
Calcitonin-negative neuroendocrine tumor of the thyroid with metastasis to liver-rare presentation of an unusual tumor:A case report and review of literature
2020-04-22 07:13HuaiJieCaiHanWangNanCaoBinHuangFanLeiKongLiRenLuYaYuanHuangWeiWang
World Journal of Clinical Cases 2020年1期
Huai-Jie Cai,Han Wang,Nan Cao,Bin Huang,Fan-Lei Kong,Li-Ren Lu,Ya-Yuan Huang,Wei Wang
Huai-Jie Cai,Han Wang,Nan Cao,Bin Huang,The Fourth Clinical Medicine College,Zhejiang Chinese Medical University,Hangzhou 310053,Zhejiang Province,China
Fan-Lei Kong,Li-Ren Lu,Ya-Yuan Huang,Wei Wang,Department of Ultrasound,Affiliated Hangzhou First People's Hospital,Zhejiang University School of Medicine,Hangzhou 310006,Zhejiang Province,China
Abstract
Key words: Thyroid;Neuroendocrine tumor;Hepatic metastases;Diagnosis;Treatment;Case report
INTRODUCTION
Medullary thyroid carcinoma (MTC) is one of the most common neuroendocrine tumors (NETs) of the thyroid with an incidence of 1%-2% according to the revised guidelines for the treatment of MTC issued by the American Thyroid Association[1].In general,calcitonin is produced by thyroid parafollicular cells and its elevation in serum is the main criterion for clinical diagnosis of MTC.Calcitonin is additionally an important indicator for prognosis of the disease[2,3].
Clinical diagnosis of calcitonin-negative neuroendocrine tumors of the thyroid(CNNET) is confusing[4].Owing to the extreme rarity of these cases,standardized management protocols are yet to be formulated.Prognosis of CNNET is poorer than that of other thyroid tumors.CNNET features on ultrasound are indistinguishable from those of papillary thyroid carcinoma,and diagnosis is mainly dependent on pathological findings.In cases where morphological identification is difficult,positivity of TTF-1,CgA,Syn,Ki-67,and other specific markers may aid in further diagnosis.
In terms of treatment and prognosis,surgical resection of the thyroid gland is the preferred option,while transcatheter arterial chemoembolization (TACE) has limited efficacy for liver metastasis.In this study,the ultrasonic features and immunohistochemical characteristics of CNNET with liver metastases have been investigated in detail.Furthermore,comparative analysis of the current case with previous reports of CNNET has provided a deeper understanding of the underlying factors and integration of case information with the objective of facilitating standardization of diagnosis and effective disease management.
CASE PRESENTATION
Chief complaints
On October 29,2018,a 56-year-old female patient was admitted to our hospital due to goiter and pain for over a month.
History of past illness
Radical resection of rectal carcinoma 1 year earlier.
Personal and family history
The family history was unremarkable.
Physical examination upon admission
Normalities were noted on physical examination with the exception of slight goiter with pain,and multiple enlarged lymph nodes were detected in the bilateral neck.
Laboratory examinations
Normalities were detected in laboratory tests,including calcitonin and CEA levels and thyroid and parathyroid function.
Imaging examinations
Ultrasound examination revealed that the thyroid gland was full and irregular in shape,and the envelope was not smooth.Multiple nodules were detected in bilateral lobes;the larger about 2.6 cm × 2.1 cm × 1.7 cm in size located in the right thyroid.The internal echo was uneven.Color Doppler flow imaging indicated abundant blood supply.Multiple enlarged lymph nodes were detected in the bilateral neck;the largest about 4.2 cm × 2.6 cm × 2.0 cm in size located on the right side (Figure 1).
Routine blood parameters,coagulation function,thyroid function,parathyroid function,calcitonin,and tumor indices were within the normal range.Pathological diagnosis of whole tissue disclosed that the thyroid gland was beam-shaped with significant cell atypia,thick and granular nuclear chromatin,obvious karyokinesis,and patchy necrosis.Immunohistochemical analyses showed calcitonin-,TG-,CEA-,PAX-8-,TTF-1+,CgA+,Syn+,and Ki-67+,suggestive of CNNET with cervical lymph node metastasis (Figure 2).
