
FOLFOXIRI vs FOLFIRINOX as first-line chemotherapy in patients with advanced pancreatic cancer: A population-based cohort study
2020-05-16 06:38:58AngliqueVienotHortenseChevalierClmentBologniniElisabetaGhergaElodieKlajerAurliaMeurisseMarineJaryStefanoKimChristelleEngremontThierryNguyenFabienCalcagnoHamadiAlmotlakFrancineFeinMeherNasriSyrineAbdeljaouedAnthonyTurpinC
Angélique Vienot, Hortense Chevalier, Clément Bolognini, Elisabeta Gherga, Elodie Klajer, Aurélia Meurisse,Marine Jary, Stefano Kim, Christelle d’Engremont, Thierry Nguyen, Fabien Calcagno, Hamadi Almotlak,Francine Fein, Meher Nasri, Syrine Abdeljaoued, Anthony Turpin, Christophe Borg, Dewi Vernerey
Angélique Vienot, Clément Bolognini, Elodie Klajer, Marine Jary, Stefano Kim, Thierry Nguyen,Fabien Calcagno, Hamadi Almotlak, Christophe Borg, Department of Medical Oncology,Besançon University Hospital, Besançon F-25030, France
Angélique Vienot, Aurélia Meurisse, Marine Jary, Stefano Kim, Syrine Abdeljaoued, Christophe Borg, Dewi Vernerey, University Bourgogne Franche-Comté, INSERM, EFS BFC, UMR1098,Interactions Hôte-Greffon-Tumeur/Ingénierie Cellulaire et Génique, Besançon F-25000,France
Angélique Vienot, Marine Jary, Stefano Kim, Christophe Borg, INSERM CIC-1431, Clinical Investigation Center in Biotherapy, Besançon University Hospital, Besançon F-25030, France
Hortense Chevalier, Anthony Turpin, Department of Medical Oncology, Lille University Hospital, Lille F-59000, France
Elisabeta Gherga, Meher Nasri, Department of Medical Oncology, Nord Franche-Comté Hospital, Montbéliard F-25020, France
Aurélia Meurisse, Dewi Vernerey, Methodological and Quality of Life in Oncology Unit,Besançon University Hospital, Besançon F-25030, France
Christelle d’Engremont, Francine Fein, Department of Gastroenterology, Besançon University Hospital, Besançon F-25030, France
Abstract
Key words: Advanced pancreatic cancer; First-line chemotherapy; FOLFOXIRI;FOLFIRINOX; Propensity score; Cohort study
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) carries a poor prognosis, with a 5-year overall survival (OS) rate of only 8%-9% for all stages taken together[1]. Pancreatic cancer is expected to become the second leading cause of cancer death in the United States and Europe by 2030[2,3]. This poor prognosis is mainly due to late diagnosis,with only 20% of patients with PDAC eligible for surgery. Complete surgical resection of localized PDAC followed by 6 mo of adjuvant chemotherapy is the only recognized standard of care that has been shown to improve patient survival, with a median OS up to 54.4 mo with modified FOLFIRINOX [5-fluorouracil (5-FU), irinotecan, and oxaliplatin][4]. Furthermore, more than 80% of cases are diagnosed at an advanced,unresectable stage, with almost 50% of patients presenting with metastatic disease and almost 30% with locoregional extension[1]. In addition, it has been shown that most patients who undergo surgery develop further tumor recurrence[4].
Advanced or recurrent PDAC remains a challenging, non-curable disease, for which therapeutic options are still limited and mainly rely on supportive care and systemic chemotherapy to improve patient OS and health-related quality of life(HRQoL)[5]. Up to 2010, gemcitabine was the only standard of care as first-line chemotherapy (L1) in patients with metastatic PDAC[6]. Over the last decade,incremental progress has been achieved in the landscape of advanced PDAC (aPDAC)management with the approval of two active cytotoxic combinations, namely FOLFIRINOX, and gemcitabine plusnab-paclitaxel regimens[7,8]. FOLFIRINOX polychemotherapy became a reference regimen in this setting, based on the results of the PRODIGE 4/ACCORD 11 phase III trial[7]. This study demonstrated the superiority of FOLFIRINOX over gemcitabine monotherapy in terms of OS (median:11.1vs6.8 mo;P< 0.001) and progression-free survival (PFS; median: 6.4 movs3.3 mo;P< 0.001) in 342 selected patients with metastatic PDAC, age < 76 years, Eastern Cooperative Oncology Group performance status 0-1, and normal bilirubin level (<1.5 times the upper limit of normal). The objective response rate for FOLFIRINOX was 31.6%vs9.4% for gemcitabine (P< 0.001). FOLFIRINOX consisted of oxaliplatin (85 mg/m2), irinotecan (180 mg/m2), leucovorin (400 mg/m2), and 5-FU (400 mg/m2administered by intravenous bolus, followed by 2400 mg/m2given as a 46-h continuous infusion), every 2 wk[7].
The HRQoL of patients was significantly better with FOLFIRINOX as compared with gemcitabine, except for diarrhea[9]. A higher incidence of adverse events was observed with the FOLFIRINOX group, including grade 3 or 4 neutropenia (45.7%),febrile neutropenia (5.4%) and diarrhea (12.7%)[7]. A retrospective study evaluated a“modified FOLFIRINOX” regimen without the bolus of 5-FU, and administration of hematopoietic growth factors to all patients with aPDAC[10]. This study showed a better safety profile (grade 3 or 4 neutropenia 3%), and maintained efficacy, with a response rate of 30% and a median OS of 16.4 mo (9 mo for metastatic disease).However, the incidence of severe diarrhea remained high, at 13%[10].
