
Hyalinizing clear cell carcinoma-a rare entity in the oral cavity:A case report
2020-04-22 07:13AlejandroDonohueCornejoOsleiPaesdeAlmeidaCelestenchezRomeroLeFranciscoEspinosaCristbalSimYobannyReyespezJuanCarlosCuevasGonzlez
World Journal of Clinical Cases 2020年1期
Alejandro Donohue-Cornejo,Oslei Paes de Almeida,Celeste Sánchez-Romero,León Francisco Espinosa-Cristóbal,Simón Yobanny Reyes-López,Juan Carlos Cuevas-González
Alejandro Donohue-Cornejo,León Francisco Espinosa-Cristóbal,Simón Yobanny Reyes-López,Juan Carlos Cuevas-González,Stomatology Department,Biomedical Sciences Institute,Autonomous University of Ciudad Juárez,Chihuahua 32310,México
Oslei Paes de Almeida,Celeste Sánchez-Romero,Diagnosis Department,Oral Pathology Section,Dentistry Faculty of Piracicaba,State University of Campinas,São Paulo 13414-903,Brazil
Abstract
Key words: Hyalinizing clear cell carcinoma;Salivary gland tumor;Immunohistochemical reactions;Case report
INTRODUCTION
Hyalinizing clear cell carcinoma (HCCC) is a rare tumor that originates in the salivary glands.Although this neoplasia constitutes less than 1% of minor salivary gland tumors,when this carcinoma presents,it has a predilection to develop in this type of gland.Due to its rarity,it has not been studied extensively.To this end,we present this case report,the clinical,histopathological,and immunohistochemical documentation of which can be useful for the clinician and pathologist when making the diagnosis,increasing our understanding and recognition of this carcinoma[1,2].
CASE PRESENTATION
Chief complaints
A 67-year-old female visited the maxillofacial surgery department due to a smooth,slightly yellowish protruding mass on the left side of the floor of the mouth,at the level of the molars (Figure 1A).
History of present illness
The tumor mass had a soft consistency on palpation and did not adhere to deep planes.The patient reported having noticed an increase in the volume of the mass for approximately 1 year asymptomatically.
Pathological findings
Based on the clinical features,the surgeon chose to perform an excisional biopsy.The tumor was well-demarcated from the surrounding tissues therefore,it was completely removed,measuring 5 cm × 4 cm × 4 cm (Figure 1B),and once the sample was processed and stained with hematoxylin and eosin (HE),a tumor lesion was observed,composed primarily of diffuse,proliferating clear cells that formed compact groups and cords that were separated by thick eosinophilic bands of collagen,with the appearance of hyaline (Figure 2A and B).Despite the predominance of clear cells,focal groups of tumor cells with eosinophilic cytoplasm were identified (Figure 2D),occasional mitoses and neural invasion were observed (Figure 2C).
Periodic acid-Schiff (PAS) stains and immunohistochemical reactions were performed to confirm the diagnosis.HCCC is diastase sensitive due to the glycogen of the tumor cells,as showed by our case,it was negative for PAS with diastase (Figure 3A) and positive for PAS without diastase (Figure 3B).Antibodies against AE1-AE3,CK5,CK7,p63,and Ki-67 were positive.In contrast,there was no signal with CK14,CK19,or smooth muscle antibodies (SMAs) (Figures 3 and 4).
FINAL DIAGNOSIS
Considering the clinical,histopathological,histochemical,and immunohistochemical findings,a diagnosis of HCCC was reached.Once the diagnosis was established and the cell morphology was re-evaluated surgical borders with neoplastic cells were identified.

Figure1 Clinical and macroscopic aspects of the lesion.
TREATMENT
The patient underwent a second surgery,widen the margins,to ensure complete removal of the lesion.
OUTCOME AND FOLLOW-UP
Close long-term follow-up.
DISCUSSION
Several studies suggest that HCCC presents primarily as a painless lesion that most often affects females (2:1),between the sixth and seventh decades of life.It is considered a low-grade neoplasm that rarely recurs or metastasizes[3].
This case had clinical characteristics of a benign lesion with duration of a year,which was intact covering mucosa and well-demarcated from the surrounding tissues.When the computerized axial tomography was performed,a small isodense exophytic mass was described on the floor of the mouth,close to the left molar area without growth towards the deep planes.According to our research,this is the second case of HCCC located on the floor of the mouth (Table 1),the patient did not seek consultation until the volume increase was considerable.
Due to the clinical characteristics,such as its well-defined increase in volume,its similarity in color to the adjacent mucosa,and its asymptomatic nature and evolution,our clinical impression was that of a benign neoplasm.However,following the standard protocol of care,a biopsy was performed by histopathology and complementary approaches,which allowed us to reach a definitive diagnosis of HCCC.
