
Anomalous retinal artery associated with branch retinal artery occlusion and neovascular glaucoma:A case report
2020-04-25 02:38:52WanJuYangYanNingYangMingGaoCaiYiQiaoXing
World Journal of Clinical Cases 2020年6期
Wan-Ju Yang,Yan-Ning Yang,Ming-Gao Cai,Yi-Qiao Xing
Abstract
Key words: Branch retinal artery occlusion; Vascular abnormality; Case report
INTRODUCTION
Anomalous retinal artery takes various forms,of which a cilioretinal artery is the most common.Other forms,including anomalous course,prepapillary loop,aberrant macular artery,and trifurcation,are unusual[1].Most patients with retinal artery anomalies are healthy with normal vision[1,2].However,in rare cases,a congenital anomalous retinal artery has been reported to be associated with macro-aneurysmal rupture[3],central retinal vein occlusion[4],and/or transient vertical monocular hemianopsia[5].
Branch retinal artery occlusion (BRAO) is a rare condition that accounts for 38% of all cases of acute retinal artery occlusion[6].No treatment for BRAO has been clinically proven to be effective.Risk factors for this condition include systemic hypertension,diabetes mellitus,coronary heart disease,stroke,smoking,and obesity[6].
To the best of our knowledge,the association of anomalous retinal artery with BRAO has not previously been reported.In this article,we report a rare case of congenital anomalous retinal artery in which a large retinal artery branch with an abnormal course was associated with BRAO,leading to macular edema and severe loss of vision.The patient eventually developed neovascular glaucoma (NVG) in the affected eye.The clinical timeline is presented in Figure 1.
CASE PRESENTATION
Chief complaints
A 52-year-old male visited our clinic in June 2009 with reduced vision in the right eye for the past 8 d.
History of present illness
No relevant ocular or medical history.
蜘蛛精很快来到了巨石前,并不稍停,抬起节足直接踩了上去。那巨石高有两米,它一步而上,轻松如履平地。青辰蜷身在一处凸出石体的下方,但那只能遮住他的半截身子,他的腿脚和头脸都露在外面。他用手臂护着头脸,稍稍露出眼睛朝上望着。蜘蛛精离他很近,他发现,对方的身体,并非是一般蜘蛛那种细腰宽肚,而是一个人形,比成年人小着一些,四肢俱全。它浑身裹在漆黑的硬甲中,位于八只节足的中间,在节足的支撑下悬空斜倾,仿似飘着一般。
History of past illness