FOLFOXIRI, another modified schedule was developed based on the experience of the Gruppo Oncologico Nord Ovest (GONO) in metastatic colorectal cancers[11]to limit digestive and hematological toxicities. This regimen consisted of a lower dose of irinotecan (165 mg/m2), no bolus of 5-FU, and an increase in continuous intravenous 5-FU infusion at 3200 mg/m2, while oxaliplatin and leucovorin remained unchanged.To the best of our knowledge, to date, the FOLFOXIRI and FOLFIRINOX regimens have never been compared head-to-head. In this exploratory population-based cohort study, we aimed to compare clinical outcomes, in terms of safety and efficacy,between the FOLFOXIRI and FOLFIRINOX regimens, in patients with aPDAC in routine clinical practice.
MATERIALS AND METHODS
Patients
All consecutive patients with histologically proven aPDAC (i.e., metastatic, locally advanced, or recurrent after surgery) who were treated in L1 in two French institutions were included. Patients treated with FOLFOXIRI were enrolled at Besancon University Hospital, between January 2011 and December 2015, whereas,the FOLFIRINOX group comprised patients who received this standard regimen at Lille University Hospital, between January 2011 and December 2017. Patients were prospectively identified through the chemotherapy prescribing software used at Besancon (Bonnes Pratiques de la Chimiothérapie - BPC®, SQLI) and Lille University Hospitals (CHIMIO®, Computer Engineering). Patients with early postoperative tumor relapse (i.e., within 6 mo after the last administration of the adjuvant chemotherapy) were excluded. All therapeutic decisions were discussed and validated during digestive oncology-dedicated multidisciplinary meetings. Computed tomography-scan assessment was performed every 3 mo.
The database was registered and declared to the National French Commission for bioinformatics data and patient liberty (CNIL; No. of CNIL declaration: 1906173 v 0).The study followed standard procedures in France, with approval by the relevant institutional review boards. All patients with cancer signed a general informed consent at the time of their first visit to both Medical Oncology Departments. This consent allows the use of their clinical and biological data in the cohort study. No additional specific informed consent for this study was deemed necessary.Demographics, cancer history, pathological, clinical, biological, and radiological parameters at chemotherapy initiation, as well as treatment outcomes, were retrospectively collected from medical records. The database was locked on April 23,2019.
Treatment regimens
FOLFIRINOX was administered according to the standard schedule validated by the PRODIGE 4/ACCORD 11 study. This regimen consisted of a combination of oxaliplatin (85 mg/m2, over 2 h), followed by leucovorin (400 mg/m2, over 2 h), with the addition through a Y-connector, after 30 min, of irinotecan (180 mg/m2, over 90 min), followed by 5-FU (400 mg/m2) by intravenous bolus, on Day 1. Then, a continuous intravenous infusion of 5-FU (2400 mg/m2) was administered over 46 h starting on Day 1[7]. FOLFOXIRI consisted of the same molecules with a reduced dose of irinotecan and no bolus 5-FU, according to the GONO regimen used in metastatic colorectal cancer: Irinotecan (165 mg/m2, over 1 h), followed by oxaliplatin (85 mg/m2) and leucovorin (200 mg/m2) concomitantly over 2 h through a Yconnector,on Day 1; and followed by a continuous intravenous infusion of 5-FU (3200 mg/m2)over 48 h starting on Day 1[11]. These two treatments were administered every 2 wk until disease progression or unacceptable toxicity. Hematopoietic growth factors were systematically used after each chemotherapy cycle in at least 80% of cases in the FOLFIRINOX group and for all patients enrolled in the FOLFOXIRI group.
Statistical analysis
Median value (interquartile range) and frequency (percentage) were provided for the description of continuous and categorical variables, respectively. Medians and proportions were compared between the FOLFIRINOX and FOLFOXIRI groups using Wilcoxon–Mann–Whitney and chi-square tests (or Fisher’s exact test, if appropriate),respectively. OS was calculated from the date of the first administration of L1 to the date of death from any cause. Survival data were censored at the last follow-up. PFS was calculated from the date of the first administration of L1 to the date of progression or death from any cause, or the date of the last follow-up, at which point data were censored. OS and PFS were estimated using the Kaplan-Meier method and described using median or rate at specific time points with 95% confidence intervals(CIs), and compared using the log-rank test. Follow-up time was calculated using a reverse Kaplan-Meier estimation when feasible[12]. Objective tumor response was determined according to Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 criteria[13]. Toxicity was evaluated according to the National Cancer Institute Common Terminology Criteria[14].
The primary analysis was conducted using data from the total population, and compared characteristics and outcomes between the FOLFIRINOX and FOLFOXIRI groups. A propensity score approach was then applied to deal with potential heterogeneity in baseline characteristics between the two administered regimens in L1. Two methods were used to address the potential confounding effect of the unbalanced factors: First, the inverse probability of treatment weighting (IPTW) and second, propensity score matching[15]. Propensity score construction was based on probability estimation with a nonparsimonious multivariable logistic regression model including the main parameters distributed unequally between the FOLFIRINOX and FOLFOXIRI groups. Hazard ratios (HRs) and 95%CIs were estimated using the IPTW Cox proportional hazards model. Accuracy of the model was verified by testing discrimination and calibration. Discrimination of the IPTW Cox model was assessed by the area under the curve, and calibration by the Hosmer–Lemeshow goodness-of-fit test. Propensity score matching, based on the caliper method with a ratio of 1:1, was performed to generate two samples with wellbalanced characteristics. Sensitivity analysis to determine the reliability and the robustness of the primary analysis was performed in the subgroup of patients with metastatic disease. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary NC, USA).P< 0.05 were considered statistically significant, and all tests were two-sided.
RESULTS
Patient characteristics
A total of 289 patients with aPDAC treated in L1 were included in this study. Of these patients, 124 received the FOLFIRINOX regimen and 165 received FOLFOXIRI chemotherapy. Patient characteristics of the two treatment groups are described and compared in Table 1. The two cohorts displayed similar characteristics, except for primary tumor site (located in the pancreatic head in 43.1% in the FOLFIRINOX groupvs56.7% in the FOLFOXIRI group;P= 0.022), histological grade, stage at chemotherapy initiation (88.7% had metastatic stage in the FOLFIRINOX groupvs63.6% in the FOLFOXIRI group;P< 0.001), and pain (corresponding to the prescription of morphine). Of note, patients in the FOLFIRINOX group had a significantly higher albumin level (39.1 g/Lvs35.0 g/L;P< 0.001), and an increased number of metastatic sites (P< 0.001) than those in the FOLFOXIRI group (Table 1).
