagnostic yield rate, defined as the percentage of enteroscopy procedures with findings relevant to the indication of the procedure[10].Other outcomes were therapeutic yield rate, total enteroscopy rate,depth of maximal insertion (DMI), time to maximum insertion, and examination time(per-oral and per-anal).
Data extraction
The following data from each study were extracted:First author’s name, publication year, country, study design, interventions, patient demographics, indications, number of endoscopies, diagnostic and therapeutic yields, DMI, time to maximum insertion,and examination time (per-oral and per-anal).Different opinions between the reviewers were revolved through discussion.
Risk of bias assessment
As described in the Cochrane Handbook for Systematic Reviews of Interventions[19],we assessed the quality of RCT based on random sequence generation, allocation concealment, blinding of participants and investigators, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias.We used the Newcastle-Ottawa Scale to assess the quality of prospective study[20].Any disagreement was resolvedviadiscussions.
Statistical analysis
Statistical analyses were performed using RevMan software (version 5.3; Copenhagen:The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).Standard deviation was obtained from the range and interquartile range as recommended[21,22].Results are expressed as odds ratio (OR) for categorical variables or mean difference (MD) for continuous variables with 95% confidence interval (CI).Heterogeneity was assessed usingI2test.P< 0.05 orI2> 50% was considered as significant heterogeneity.A fixedor random-effects model was used, depending on the absence or presence of significant heterogeneity.Potential for publication bias was assessed by funnel plot.P< 0.05 was considered statistically significant.
RESULTS
Description of studies
The detailed steps of our literature search are shown in Figure 1.Briefly, a total of 384 articles were identified.After screening, 22 potentially relevant articles and abstracts were retrieved from the electronic databases.After excluding 11 studies based on the predefined inclusion criteria, 11 studies were identified.Six trials compared DBE with SE[2,8-12], four compared DBE with SBE[3-6], and one compared SBE with SE[7], which were evaluated separately in the meta-analysis.Baseline characteristics and outcome measures are shown in Tables 1 and 2.The risks of bias of the RCTs included in this meta-analysis are detailed in Supplementary Figure 1.Each prospective study achieved eight points in assessing quality according to the Newcastle-Ottawa Scale.