The patient reported no history of systemic hypertension,diabetes mellitus,coronary heart disease,stroke,smoking,or obesity.
Personal and family history
None.
Physical examination upon admission
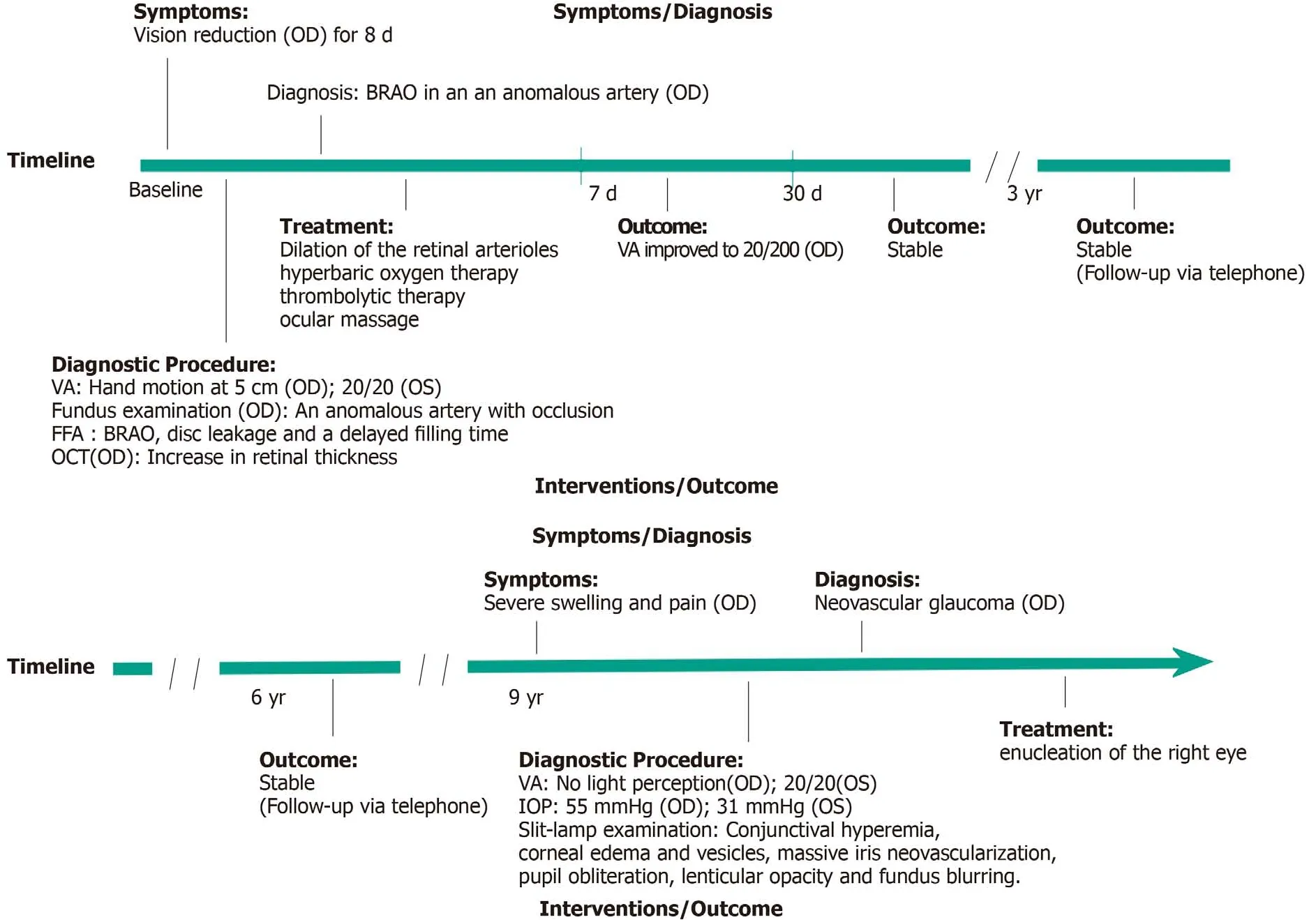
Figure 1 Clinical timeline.
His visual acuity was hand motion at 5 cm OD and 20/20 OS compared to 20/20 OD and 20/20 OS 8 d earlier.Examination revealed normal findings in the anterior segment and intraocular pressures (IOPs) that were within normal limits in both eyes.
Laboratory examinations
Laboratory examination revealed fasting blood glucose of 4.67 mmol/L,triglyceride of 0.65 mmol/L,total cholesterol of 4.38 mmol/L,erythrocyte sedimentation rate of 6.00 mm/h,and various decreases in whole blood viscosity at low-shear rate,medium-shear rate,and high-shear rate.
Imaging examinations
The fundus examination revealed an anomalous artery that extended from the superior temporal arcade,and then crossed the macula into the inferior temporal quadrant.The anomalous artery was partially occluded,with a narrowed lumen.A cherry-red spot and adjacent cloudy whitening indicated an edematous macula(Figure 2).The patient’s pupillary light reflex showed prolonged latency.Carotid ultrasound Doppler suggested mild stenosis of the right vertebro-basilar artery.Fundus fluorescein angiography confirmed involvement of the anomalous inferior temporal artery branch in the BRAO,disc leakage,and a delayed filling time in the right eye (Figure 3A-H).Optical coherence tomography was performed to evaluate these lesions.The results showed increased thickness of the neuroretina and underlying layers (Figure 3I and J).
FINAL DIAGNOSIS
Anomalous retinal artery associated with BRAO.
TREATMENT
The patient was treated with dilation of the retinal arterioles,hyperbaric oxygen therapy,and thrombolytic therapy,in combination with ocular massage.At 1 wk later,visual acuity of the right eye had improved to 20/200.
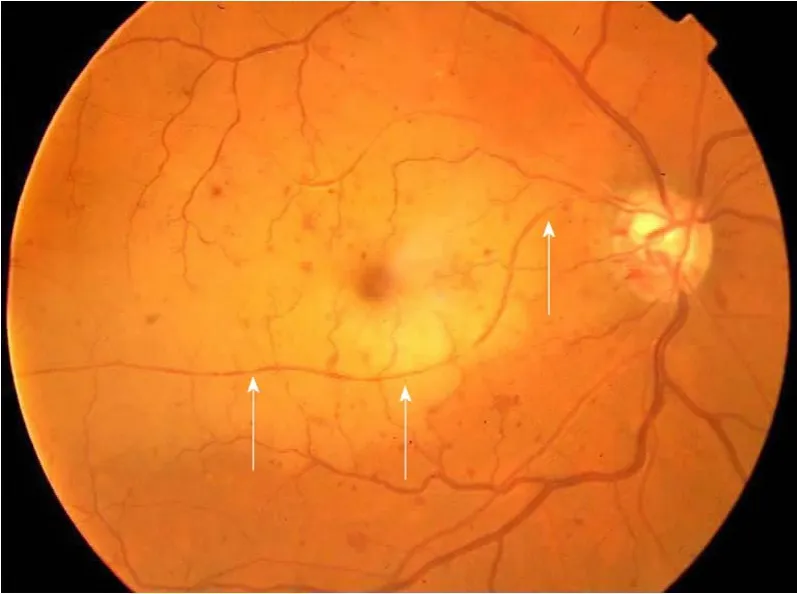
Figure 2 Color fundus image of the right eye at presentation showing an anomalous artery originating from the superior temporal arcade and crossing the macula into the inferior temporal retinal quadrant.