Outcomes of the overall population
After a median follow-up of 30.8 mo (95%CI: 23.0-NA) and 61.4 mo (95%CI: 43.2-87.9),median OS was 11.6 mo (95%CI: 10.8-15.5) and 11.1 mo (95%CI: 9.8-13.1) in the FOLFIRINOX and FOLFOXIRI groups, respectively (HR = 1.12; 95%CI: 0.86-1.46;P=0.391; Figure 1A). Median PFS was 5.8 mo (95%CI: 3.9-6.9) in the FOLFOXIRI group and 6.7 mo (95%CI: 6.0-7.8) in the FOLFIRINOX group (HR = 1.14; 95%CI: 0.89 to 1.46;P= 0.298; Figure 1B). OS rates at 12, 18, and 24 mo were 49.6%, 36.4%, and 28.3%,respectively, in the FOLFIRINOX group as compared with 45.1%, 30.9%, and 21.2%,respectively, in the FOLFOXIRI group.
Detailed outcomes data are summarized in Table 2. The objective response rate was 47.8% in the FOLFIRINOX group, compared to 37.1% in the FOLFOXIRI group (P=0.187), while disease-control rates were 75.7% and 66.7%, respectively (P= 0.124). The number of cycles was significantly higher in the FOLFIRINOX group (11.0vs7.0 cycles;P= 0.027). Maintenance chemotherapy was administered in 45.2% of patients in the FOLFIRINOX group and in 37.6% of those in the FOLFOXIRI group (P= 0.194).The median maintenance time was 2.8 mo (95%CI: 1.0-4.4) in the FOLFIRINOX groupvs2.7 mo (95%CI: 1.9-5.8) in the FOLFOXIRI group (P= 0.421). Second-line chemotherapy was administered to 91 (73.4%) patients in the FOLFIRINOX group and 117 (70.9%) patients in the FOLFOXIRI group (P= 0.643). No treatment-related deaths were observed. Grade 3 or 4 toxicities occurred in 19.5% of patients in the FOLFIRINOX group as compared with 28.7% in the FOLFOXIRI group, but this difference did not reach statistical significance (P= 0.079). In the FOLFOXIRI group,grade 3 or 4 hematological adverse events of any type were observed in 3.1% of patients. FOLFOXIRI was associated with a higher incidence of grade 3 or 4 digestive adverse events as compared to the FOLFIRINOX group (12.8%vs4.2%, respectively).
Propensity score approach
Potential biases identified during the description of the total cohort were minimized by the use of a propensity score estimated by an unconditional multivariable logistic regression model. Histological grade and albumin level were not selected in the propensity score process due to the high rate of missing data(Supplementary Table 1). Thus, primary tumor site, stage at diagnosis, stage at chemotherapy initiation, number of metastatic sites, lymph node and liver metastases,and pain were included in the propensity score (Supplementary Table 2). The model exhibited excellent discrimination with an area under the curve of 0.73 (Supplementary Figure 1) and a good calibration (P= 0.840, Hosmer–Lemeshow goodnessoffit test). For each patient, a propensity score value was then calculated based on the multivariable model (Supplementary Figure 2). In the IPTW analysis, the L1 regimen was not significantly associated with either OS (282 patients, 236 events; HR = 1.19;95%CI: 0.91-1.54;P= 0.202) or PFS (281 patients, 256 events; HR = 1.25; 95%CI: 0.98-1.60;P= 0.077). Patients treated with the FOLFOXIRI regimen were then matched considering their nearest neighbor, with a caliper of 0.10 and a ratio of 1:1, with patients in the FOLFIRINOX group.
Patient characteristics and outcomes in the propensity scorematched population
After propensity score matching, 96 patients in each group (79.0% and 59.3% in the FOLFIRINOX and FOLFOXIRI groups, respectively) were successfully matched.There were no statistically significant differences between the two matched groups in baseline characteristics: Primary tumor site (P= 0.385), stage at chemotherapy initiation (P= 0.439), number of metastatic sites (P= 0.724), lymph node metastases (P= 0.817), liver metastases (P= 0.385), and pain (P= 0.877). Patients in the FOLFIRINOX group were characterized by tumors with a more differentiated histological grade (P= 0.011) and a higher albumin level (P= 0.001) (Table 3). After a median follow-up of 43.2 mo (95%CI: 31.0-61.4) in the matched groups, survival rates for patients remained similar between the two regimens in terms of OS (HR= 1.22;95%CI: 0.89-1.67;P= 0.219; Figure 1C) and PFS (HR = 1.27; 95%CI: 0.94-1.71;P= 0.120;Figure 1D). There was no statistically significant difference in objective response (P=0.079), maintenance chemotherapy (P= 0.553), or second-line administration rates (P= 0.636). Grade 3 or 4 toxicities remained unchanged between the two treatments(20% in the FOLFIRINOX groupvs29.2% in the FOLFOXIRI group,P= 0.148). The incidence of grade 3 or 4 digestive adverse events remained higher in the FOLFOXIRI group (9.4%vs5.6%) (Table 2).