After 2 mo,the patient was readmitted due to dull upper abdominal pain.Ultrasound findings suggested an equal echo nodule in the left liver (S2) measuring 1.9 cm × 1.8 cm.The boundary was clear with a surrounding sound halo similar to the bull's eye sign.Contrast-enhanced ultrasonography (CEUS) showed that the mass was enhanced rapidly after 13 s,reached a peak in 17 s,and showed a "fast in and fast out" performance pattern,compared with normal liver parenchyma (Figure 3A-C).In magnetic resonance images (MRI),we observed low T1 signal mass and high T2 and DWI signal mass,with a ring-shaped edge of enhancement.
Based on the combined medical history and imaging findings,metastasis was suspected.Biopsy findings confirmed neurosecretory liver metastasis.After TACE,review of computed tomography (CT) findings showed iodized oil perfusion of the entire mass (Figure 3D).MRI performed 3 mo later revealed no significant reduction in the previous mass and multiple new metastases in the liver;the largest of which was 1.0 cm × 0.7 cm in size (Figure 4).
FINAL DIAGNOSIS
Calcitonin-negative neuroendocrine tumor of the thyroid with metastasis to liver.
TREATMENT
According to the 2015 American Thyroid Association management guidelines,the patient had puncture indications,and fine needle biopsy was performed on the right lobe nodules and right lymph nodes.The results suggested that right nodules were suspicious for tumor cells and right lymph nodes should be considered for metastasis.Consequently,complete thyroidectomy was performed after exclusion of contraindication,followed by clearance of lymphoid and adipose tissue of bilateral neck in areas II,III,IV,and V.Intraoperatively,bilateral nodules with a hard texture and unclear boundary occupied almost the entire thyroid gland.Bilateral neck exploration revealed multiple enlarged lymph nodes of hard texture,although the boundary remained clear.Two months after operation,TACE treatment was elected to control metastatic tumor growth of the left liver (S2) after consultation with the patient.The tumor blood supply artery was injected with epirubicin (20 mg) and cisplatin (60 mg) through a microcatheter,followed by 5 mL super-liquefied lipiodol suspension,and the puncture site pressurized after the operation.
OUTCOME AND FOLLOW-UP
MRI performed 3 mo later revealed no significant reduction in the previous mass and multiple new metastases in the liver,and the patient was referred to a specialist hospital to seek treatment.
DISCUSSION
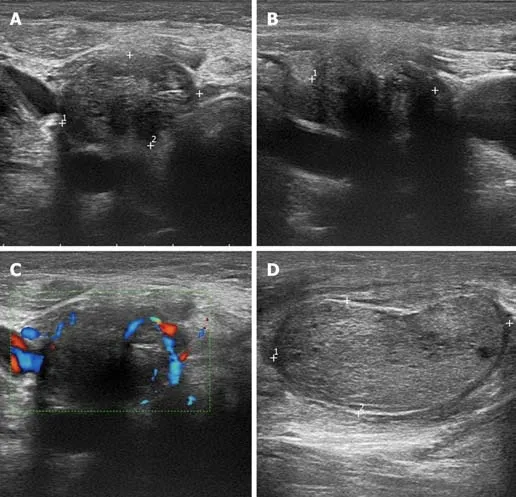
Figure1 Ultrasound images of calcitonin-negative neuroendocrine tumor with cervical lymph node metastases.
MTC is a rare thyroid NET with clinical features mainly characterized by proliferation of thyroid parafollicular cells with substantial levels of peptide hormones and calcitonin,which facilitate its differentiation from other thyroid tumors.Mutation of the RET proto-oncogene on chromosome 10 is the main underlying cause of pathogenesis in MTC[5].CNNET is an even rarer condition,with only 17 cases documented in PubMed and no identified pathogenic factors.Early CNNET generally has no clinical symptoms,and its presence is difficult to detect until the tumor is further enlarged or accompanied by lymph node metastases.
