
A Meta-Analysis of Treating Radiation Proctitis by Retention Enema with Integrated Traditional Chinese and Western Medicine
2020-04-19 07:38:24LIUJiajia刘佳佳XUEMeiping薛美平WANGBoWANGXixing王晞星
LIU Jia-jia (刘佳佳), XUE Mei-ping (薛美平), WANG Bo (王 博), WANG Xi-xing (王晞星)
1. Graduate School, Shanxi University of Chinese Medicine, Taiyuan 030000, China
2. Oncology Department, Shanxi Traditional Chinese Medicine Hospital, Taiyuan 030000, China
3. Graduate School, Shanxi Medical University, Taiyuan 030000, China
ABSTRACT Objective:To systematically and objectively evaluate clinical efficacy of retention enema with integrated traditional Chinese and western medicine on radiation proctitis (RP). Methods:CNKI, WANFANG,VIP, CMB and foreign language databases like Embase, Central and Medline were searched. Search dates were from establishment of the databases until May 2020. Randomized controlled trials (RCTs) of retention enema with integrated traditional Chinese and western medicine for RP were retrieved. Two system reviewers selected literature materials, extracted literature data, and evaluated the quality of the literatures.RevMan 5.3 software was used for data analysis. Results:A total of 12 studies were included, including 941 patients. Meta-analysis results showed: Clinical efficacy in the retention enema group with integrated traditional Chinese and western medicine was better than that in the simple western medicine enema or blank enema group (OR=5.96, 95% CI [5.50, 14.29], P<0.000 01). Improvement of abdominal pain in the retention enema group with integrated traditional Chinese and western medicine was better than that in the control group (MD=-0.57, 95% CI [-0.72, -0.42], P<0.000 01). Treatment for hematochezia in the retention enema group with integrated traditional Chinese and western medicine was better than that in the control group (MD=-0.55, 95% CI [-0.69, -0.42], P<0.000 01). Improvement of diarrhea in the retention enema group with integrated traditional Chinese and western medicine was better than that in the control group(MD=-0.69, 95% CI [-0.91, -0.48], P<0.000 01). KPS scores in the retention enema group with integrated traditional Chinese and western medicine were better than those in the control group (MD=11.91, 95%CI [3.81, 20.01], P<0.000 01). Conclusion:Clinical efficacy of retention enema with integrated traditional Chinese and western medicine on RP is better than simple western medicine enema or blank enema. Due to the low quality of the included clinical literatures, it is necessary to carry out more deliberate, detailed,high-quality, randomized, double-blind, and multi-center RCTs in order to give more powerful demonstration on its clinical efficacy on RP.
KEYWORDS A Meta-analysis; Radiation proctitis; Integrated traditional Chinese and western medicine;Retention enema
Radiation proctitis (RP) is a rectal mucosal injury caused by radiotherapy for malignant pelvic tumors[1]. It clinically manifests as increased frequency of bowel movements, abdominal pain and discomfort, ungratifying diarrhea, a feeling of heavy sinking during defecation, blood-stained stools, etc.. It can even cause rectal stenosis,rectal ulcer, anorectal fistula, etc. Studies have shown that such adverse reactions can occur when the total amount of radiotherapy received by a patient reaches 30 Gy. If the total amount of radiation reaches 50-70 Gy, the incidence of adverse reactions will reach 70%[1]. For RP,western medicine mainly focus on symptomatic treatment such as anti-inflammation, antibiotics,probiotics, antioxidant antidiarrheal agents,somatostatin, etc.[2]. But it has disadvantages like easy to relapse, severe adverse reactions,not suitable for long-term use, and unsatisfactory clinical efficacy. Traditional Chinese medicine(TCM) include oral Chinese materia medica and preparations, Chinese materia medica enema, sitz bath, acupuncture and moxibustion etc. But there are also problems such as diverse prescriptions based on syndrome differentiation and inconsistent efficacy standards.Consensus on Diagnosis and Treatment for Radiation Proctitis(《放射性直肠炎(肠澼)诊疗共识》)[3]recommends that "anal dripping retention enema" is the best therapeutic plan for RP. Therefore, this study systematically evaluated clinical efficacy of retention enema on RP with integrated traditional Chinese and western medicine in order to provide reference for future clinical study and clinical application.