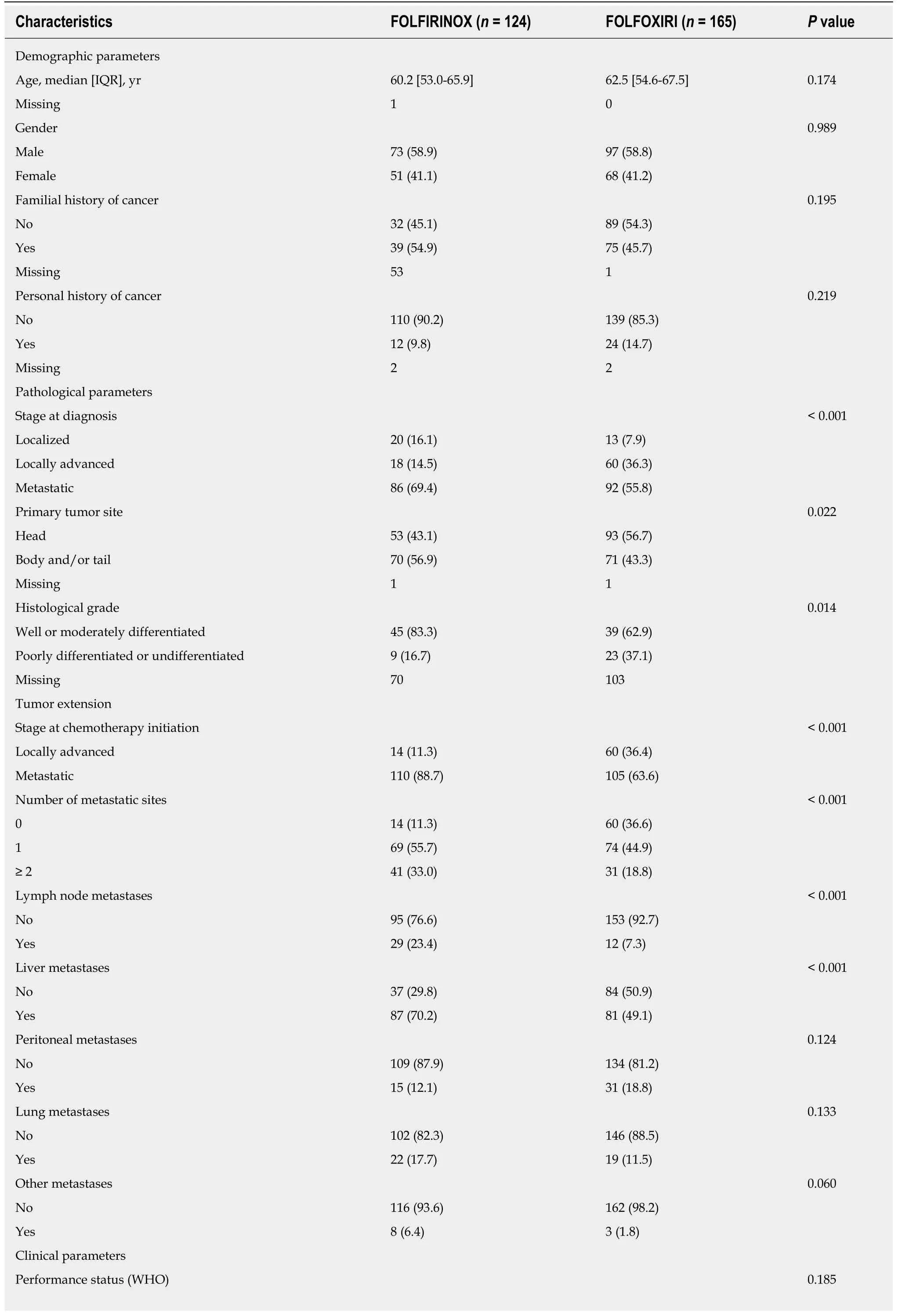
Table 1 Patient characteristics of the overall population according to first-line chemotherapy, n (%)
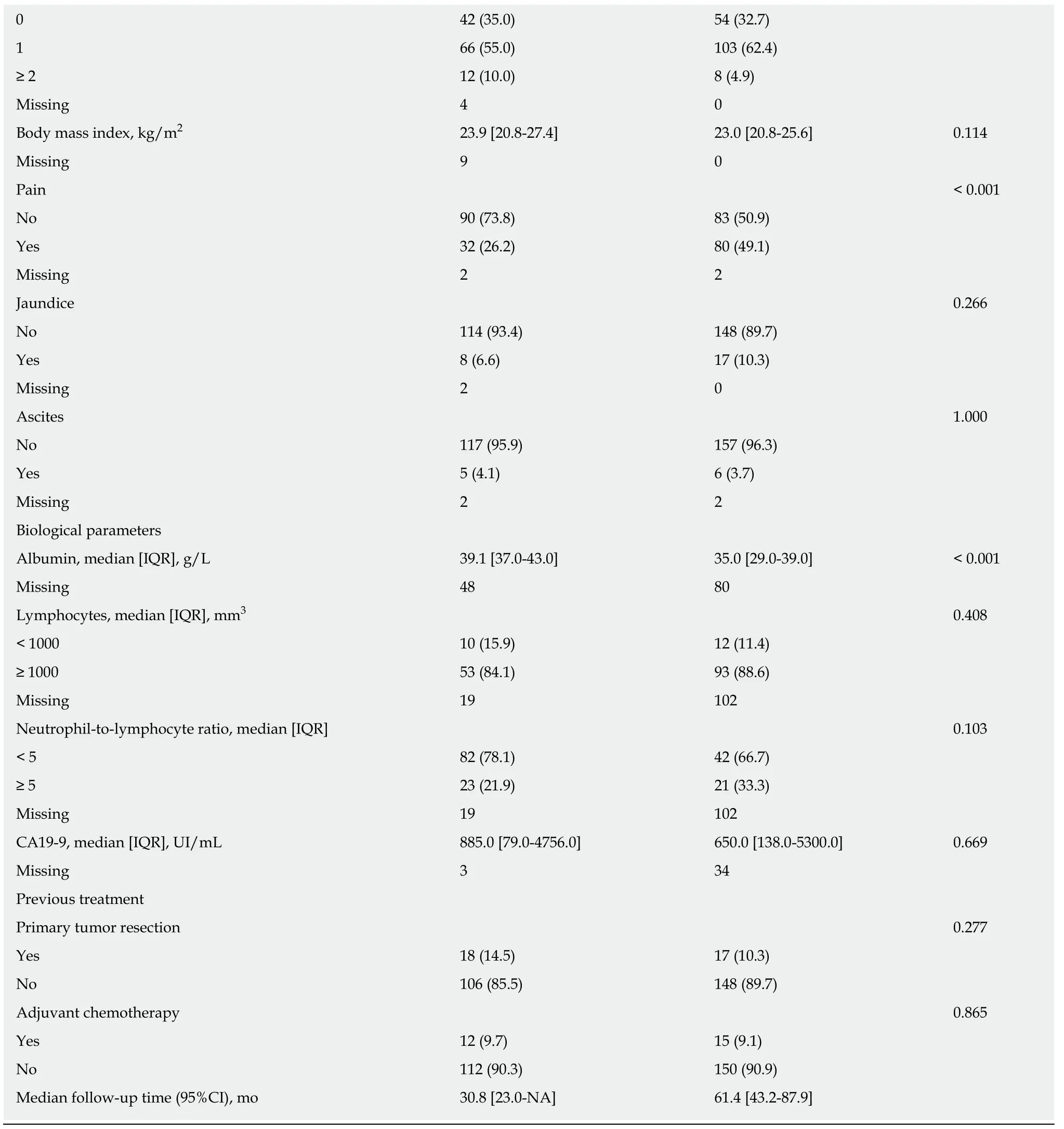
χ2 tests or Fisher’s exact tests were used to compare proportions, and Wilcoxon tests were used to compare continuous variables between the FOLFIRINOX and FOLFOXIRI groups. All statistical tests were two-sided. CA19-9: Carbohydrate Antigen 19-9; IQR: Interquartile range; WHO: World Health Organization.