DBE vs SE
There were six comparisons of DBEvsSE:Five from Europe and one from Asia[2,8-12].Three were RCTs[2,8,11]and three were prospective studies[9,10,12].A total of 370 procedures were analyzed, including 255 DBE and 115 SE procedures.
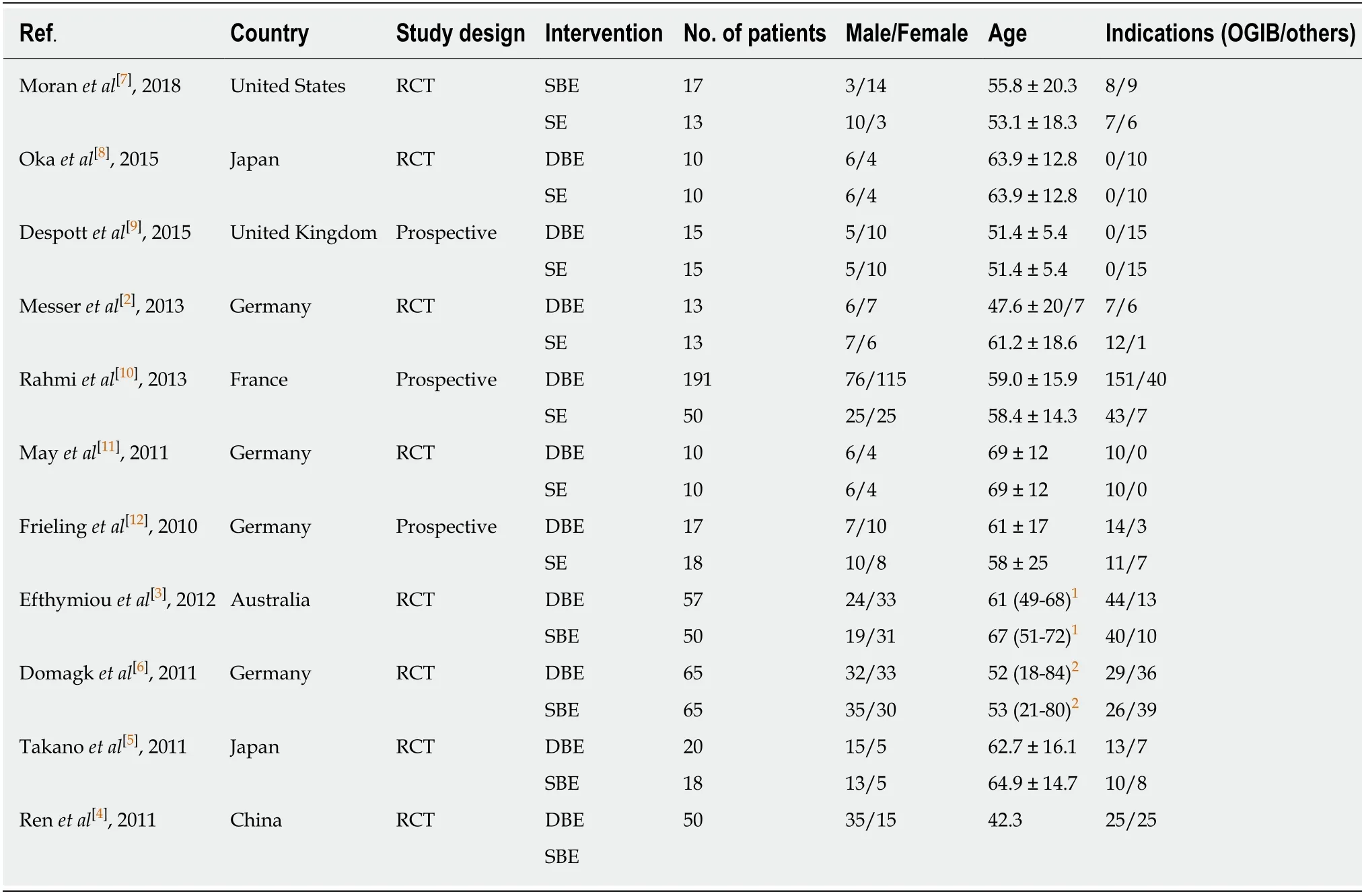
Table 1 Study characteristics
As shown in Figure 2, there was no significant difference in diagnostic yield (OR =1.19, 95%CI:0.68-2.08) or therapeutic yield (OR = 1.17, 95%CI:0.61-2.23) between DBE and SE.DBE resulted in deeper DMI (MD = 36.76, 95%CI:5.09-68.43), corresponding to longer time to maximum insertion (MD = 15.14, 95%CI:12.00-18.27) and examination time (MD = 12.98, 95%CI:9.57-16.38).There was no statistical heterogeneity between the studies with regard to diagnostic yield, therapeutic yield,DMI, time to maximum insertion, and examination time (P> 0.05).The funnel plot did not show publication bias in terms of diagnostic yield between DBE and SE(Supplementary Figure 2).
DBE vs SBE
There were four RCTs comparing DBE with SBE[3-6].A total of 327 procedures were analyzed, including 171 DBE and 156 SBE procedures.
As shown in Figure 3, there were no significant differences in diagnostic yield (OR= 0.85, 95%CI:0.55-1.33), therapeutic yield (OR = 1.71, 95%CI:0.64-4.60), total enteroscopy (OR = 6.10, 95%CI:0.31-118.52), DMI (MD = -20.42, 95%CI:-89.29-48.45),per-oral examination time (MD = -7.45, 95%CI:-36.60-21.16), or per-anal examination time (MD = 2.48, 95%CI:-6.49-11.44).There was no statistical heterogeneity between the studies with regard to diagnostic yield, therapeutic yield, or per-anal examination time (P> 0.05).The funnel plot did not show publication bias in terms of diagnostic yield between DBE and SBE (Supplementary Figure 3).
SBE vs SE
We could not conduct a meta-analysis since there was only one trial comparing SBEvsSE.In the single trial[7], patients needed for an anterograde enteroscopy were randomized to receive SBE (n= 17) or SE (n= 13), thus evaluating a direct comparison between SBE and SE.However, this was insufficient to compare these modalities using meta-analysis.In this trial which ceased without reaching the required sample size, there were no significant differences identified between SBE and SE with regard to diagnostic yield (41%vs69%,P= 0.16), therapeutic yield (24%vs46%,P= 0.26),DMI (285.3 ± 80.8 cmvs330.0 ± 88.2 cm,P= 0.16), or procedure time (38.3 ± 12.4vs37.0 ± 10.5,P= 0.76).