MATERIALS AND METHODS
Selection of Literatures
Inclusion criteria
① Study design methods: The trial design was in accordance with the clinical randomized controlled method. Any mention of "random entry"in the literature, regardless of whether blinding and allocation concealment were mentioned or not, it was included. ② Study objects: RP patients. Age,gender, region and race were not limited. ③ Control measures: Western medicine/blank retention enema. ④ Intervention measures: Retention enema(with integrated traditional Chinese and western medicine). ⑤ Evaluation indexes of study results:Effects of enema and symptom scores. ⑥ Available raw data of the literature.
Exclusion criteria
Literatures met one or more of the following were excluded. ① Abstracts, conference papers,letters, and periodical literatures with data errors or missing. ② Multiple submissions. ③ The full text was unknown. ④ Non-Chinese and English literatures. ⑤ Categories of research progress,case sharing, conference guidelines and basic study. ⑥ Papers without original data or papers whose data could not be used. ⑦ Incomplete randomized controlled trial (RCT) studies, including quasi-randomized controlled studies (e.g. studies with allocation plans based on dates of visits or ID tail numbers) and studies lacking comparison on efficacy before and after in the control group. ⑧Those without evaluation indexes of relevant study results. ⑨ Retrospective studies. ⑩ Missing or incomplete efficacy evaluation standards. Without description on ways of administration.
Literature Retrieval Strategies
Relevant requirements and guidelines in the work manual of the international medical center The Cochrane Collaboration were followed. Computers were used to search CNKI, Wanfang, VIP, CBM,Embase, Central and Medline. Search dates were stopped by May 2020. Chinese and English were search languages. Chinese search terms included"放射性直肠炎", "放射性肠炎", "放射性直肠粘膜损伤", "放射性直肠", "肠澼", "中西医结合", "中西医", "保留灌肠" and "灌肠". English search terms included "radiation enteritis" "RE" "radiation proctitis""combination of traditional Chinese and Western medicine" "Integrated Chinese and Western Medicine" and "Enema". Combination of subject terms and freed terms was applied for searching, and references of the included literatures were tracked.
Literature Screening
EndNote X9 file management software was applied to remove repetitive literatures. Then,2 system reviewers read titles and abstracts to screen literatures in strict accordance with the above inclusion and exclusion criteria to remove unqualified literatures. By reading full texts carefully to clarify the final included ones. When there were conflicts or disagreements, they were negotiated by the 2 or with the third system reviewer. When having incomprehension during literature screening, original authors could be contacted. If the original authors were unavailable, the literatures would be excluded.
Data Extraction
Data extraction included basic situations of studies, study methods, sample sizes, outcome indicators, etc. Two system reviewers independently screened literatures based on the above criteria, and at the same time performed quality evaluation and cross-checked the results. In case of disagreements,the third researcher would participate in discussions and make decisions through consultation. At the same time, the authors of the literatures would be contacted to clarify the reliability of study related information.
Quality Evaluation
Standards inCochrane Review Handbook 5.0were followed to evaluate the quality of included literatures. The evaluation mainly focused on the following aspects. ① Whether random grouping was used in the clinical trial. ② Whether allocation concealment was performed in the clinical trial. ③Whether blinding was used to avoid implementation bias and measurement bias. ④ Whether study outcome indicators were complete. ⑤ Whether the study outcome indicators were selectively reported.⑥ Whether there was bias caused by other factors.Risk assessment on each item was based on specific conditions of included studies. Two system reviewers independently extracted relevant data and conducted corresponding data analysis. In addition,after extracting the data, they were cross-checked. If there were conflicts or disagreements, they could be resolved through discussion and communication or inviting a third person to determine. When extracting the data, if it was found that there was a lack of data required for this study, the original author was contacted in order to complete the data.