OUTCOME AND FOLLOW-UP
Examination at the 1-mo follow-up visit revealed that this improvement had remained stable.Two subsequent follow-up interviews,conductedviatelephone 3 and 6 years later,indicated that visual acuity in the right eye remained unchanged.
At 9 years after initial presentation at our institution (February 2018),the patient was admitted to a local hospital (Yingshan County People’s Hospital,Hubei Province)due to severe swelling and pain in the right eye.Ophthalmic examinations showed that the right eye had no light perception.The left eye’s visual acuity was 20/20.IOP was 55 mmHg in the right eye and 31 mmHg in the left eye.The right eye also showed evidence of conjunctival hyperemia,corneal edema and vesicles,massive iris neovascularization,pupil obliteration,lenticular opacity,and fundus blurring.Based on these findings,the right eye was diagnosed with NVG.The patient subsequently underwent enucleation of the right eye at a local hospital.
DISCUSSION
We reported an extremely rare case of retinal vascular anomaly in combination with BRAO that led to severe loss of vision of the affected eye.In this case,as is typical for a congenital retinal macrovessel (CRM),a large artery branch originated at the superior temporal arcade,then crossed the horizontal raphe to travel through the macular area.As a form of retinal vascular anomaly,CRM is typically unilateral and rarely affects vision in the affected eye[1,2].However,the patient may lose vision in the affected eye if the CRM is complicated with a foveal cyst,macular hemorrhage,serous macular detachment,BRAO,or other vascular abnormality[2].Although CRM typically affect veins[1,2],in this case,the CRM stemmed from an artery.
Although CRMs are typically associated with normal visual acuity,in this case,BRAO of the anomalous retinal artery resulted in dramatically reduced visual acuity(hand motion at 4 cm) at the time of presentation.To the best of our knowledge,this is the first report on an anomalous retinal artery involved in a BRAO.In a similar case previously reported by Goelet al[7],the BRAO was associated with an anomalous retinal vein.
BRAO is not common and may result in a sudden,painless loss of vision.Although the pathogenesis of the BRAO was not determined in this case,the risk factors for BRAO include systemic hypertension,diabetes mellitus,coronary heart disease,stroke,and smoking[8].However,our patient denied all of these factors.
In this case,the superior temporal artery branch took an abnormal course,supplying blood to the inferior temporal,rather than superior temporal,retina.A large survey of anatomical variation,undertaken by Awan[1]included eyes from 2100 people.The inferior temporal retina was supplied by a large branch from the superior temporal artery in 11 eyes,as in the case presented above.The author also reported that the superior temporal retina was supplied by the inferior temporal artery in eight eyes.In such patients,occlusion of the involved artery results in “paradoxical field defects.” Importantly,all patients examined by Awan[1]had normally functioning eyes,despite the abnormal course of the involved artery branches.

Figure 3 Fundus fluorescein angiography and optical coherence tomography images for the right eye.
In our case,the eye with an anomalous retinal artery eventually developed NVG with complete loss of vision.It has been reported that NVG may result from BRAO[9,10].Yamamotoet al[9]reported a case of NVG in combination with recurrence of a BRAO 5 wk after a 72-year-old man was initially diagnosed with BRAO.In our case,the NVG appeared 9 years after the initial BRAO.Although the cause of NVG in our case was not determined,we speculate that the NVG may have been associated with a recurrence of the BRAO.
CONCLUSION
Congenital anomalous retinal artery generally does not affect the vision of a patient.However,an abnormal artery that passes through and supplies blood to the macular area may negatively impact visual acuity when complicated with BRAO.
猜你喜欢
科教新报(2022年17期)2022-05-24 04:34:52
祝您健康(2020年9期)2020-09-08 06:21:54
意林(2018年17期)2018-09-30 02:42:48
琴童(2018年2期)2018-03-06 16:36:52
学苑创造·A版(2017年8期)2017-06-24 18:06:48
故事作文·低年级(2017年3期)2017-04-04 20:49:46
中学生阅读(初中版)(2016年7期)2017-02-24 09:36:52
电子制作(2016年15期)2017-01-15 13:39:11
故事作文·低年级(2016年1期)2016-09-10 07:22:44
作文评点报·作文素材小学版(2014年45期)2014-11-25 21:34:07
 World Journal of Clinical Cases2020年6期
World Journal of Clinical Cases2020年6期
- World Journal of Clinical Cases的其它文章
- Late-onset multiple acyl-CoA dehydrogenase deficiency with cardiac syncope:A case report
- Misdiagnosis of primary intimal sarcoma of the pulmonary artery as chronic pulmonary embolism:A case report
- Two bone blocks sandwich technique for horizontal reconstruction of severely atrophic alveolar ridge in anterior maxilla:A case report
- Muscular involvement of extranodal natural killer/T cell lymphoma misdiagnosed as polymyositis:A case report and review of literature
- Total endovascular repair of an intraoperative stent-graft deployed in the false lumen of Stanford type A aortic dissection:A case report
- Extrapontine myelinolysis caused by rapid correction of pituitrin-induced severe hyponatremia:A case report