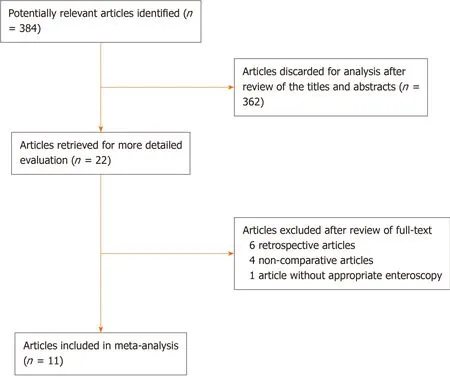
Figure 1 Flow chart.
Sensitivity/subgroup analysis
We did not perform additional sensitivity or subgroup analysis to assess the observed heterogeneity due to limited number of studies.
DISCUSSION
Although the small intestine has long been considered the final frontier of endoscopy,significant progress in small-bowel enteroscopy techniques has led to increased diagnostic and therapeutic capabilities[23].This meta-analysis including 727 patients, to our knowledge, is the first systemic meta-analysis comparing DBE, SBE, and SE with regard to clinical outcomes.Our study showed that DBE and SBE had similar clinical outcomes.We also identified that the diagnostic and therapeutic yields were comparable between DBE and SE.It was noteworthy that compared with DBE, SE had shorter procedural time but less depth of insertion.However, SE needs further evaluation vs SBE for clinical outcomes.
In our meta-analysis, double- and single-balloon systems showed similar performance in diagnostic and therapeutic yields, DMI, time to maximum insertion,and examination time.As for diagnostic yield, these four RCTs included in our study showed no significant difference.But in two retrospective studies we excluded[24,25],diagnostic yields were significantly higher in SBE, compared to the DBE group (61.7%vs48.2%,P< 0.001; 62.0%vs35.6%,P= 0.014).Nevertheless, retrospective studies easily suffered from patient selection bias, which was also declared by the author.These findings are consistent with previous meta-analyses[13,14].However, the two meta-analyses included May’s study[17]which was based on the P-type Fujinon instrument for both DBE and SBE.Although the P-type enteroscope allowed deeper intubation in the small bowel, therapeutic maneuvers were difficult to perform using this instrument in comparison with the T-type[26].Lipkaet al[14]mentioned that the Psystem was less comparable to the Olympus system used in the other trials.Although results were similar to the previous, our study excluding that trial may be more credible.It is interesting that these two meta-analyses included the same four RCTs but reached the controversial conclusion in terms of total enteroscopy rate.Wadhwaet al[13]concluded that DBE was superior to SBE with regard to complete small bowel visualization (relative risk [RR] = 0.37, 95%CI:0.19-0.73), while Lipka not (RR 1.73,95%CI:0.86-3.48).The recommendation to prefer DBE in patients in whom total enteroscopy is desired may be based on the feeling of many endoscopists.In our study, total enteroscopy rate tended to be higher in DBE than SBE, although the difference was not significant (OR = 6.10, 95%CI:0.31-118.52).Complete enteroscopymay not be necessary to make a diagnosis, but it plays a role in determining the extension of a known disease and the number of the lesions, especially for the fact that many small bowel diseases are not solitary but multiple, such as vascular malformations, polyps in polyposis syndrome, or Crohn’s stenosis[27].Similarly,previous studies have shown that the rate of complete enteroscopy by using the DBE method is approximately 40% to 80%[28], while the rates of SBE decreased to approximately 5% to 25%[29,30].If complete enteroscopy is needed for identifying the extent and number of the lesions, specifically for those once diagnosed by capsule endoscopy with multiple lesions, we recommended DBE technique because it provides a higher rate of complete enteroscopy at present[27].