Overall,81.8% of cases of HCCC occur in the buccal cavity.The most frequent sites are the tongue,hard palate,floor of the mouth,and base of the tongue;HCCC is uncommon in the major salivary glands,nasopharynx,hypopharynx,and lacrimal gland[4].In a review of the literature that we conducted in cases from 2011 to date,we found 13 published clinical cases located in oral cavity of which 8 (61%) affected the female sex and 5 (39%) the male (Table 1).
Histopathologically,HCCC comprises proliferating epithelial cells with a clear cytoplasm.In some cases,a subgroup of cells with eosinophilic cytoplasm are present,all of which are organized in trabeculae,cords,or solid nests that are surrounded by a stroma of hyaline fibrous tissue.This tumor usually presents with immunohistochemical positivity for p63,CK5,CK7,CK14,and CK19 and negative S-100,CK 14,SMA,and PAX8 expression,in addition to negativity for PAS with diastase,which favors a diagnosis of HCCC and helps rule out other histopathological differential diagnoses,such as malignant myoepithelioma,epithelial-myoepithelial carcinoma,clear cell mucoepidermoid carcinoma,low-grade polymorphic adenocarcinoma,acinar cell carcinoma,clear cell oncocytoma,and renal metastatic carcinoma[5-9].Thus,an immunohistochemical panel with the appropriate antibodies must be performed.
In our case,we observed immunolabeling with antibodies against AE1-AE3,CK5,CK7,p63,and Ki67,whereas SMA,CK14,and CD10 were negative.Thus,we recommend using these immunohistochemical markers to aid in the diagnosis of this neoplasia with the histopathological characteristics that we have described.
HCCC is considered a low-grade malignancy.However,the size of the tumor,the cellular atypia,and the number of mitoses is related to its prognosis,and as with any other carcinoma,to decrease the likelihood of recurrence,it must be removed completely[10].In case series,up to 25% of evidence of metastasis has been reported[11].Although the treatment depends on the clinical characteristics of the tumor,in 50% of cases,it is limited to surgery,versus surgery and radiotherapy in 25.7%,with a 5-year survival of 77.6%;the remainder corresponds to other treatment modalities or is unknown to due to the unavailability of data[1].
In our case,by histopathology,we noted that the frequency of atypia and mitosis was low and that the positivity to Ki-67 antibody was of 3%,which was consistent with a low-grade malignant neoplasm.Although some tumor cells had infiltrated nervous tissue,the presence of metastases was ruled out by imaging (positron emission tomography).Because the edges of the excisional biopsy were not free of tumor cells,the patient underwent a second surgery to eliminate the possibility of recurrence.After 2 years of follow-up,there are no data that suggest recurrence,but continuous and long-term follow-up is indicated to identify any eventual alterations in a timely manner.
CONCLUSION
HCCC is a rare salivary gland tumor that has not been studied extensively.We presented herein the second case reported in the literature affecting the floor of the mouth.Its diagnosis is usually challenging,because clinically,it can be confused with a benign neoplasm,whereas histologically,there are several differential diagnoses.Thus,auxiliary techniques,such as PAS staining and immunohistochemistry,are valuable tools in reaching the correct diagnosis of this tumor.

Figure3 Negative tumor cells staining and histochemistry periodic acid-Schiff positive without diastase.
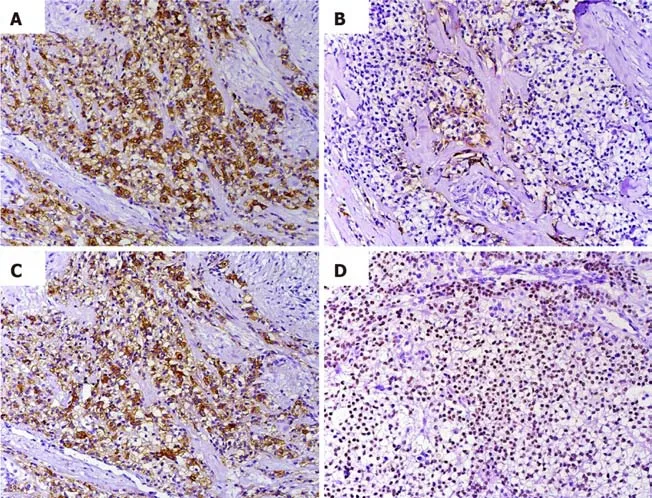
Figure4 Immunohistochemical profile of the tumor.
 World Journal of Clinical Cases2020年1期
World Journal of Clinical Cases2020年1期
- World Journal of Clinical Cases的其它文章
- Role of oxysterol-binding protein-related proteins in malignant human tumours
- Oncogenic role of Tc17 cells in cervical cancer development
- Acute distal common bile duct angle is risk factor for postendoscopic retrograde cholangiopancreatography pancreatitis in beginner endoscopist
- Three-dimensional computed tomography mapping of posterior malleolar fractures
- Application of a modified surgical position in anterior approach for total cervical artificial disc replacement
- Potential role of the compound Eucommia bone tonic granules in patients with osteoarthritis and osteonecrosis:A retrospective study