Because the current case had a history of rectal cancer,we should also consider the possibility of rectal cancer origin.While the likelihood is low,rectal cancer metastasis to the thyroid gland has been documented[6].Diagnosis of CNNET mainly relies on the presence of pathological immunomarkers,such as CgA,Syn,CEA,and TTF-1.In particular,TTF-1 is a transcription factor that primarily regulates expression of thyroid-specific genes,including thyroglobulin and thyroid peroxidase,which may be highly suggestive of tumor origin in the thyroid gland and often detected in MTC or CNNET[7].
CNNET has no specific manifestations in imaging and is difficult to distinguish from other tumors.Discrimination from a number of diseases is required for confirmation of diagnosis.One is thyroid paraganglioma,a rare primary NET of the thyroid gland.Histologically,this tumor presents as a solid nest,organ-like structure,with no expression of calcitonin and TTF-1,distinct from CNNETs.The value of malignant small cell tumors in differential diagnosis has also been demonstrated.Poorly differentiated small-cell medullary carcinoma with low amyloid load is similar in cell size to small cell carcinoma,malignant lymphoma,Ewing sarcoma,and smallcell malignant melanoma.However,these tumors have unique morphological characteristics,and immunohistochemistry is helpful for differentiation.The third tumor type is metastasis of lung origin.TTF-1 is expressed not only in normal thyroid C cells,follicular epithelial cells,and tumors formed by these cells but also in lung adenocarcinoma.However,cells of lung adenocarcinoma are more heterogeneous and may have adenoid structure or glandular cavity.Combined pulmonary CT and histological analyses may be applied to exclude this tumor type[7].The characteristics of CNNET based on earlier literature are summarized in Table 1[8-22].

Figure2 Thyroid pathology and immunohistochemistry.
The 17 cases reported to date include 10 males and 7 females aged 16-76 years(mean age:51 ± 16 years) with tumor sizes of 0.6-15 cm (average size:4.0 ± 3.4 cm).Expression of CgA and Syn was detected in almost all cases.TTF-1,a specific marker of thyroid follicular cells,has a high positive rate in common benign and malignant thyroid lesions and is specifically expressed in the nucleus.TTF-1 results were collected in 9 cases,among which 3 cases were negative,and 6 were positive.Expression of TTF-1 was not significantly correlated with patient age or tumor size.TG,the main glycoprotein produced by the thyroid gland,is generally used as a template for thyroid hormone synthesis and storage of thyroid iodine.Differentiated thyroid carcinoma is often positive for TG.As shown in Table 1,TG data were obtained in 6 cases (2 negative and 4 positive).Further studies on a larger number of cases are required to ascertain whether TG is specific for CNNET.Owing to the lack of unique pathological characteristics,no distinctive prognostic biomarkers have been identified.Lymph node metastasis occurred in two of the cases,one of which was peritoneal metastasis with a higher degree of malignancy.The primary thyroid mass had a diameter of 15 cm.The lower boundary reached the hilar level,with Ki increment index reaching 70%.The tumor rapidly metastasized and could only be controlled by palliative chemotherapy.The mean survival rate of CNNET has not been determined due to limited information.

Figure3 Ultrasound and computed tomography images of liver metastases.
For smaller CNNETs,surgery is the preferred treatment of choice.According to previous reports,surgical treatment achieved good results.However,in this case,liver metastasis was detected 2 mo after surgery.Because the patient had a history of radical rectal cancer surgery a year earlier,it was necessary to exclude the possibility of rectal cancer origin.Metastases from rectal cancer usually present as well-defined hyperechoic nodules,some of which may calcify with acoustic shadows in the rear.In this case,the ultrasound was isoechoic and CEUS characterized as "fast in,fast out,high overall enhancement",similar to the performance of pancreatic NET reported by Takadaet al[23].The imaging findings were additionally more consistent with those of NET origin.The liver mass was punctured,and the thyroid confirmed as the tumor sourceviapathology.