Sensitivity analyses in the subgroup of patients with metastatic disease
Sensitivity analysis was performed exclusively including the metastatic population from the two treatment groups, corresponding to 110 patients in the FOLFIRINOX group and 105 patients in the FOLFOXIRI group. Patient characteristics are detailed in Supplementary Table 3. As observed for the overall population, characteristics were similar, except for histological grade, lymph node metastases, pain, and albumin level(39 g/L in the FOLFIRINOX groupvs34.6 g/L in the FOLFOXIRI group,P< 0.001).Patients in the FOLFIRINOX group displayed significantly more peritoneal metastases (86.4%vs70.5%,P= 0.005) and a lower neutrophil-to-lymphocyte ratio (P= 0.010), compared to those in the FOLFOXIRI group (Supplementary Table 3).

Figure 1 Kaplan-Meier curves of overall survival and progression-free survival for the FOLFIRINOX and FOLFOXIRI groups in the overall population and the propensity scorematched population. A
The median duration of follow-up was 26.7 mo (95%CI: 23.0-31.1) in the FOLFIRINOX group compared to 44.2 mo (95%CI: 36.7-71.5) in the FOLFOXIRI group. Median OS was significantly longer in the FOLFIRINOX group (13.3 mo;95%CI: 10.7-15.5) compared to the FOLFOXIRI group (8.5 mo; 95%CI: 6.7-10.2) (HR=1.44; 95%CI 1.07-1.94;P= 0.017; Supplementary Figure 3A). Similarly, patients treated with the FOLFIRINOX regimen had more favorable PFS (6.7 mo; 95%CI: 5.7-7.8;vs3.9 mo; 95%CI: 2.9-6.1, respectively), but the difference was not statistically significant(HR= 1.30; 95%CI: 0.97-1.72;P= 0.073; Supplementary Figure 3B). Both cohorts exhibited other similarities in outcomes, which are summarized in Supplementary Table 4.
Furthermore, propensity score analysis was performed in metastatic patients (Supplementary Tables 5 and 6, Supplementary Figures 4 and 5). In the IPTW analysis, the L1 regimen was not significantly associated with either OS (122 patients, 100 events;HR = 1.08; 95%CI: 0.73-1.60;P= 0.703) or PFS (122 patients, 113 events; HR = 1.06;95%CI: 0.73-1.55;P= 0.746). After propensity score matching(Supplementary Table 7), survival rates for patients were similar between the two regimens in terms of OS (HR = 0.94; 95%CI: 0.54-1.61;P= 0.810; Supplementary Figure 6A) and PFS (HR = 0.94; 95%CI: 0.55-1.61;P= 0.827; Supplementary Figure 6B).Moreover, no difference in objective response (P= 0.317), maintenance chemotherapy(P= 1.000), or second-line administration rates (P= 1.000) was observed. Treatmentrelated grade 3 or 4 adverse events, including digestive and hematological adverse events, were similar between the two propensity score-matched treatment groups (P=0.362) (Supplementary Table 8).
DISCUSSION
This is the first study to show, in a head-to-head comparison, that FOLFOXIRI is feasible as L1 in patients with aPDAC but does not confer any therapeutic benefit ascompared with FOLFIRINOX. PDAC is a highly aggressive cancer, and chemotherapy remains the cornerstone of advanced disease therapy. Preclinical studies showed synergistic activity between oxaliplatin, irinotecan and 5-FU[16-18], and phase II/III trials confirmed the antitumor activity of the FOLFIRINOX combination in metastatic pancreatic cancers[7,19]. Although FOLFIRINOX is a first-line option for patients with metastatic PDAC, the significant adverse event rate limits its administration in full doses. However, its substantial benefit in terms of survival rates and HRQoL encourages the assessment of a modified schedule that will likely yield a muchneeded improvement in the balance of toxicityvsefficacy in this setting.

Table 2 Outcomes in the overall population and propensity score-matched population according to first-line chemotherapy, n (%)
FOLFOXIRI, a triplet-chemotherapy regimen with a lower dose of irinotecan and no bolus of 5-FU, has already demonstrated its efficacy and good tolerance and is validated in metastatic colorectal cancer[11,20]. Vivaldiet al[21]evaluated FOLFOXIRI in pancreatic cancer in an observational cohort study of 137 patients, of whom 59.1% had metastatic disease. They reported that FOLFOXIRI improved patient survival rates with a median OS of 12 mo for the overall population and 10.8 mo for the metastatic patients. The objective response rate was 38.6% in the whole population and 35.8% in patients with metastatic PDAC. Moreover, the schedule showed a good tolerance profile with the occurrence of grade 3 diarrhea in only 8%, and febrile neutropenia(grade 3 or 4 neutropenia 35.7%) in < 1%. These results are in line with those observed in our study. Nevertheless, FOLFOXIRI was never compared head-to-head to the standard FOLFIRINOX in this setting.