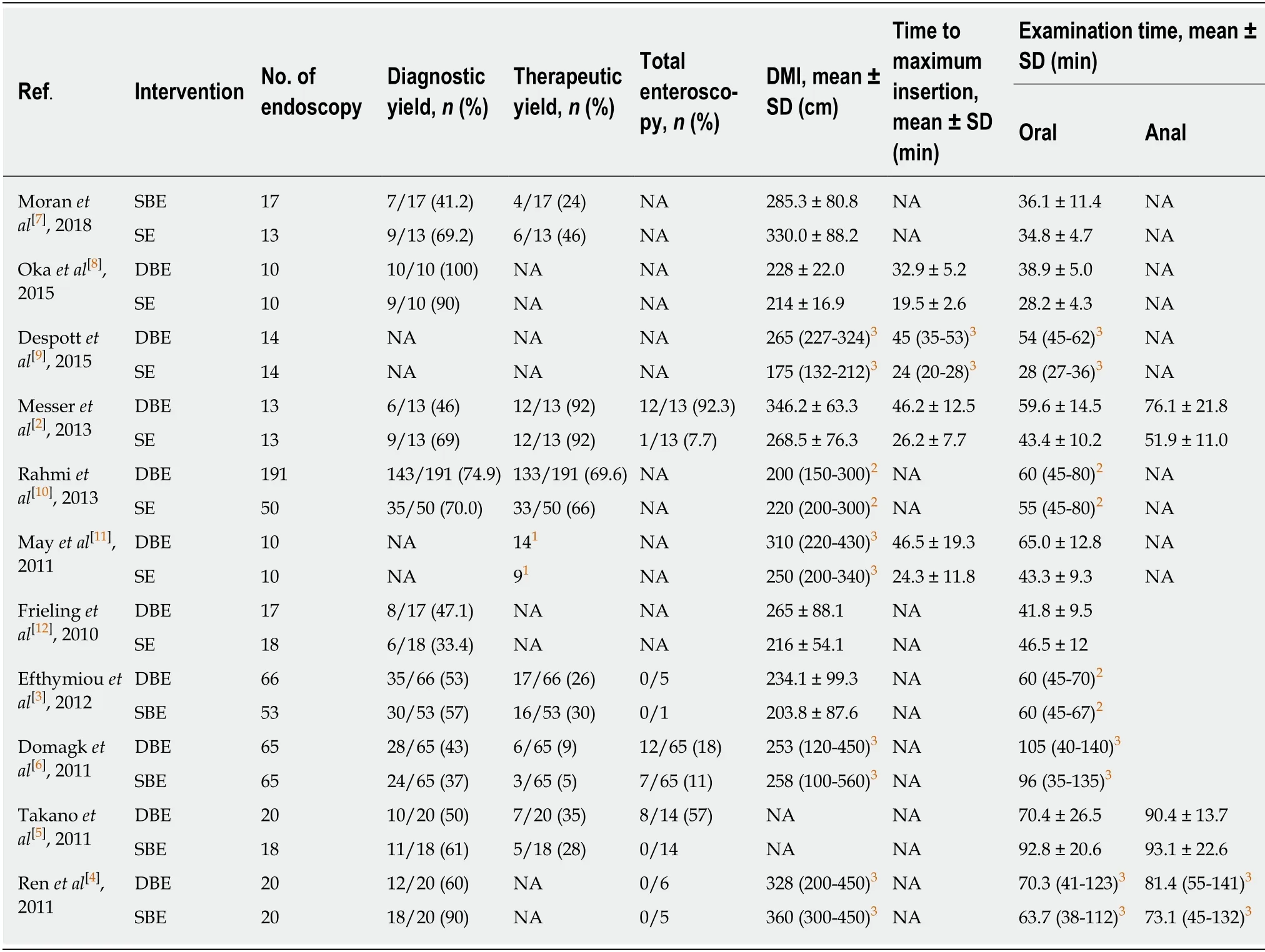
Table 2 Outcome measures of enteroscopy
Spiral enteroscopy, first reported in 2009[31], is another newly developed enteroscopy, which was found to have the advantages of shorter examination time and being more stable within the bowel, thus allowing controlled examination of the intestinal mucosa[31-33].The previous meta-analysis conducted by Baniyaet al[15]combined prospective and retrospective studies, demonstrating that balloon enteroscopy (DBE + SBE) and SE were similar with regard to diagnostic and therapeutic success rates and DMI, but the procedure time was significantly less for the SE group.Excluding retrospective study, we identified three RCTs and three prospective studies comparing DBE with SE, and found that there were no significant differences between DBE and SE with regard to diagnostic and therapeutic yields.However, our study showed that DBE resulted in deeper DMI, in cost of longer procedure time, which is consistent with previous studies[2,9,11].Although the difference was not significant, DBE tended to achieve deeper small bowel insertion compared to SE[8,12].Only one study compared DBE and SE in terms of total enteroscopy, and the total enteroscopy rate was 92% in the DBE group and 8% in the SE group (P= 0.002)[2].Compared with SE, we also recommended DBE if complete enteroscopy was needed.