The rapid development of CEUS in recent years has provided significant advantages in diagnosis of tumors with a rich blood supply.Ishikawaet al[24]reported 87.8% accuracy,85.0% specificity,and 90.5% sensitivity of ultrasound for NET.Kitanoet al[25]further assessed the sensitivity (78.9%) and specificity (98.7%) of contrastenhanced ultrasound in diagnosis of NET with a rich blood supply.Experiments by Palazzoet al[26]indicated that multimodal ultrasound can be effectively applied to evaluate the texture of NET and predict invasiveness of tumors with high specificity(82%),accuracy (86%),sensitivity (96%),positive predictive value (71%),and negative predictive value (98%).Moreover,Takadaet al[23]showed that CEUS and timeintensity curve could effectively aid in pathological classification of NET.However,metastasis of CNNET to the liver has not been reported until now,and no unified standards exist for CEUS characteristics of CNNET,which requires further investigation.
Liver metastasis could be attributed to three potential factors.First,preoperative CNNET had metastasized when the mass was small and could not be detected using ultrasound.Second,surgical excision led to hemorrhagic metastasis.Third,the degree of malignancy itself was higher.The third option was the most feasible because the CNNET blood supply in this case was extremely rich,and Ki increment index was 20%.In a study by Grozinsky-Glasberget al[27],single treatment of eight cases of MTC metastatic tumors to the liver with TACE achieved a degree of therapeutic efficacy.However,in the current case,the mass did not shrink significantly after TACE,and several new lesions were detected.According to the guidelines of the American Association for the Study of Liver Diseases[28],efficacy evaluation for this patient was assessed as progressive disease,confirmed by the high degree of malignancy.
For CNNET,poor prognostic factors include distant or lymph node metastasis,infiltration of the capsule,advanced age,and significant elevation of Ki.Based on the limited existing knowledge,it is difficult to prevent its occurrence,and early stages often develop with no symptoms,presenting a significant challenge for clinicians.Some MTCs do not secrete calcitonin at the early stage,which may be related to low secretory behavior of the tumor.Therefore,regular review of calcitonin and CEA levels after CNNET surgery is necessary.Follow-up thyroid ultrasound,lung CT,abdominal MRI,and other examinations are critical to improve patient prognosis.Fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography may be used as an effective complementary method to detect smaller tumors.
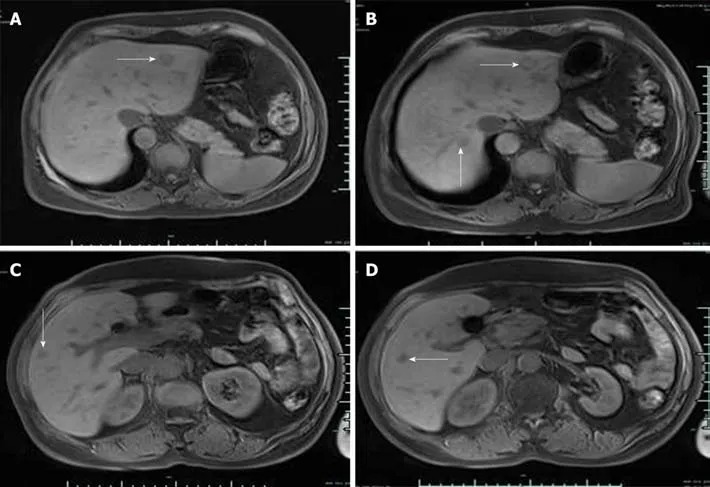
Figure4 Magnetic resonance images of liver metastases.
CONCLUSION
In conclusion,our understanding of the etiology and pathogenesis of CNNET is limited owing to the rarity of the disease.Further information on clinical progression and accumulating experience of the disease is essential to improve therapeutic outcomes.