In our study, the two regimens were compared for the first time in routine clinical practice, taking into account a large number of variables. Due to the design of thisexploratory study, patients were included in an observational cohort and the treatment regimens were not randomized. In addition to its retrospective nature,further limitations of the present study warrant discussion. Patients were treated in two centers, although both were high-volume units with similar clinical practices. Of note, patients with a different tumor extension were included, with locally advanced and metastatic stages. Thus, sensitivity analyses were performed exclusively in the metastatic population. Computed tomography-scan assessment of tumor response according to RECIST criteria was not performed centrally. This bias could explain a trend towards better tumor response in the FOLFIRINOX group. Additional variables, particularly febrile neutropenia, biological or HRQoL data, could not be evaluated in our study due to the retrospective design of the data collection, with a high rate of missing patient information.
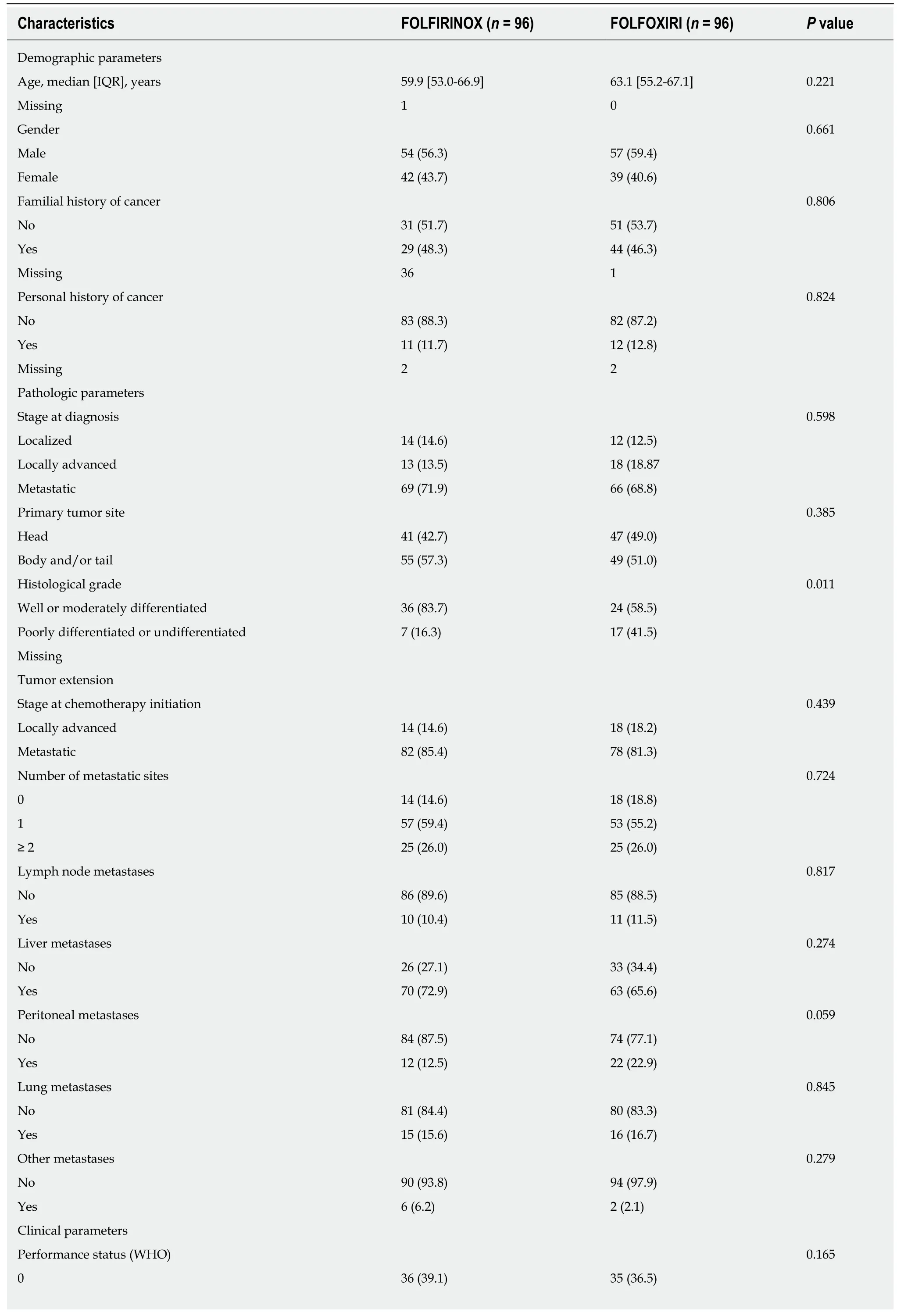
Table 3 Patient characteristics in the propensity score-matched population according to first-line chemotherapy, n (%)
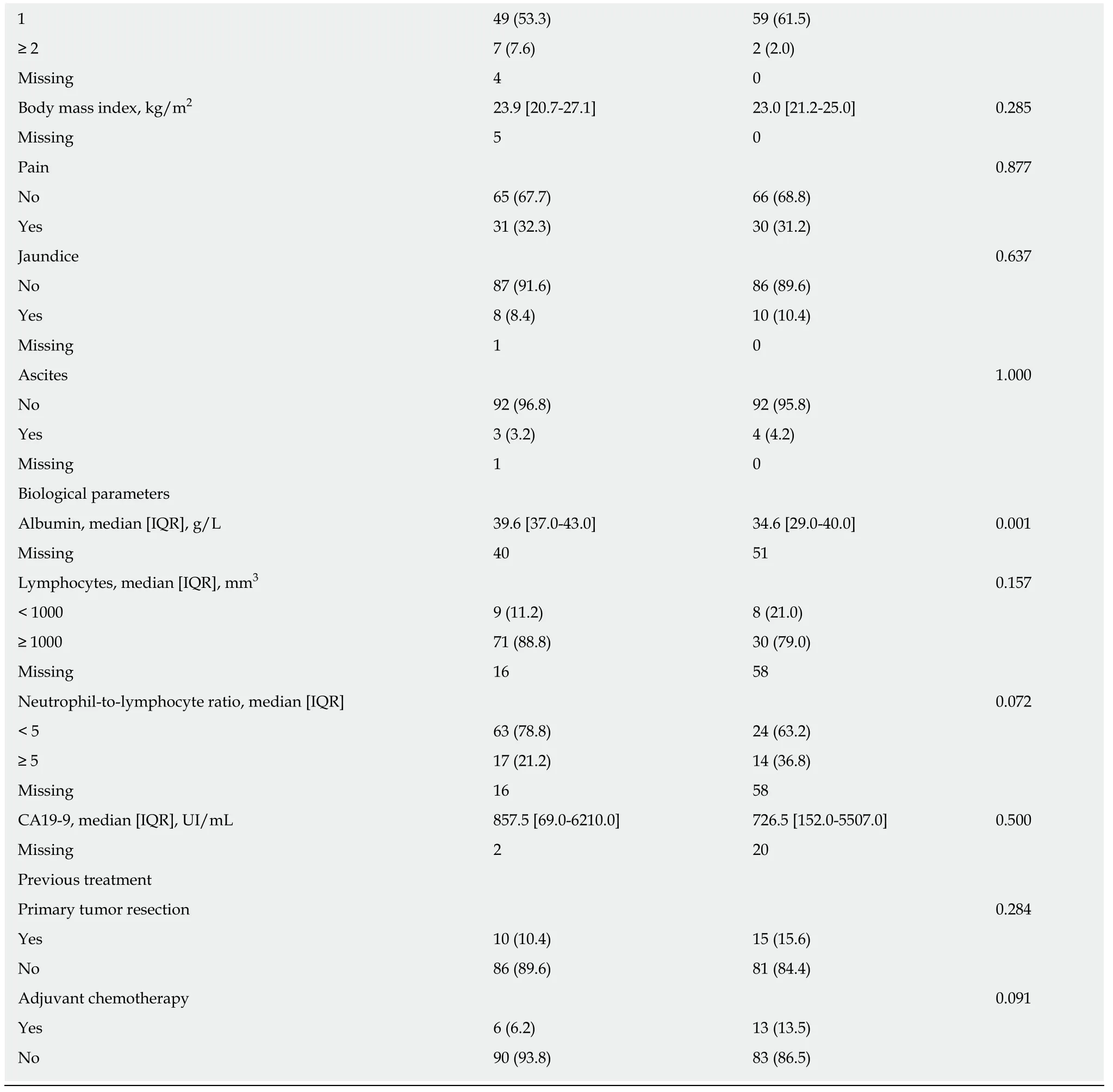
χ2 tests or Fisher’s exact tests were used to compare proportions, and Wilcoxon tests were used to compare continuous variables between the FOLFIRINOX and FOLFOXIRI groups. All statistical tests were two-sided. CA19-9: Carbohydrate Antigen 19-9; IQR: Interquartile range; WHO: World Health Organization.
To overcome these limitations, FOLFOXIRI and FOLFIRINOX were compared from a large population-based cohort of prospectively included patients with aPDAC. Most importantly, we used a rigorous methodological framework and applied a propensity score approach to take into account the potential heterogeneity in baseline characteristics between the two populations. Moreover, two different methods,namely the IPTW Cox model and propensity score matching, demonstrated the satisfactory performance and validity of the analysis. The reproducibility obtained with the sensitivity analysis in the metastatic cohort strengthened the observed results.