Statistical Analysis
Meta-analysis was performed by using RevMan 5.3 software. When testing whether there was heterogeneity among the included literatures,P>0.1 was set as the test criterion. IfP>0.1, it meant that the heterogeneity among the included literatures was small and they could be amalgamated. In this case, the fixed effect model was used. On the contrary, the random effect model was selected.The heterogeneity test was performed by usingI2quantitative analysis, andI2>50% was considered to be heterogeneous. In this case, the random effect model was used, otherwise the fixed effect model was selected. Analysis on efficacy indicators was conducted by using odds ratios (OR), and a 95% confidence interval (CI) was given. Existence of potential publication bias was analyzed with an"inverted funnel" plot.
RESULTS
Literature Screening Results
A total of 236 literatures were retrieved in the initial search, and 152 literatures were obtained after removing duplicates. After reading the titles and abstracts of the literatures, 88 literatures were screened out, and then a second screening was performed on the basis of the full text reading.Literatures with clinical study trial designs that were not in accordance with the inclusion and exclusion criteria were screened out, and 12 literatures were included, in which the random grouping method was applied in their trial designs, and the literatures were all from China. Detailed literature screening steps and the final included studies are shown in Figure 1.A total of 941 patients were included, including 488 in the trial group and 453 in the control group. Basic characteristics of the included literatures are shown in Table 1.

Figure 1. Literature Retrieval Flow Chart
Evaluation on Literature Quality
A total of 12 literatures were finally included in this study. Standards in the Cochrane ReviewHandbook 5.0 were followed to evaluate the quality of the included literatures. ① The random grouping method: In the