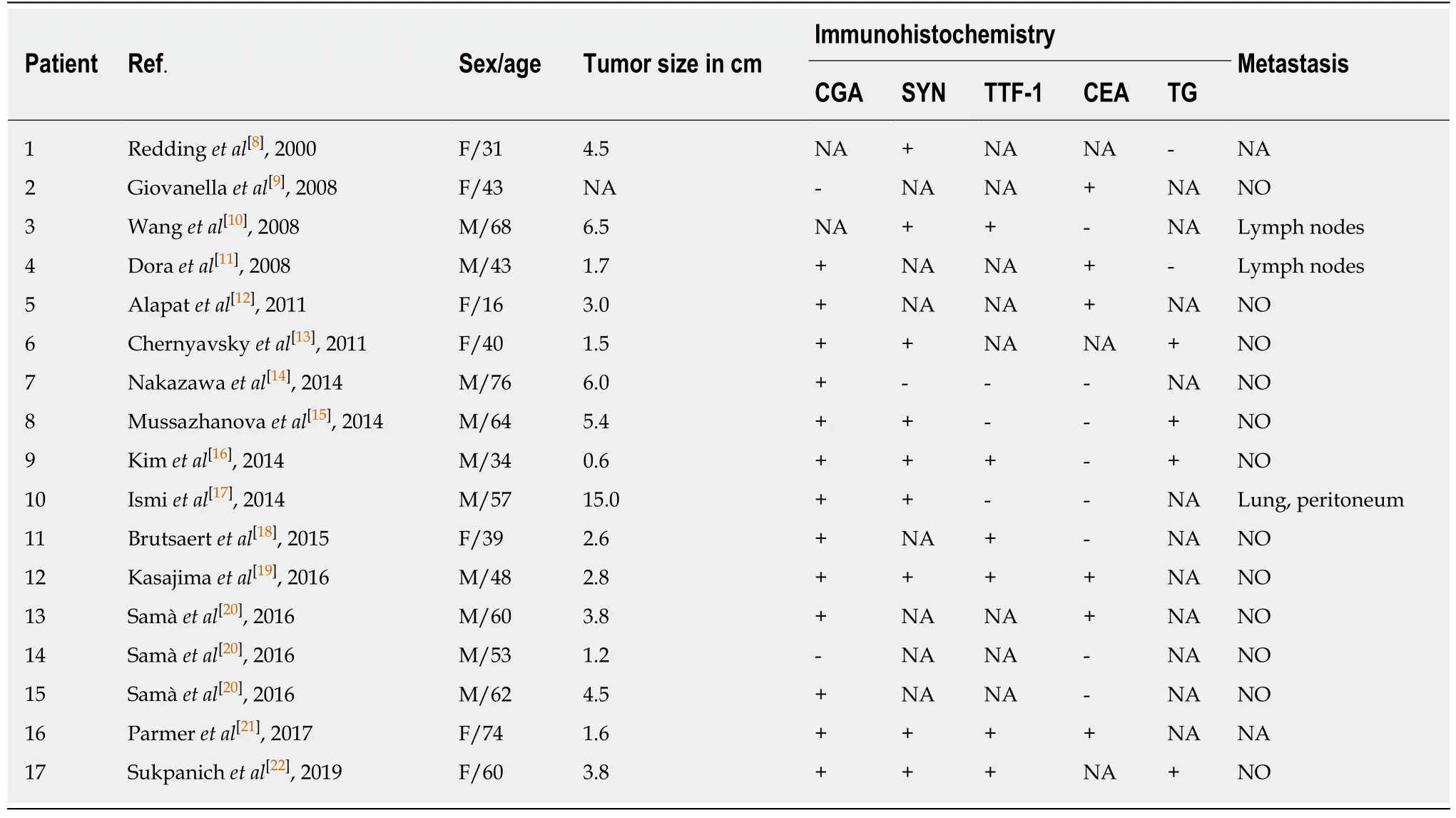
Table1 Characteristics of calcitonin-negative neuroendocrine tumors of the thyroid
 World Journal of Clinical Cases2020年1期
World Journal of Clinical Cases2020年1期
- World Journal of Clinical Cases的其它文章
- Role of oxysterol-binding protein-related proteins in malignant human tumours
- Oncogenic role of Tc17 cells in cervical cancer development
- Acute distal common bile duct angle is risk factor for postendoscopic retrograde cholangiopancreatography pancreatitis in beginner endoscopist
- Three-dimensional computed tomography mapping of posterior malleolar fractures
- Application of a modified surgical position in anterior approach for total cervical artificial disc replacement
- Potential role of the compound Eucommia bone tonic granules in patients with osteoarthritis and osteonecrosis:A retrospective study