The present study showed that the FOLFOXIRI and FOLFIRINOX L1 regimens were similar in terms of efficacy. Median OS and PFS were comparable between the two schedules, and similar to survival rates reported by Conroyet al[7]in FOLFIRINOX-treated patients. The objective response rate with the FOLFOXIRI regimen observed in our cohort (37.1%) was similar to that reported in the GONO study in FOLFOXIRI-treated patients (38.6%)[21]. No differences in response rates between the FOLFOXIRI and FOLFIRINOX regimens in our unselected population were detected. Nevertheless, they were higher than those reported in the randomized phase III trial (31.6%)[7]. The methodological approach used in our study showed that FOLFOXIRI does not provide an improved efficacy compared to FOLFIRINOX.
The FOLFOXIRI regimen was associated with an increased risk of the occurrence of grade 3 or 4 digestive toxicities (12.8%), including diarrhea, nausea/vomiting, and stomatitis. Of note, this incidence was similar to the gastrointestinal safety profile reported by Vivaldiet al[21]with FOLFOXIRI chemotherapy. Interestingly,hematological toxicities were very low in both regimens in our study, compared to FOLFIRINOX in the PRODIGE 4/ACCORD 11 study[7]. A primary prophylactic administration of hematopoietic growth factors contributed to the reduction of grade 3 or 4 neutropenia[22,23], and thus, routine use after each polychemotherapy cycle has been adopted in some institutions.
Many combinations with “modified FOLFIRINOX” chemotherapy have been evaluated, and the schedules used to deliver this polychemotherapy are heterogeneous[24,25]. Dose reductions of single or multiple agents differ among studies compared to the standard schedule[24]. An optimal relative dose intensity for FOLFIRINOX was determined by Leeet al[23]to balance toxicity and efficacy,suggesting that a decrease of 30% in chemotherapy dosages preserve tumor response.In addition, two meta-analyses suggested that dosage attenuation improves tolerance while preserving survival benefits (overall response rates: 32% with “modified FOLFIRINOX”vs33% with full doses;P= 0.879)[24,25]. A modified-dose regimen decreased the frequency of hematological and digestive adverse events and cycles reported, while making it possible to maintain dose-dense chemotherapy and treatment activity[26]. In the adjuvant setting, a modified FOLFIRINOX with no bolus of 5-FU and irinotecan at a dose of 150 mg/m2significantly increased survival compared to gemcitabine for PDAC[4]. These dose adjustments were also effective in the neoadjuvant setting for patients with locally advanced or borderline PDAC. Of note, resection was performed in more than half of the patients, and with R0 resection in 86.4% of cases[27].