Figure 2 Outcome measures between double-balloon enteroscopy and spiral enteroscopy.
Up to now, there have been only two studies testing SEvsSBE.One RCT conducted by Moranet al[7]showed no significant differences between SE and SBE with respect to diagnostic yield, therapeutic yield, DMI, and procedure time.One retrospective study conducted by Khashabet al[23]showed that SE and SBE were similar in diagnostic yield but the insertion depth was significantly higher in SE.Small sample size and retrospective design prevented giving a definitive judgement, and future adequately powered prospective study is required to confirm these findings.
Recently, a novel motorized spiral endoscope has been introduced into clinical evaluation[34].This novel enteroscopy is currently been evaluated for its efficacy and safety in three prospective clinical trials.It seems to provide a faster and deeper approach to the small bowel with similar safety and efficacy to balloon enteroscopy[35].

Figure 3 Outcome measures between double-balloon enteroscopy and single-balloon enteroscopy.
There were some limitations to the current study.First, the sample sizes of studies we included were small and we lacked high-quality prospective randomized multicenter trials.Second, a limited number of studies obstructed subgroup and sensitivity analyses.Third, there was no uniform method for insertion depth estimation and different methods of enteroscopic distance estimation were used,which may have an impact on the results[23].Fourth, due to limited studies comparing SBE with SE, we could not conduct a meta-analysis.Fifth, we only identified and included those studies that were published in English and Chinese because of the language barrier for the authors.Therefore, our meta-analysis may not include some useful published in other kinds of languages.Finally, peroral enteroscopy tended to provide higher diagnostic and therapeutic yields than peranal method.However, a limited number of studies also obstructed separate analysis.
In conclusion, the present meta-analysis has demonstrated that DBE and SBE have similar clinical outcomes.Compared with DBE, SE seem to have similar diagnostic and therapeutic yields, but shorter procedural time in cost of less depth of insertion.SE needs further evaluationvsSBE for clinical outcomes.DBE is recommended for complete enteroscopy.
ARTICLE HIGHLIGHTS
Research background
There are three different methods for the management of disorders in the distant part of small bowel:Double-balloon enteroscopy (DBE), single-balloon enteroscopy (SBE), and spiral enteroscopy (SE).
Research motivation
The efficacy of the three methods in terms of diagnostic and therapeutic yield rates, total enteroscopy rate, depth of maximal insertion, time to maximum insertion, and examination time remains unclear.
Research objectives
We aimed to compare the efficacy of DBE, SBE, and SE for the management of small bowel diseases.
Research methods
We searched randomized controlled trials and prospective studies in MEDLINE, PubMed,Embase, Cochrane Library, and Chinese CQVIP database.Statistical analyses were performedviaRevMan software.
Research results
The diagnostic and therapeutic yields did not differ significantly when comparing DBE with SE and DBE with SBE.Total enteroscopy, examination time, time to maximum insertion, and depth of maximal insertion were similar between SBE and DBE.DBE was superior to SE with regard to depth of maximal insertion, with longer time to maximum insertion and examination time.
Research conclusions
DBE and SBE may have similar clinical outcomes.Compared with DBE, SE seems to have similar diagnostic and therapeutic yields, but shorter procedural time in cost of less depth of insertion.
Research perspectives
SE needs further evaluationvsSBE.DBE is recommended for complete enteroscopy.
 World Journal of Meta-Analysis2020年2期
World Journal of Meta-Analysis2020年2期
- World Journal of Meta-Analysis的其它文章
- Effectiveness and safety of sedation in gastrointestinal endoscopy:An opinion review
- Chinese research into ulcerative colitis from 1978 to 2017:A bibliometric analysis
- Systematic review with meta-analysis of the epidemiological evidence relating smoking to type 2 diabetes
- Utility of gastrointestinal ultrasound in functional gastrointestinal disorders:A narrative review
- Treatment strategies and preventive methods for drug-resistant Helicobacter pylori infection
- Helicobacter pylori and gastric cardia cancer:What do we know about their relationship?