In previous retrospective and single-arm phase II studies, the bolus of 5-FU was more frequently discontinued in the “modified FOLFIRINOX” combination[10,28-31].Infusion of 5-FU is preferred for the treatment of colorectal cancer over bolus 5-FU. In this setting, the omission of the bolus of 5-FU has been shown to improve the safety profile, while significantly decreasing hematological toxicity[32]. A dose reduction of irinotecan (130-135 mg/m2, 150 mg/m2, or 165 mg/m2) was evaluated in previous studies[28-31,33-35]. The addition of irinotecan in FOLFOXIRI chemotherapy increased digestive toxicity occurrence, notably nausea/vomiting and diarrhea, compared to the doublet-chemotherapy (FOLFOX) in metastatic colorectal cancer[36]. In aPDAC, a 25%reduction of irinotecan compared to full dose has been associated with a decrease in diarrhea (3.1%vs12.5%, respectively) and vomiting (0%vs23.5%, respectively)[35].
Dihydropyrimidine dehydrogenase and uridine diphosphate glucuronosyltransferase (UGT) 1A1 are two key enzymes involved in the catabolic pathways of 5-FU and irinotecan, respectively. Their deficiency related to genetic polymorphisms,leads to increased exposure to the cytotoxic agents with a higher risk of adverse events. Indeed, variants of UGT1A1 have been reported to increase the risk of grade 3 or 4 hematological toxicity and diarrhea[37,38]. A study that evaluated the FOLFIRINOX regimen in pancreatic cancer, reported a significantly higher incidence of diarrhea among patients with UGT1A1 heterozygous type (UGT1A1 −/*6 and UGT1A1 −/*28)compared to those with UGT1A1 wild-type (−/−). However, for patients who received the “modified FOLFIRINOX”, there was no observed difference in the frequency of adverse events due to UGT1A1 status[39]. Furthermore, studies have indicated an association between polymorphisms of the dihydropyrimidine dehydrogenase gene encoding (DPYD) and 5-FU-induced toxicity[40]. Currently, DPYD genotype or phenotype-based dose reduction improves the safety of patients receiving fluoropyrimidine treatment and is recommended[41,42]. Preemptive screening of DPYD and UGT1A1 variants could identify patients at risk of clinically relevant adverse events, to improve FOLFIRINOX administration[43]. In an era of personalized medicine, a “genotype-guided” approach could help to individualize the dose to optimize efficacy, limit toxicity and guarantee HRQoL.
In conclusion, FOLFOXIRI is feasible in L1 in patients with aPDAC, but does not appear to confer any therapeutic benefit as compared with the FOLFIRINOX regimen.FOLFOXIRI was associated with a higher incidence of grade 3 or 4 digestive adverse events compared to FOLFIRINOX. A major difference in hematological toxicities was observed between our cohort and the PRODIGE 4/ACCORD 11 trial[7], underlining the relevance of prophylactic administration of hematopoietic growth factors in routine clinical practice. These results show that additional evaluation is not warranted in future clinical trials. FOLFIRINOX chemotherapy remains the standard of care in L1 in metastatic PDAC.
ARTICLE HIGHLIGHTS
Research background
The FOLFIRINOX regimen is the first-line reference chemotherapy (L1) in advanced pancreatic ductal adenocarcinoma (PDAC). FOLFOXIRI might contribute to a better balance in the toxicity/efficacy ratio in this setting.
Research motivation
FOLFOXIRI has demonstrated efficacy and feasibility in colorectal cancer.
Research objectives
To investigate the potential clinical value of FOLFOXIRI in patients with advanced PDAC(aPDAC) in routine clinical practice.
Research methods
This exploratory study compared clinical outcomes between the two treatments in the overall population and after propensity score matching.
Research results
All consecutive aPDAC patients treated in L1 with FOLFOXIRI (n = 165) or FOLFIRINOX (n =124) regimens were included. Median overall survival was 11.1 mo in the FOLFOXIRI cohort and 11.6 mo in the FOLFIRINOX cohort. After propensity score matching, survival rates remained similar between the regimens in terms of overall survival and progression-free survival.FOLFOXIRI was associated with a higher incidence of grade 3/4 digestive adverse events. The low hematological toxicity rates in both regimens underline the relevance of primary prophylaxis with hematopoietic growth factors.
Research conclusions
FOLFOXIRI is feasible in L1 in patients with aPDAC but does not confer any therapeutic benefit as compared with FOLFIRINOX.
Research perspectives
These results suggest that further evaluation of FOLFOXIRI in future clinical trials is not warranted. FOLFIRINOX chemotherapy remains the standard of care in L1 in metastatic PDAC.
ACKNOWLEDGEMENTS
We thank Fiona Ecarnot for English writing assistance.
 World Journal of Gastrointestinal Oncology2020年3期
World Journal of Gastrointestinal Oncology2020年3期
- World Journal of Gastrointestinal Oncology的其它文章
- Utility of positron emission tomography-computed tomography scan in detecting residual hepatocellular carcinoma post treatment: Series of case reports
- Clinical outcomes of patients with duodenal adenocarcinoma and intestinal-type papilla of Vater adenocarcinoma
- Surgical intervention for malignant bowel obstruction caused by gastrointestinal malignancies
- Impact of preoperative chemoradiotherapy using concurrent S-1 and CPT-11 on long-term clinical outcomes in locally advanced rectal cancer
- Circulating cytokines and outcome in metastatic colorectal cancer patients treated with regorafenib
- Association between interleukin-21 gene rs907715 polymorphism and gastric precancerous lesions in a Chinese population