included literatures, the random number table method was used for study grouping in 2 clinical trials, grouping based on the order of visits was used in 1 clinical study, and the remaining 9 clinical study literatures only mentioned the use of random grouping, without clearly explaining specific grouping methods. ② The allocation concealment scheme: It was mentioned in none of the studies. ③Blinding: It was mentioned in none of the studies.④ Outcome data: All study outcome data were complete. Selective reporting: Selective reporting of all the studies was unclear. ⑤ Other bias: Bias caused by other factors in all the studies was unclear.The quality evaluation is shown in Figure 2 and Figure 3.
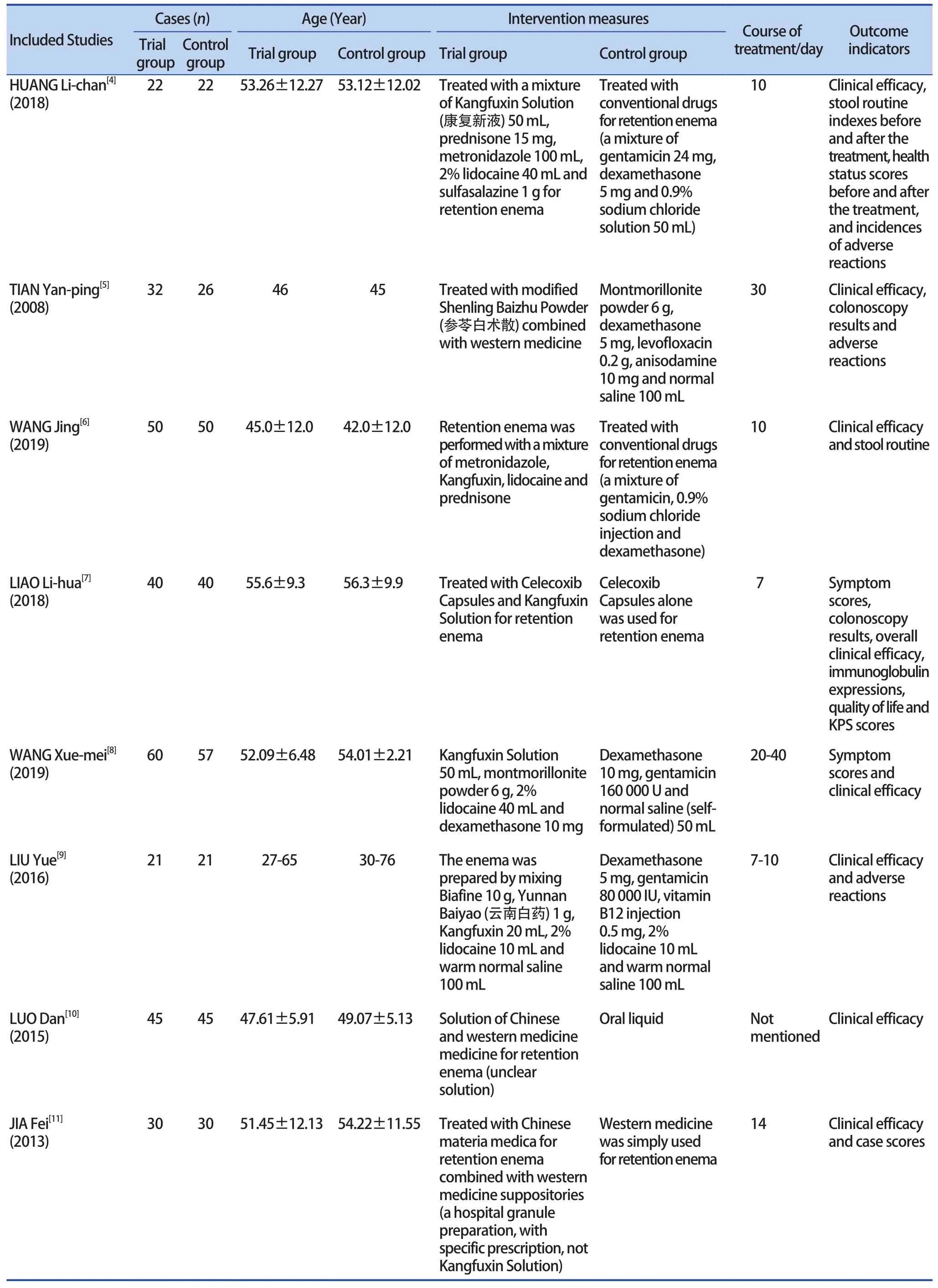
Table 1. Basic Characteristics of Included Literatures
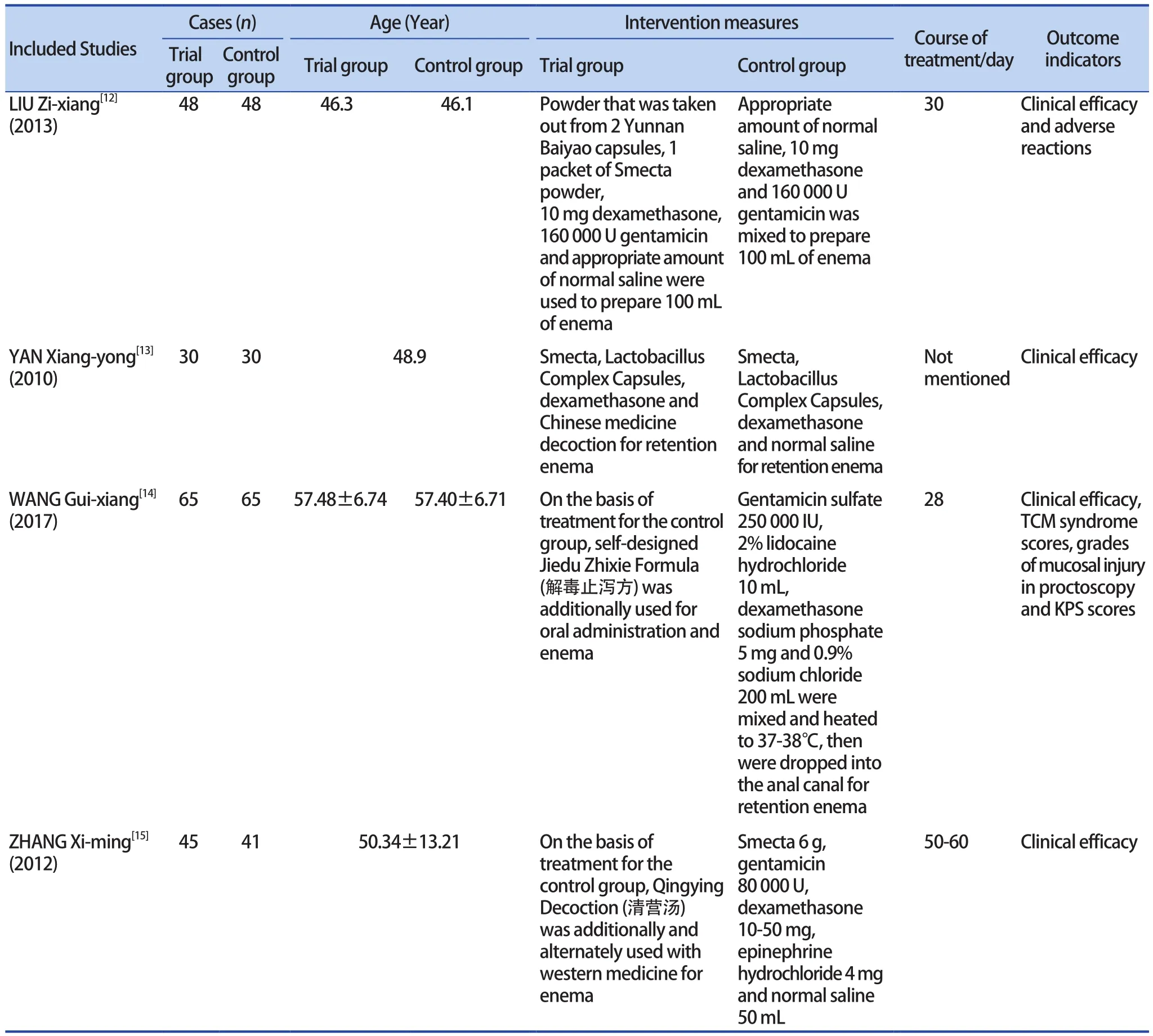
(Continued Table 1)
Results of Meta-Analysis
Clinical efficacy
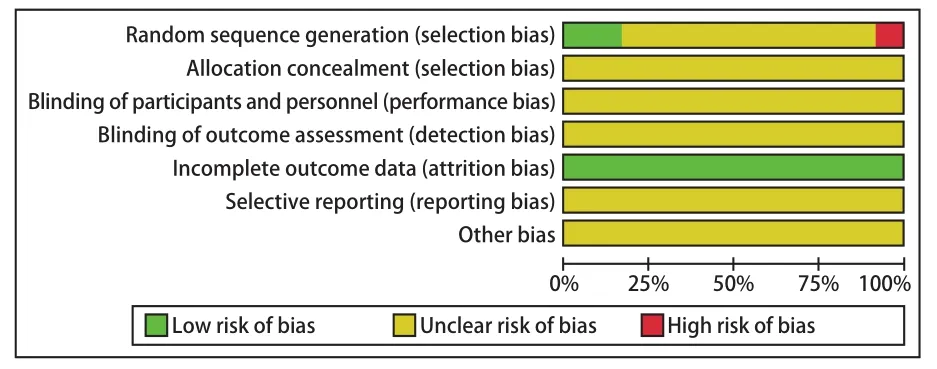
Figure 2. Quality Evaluation on Included Literatures
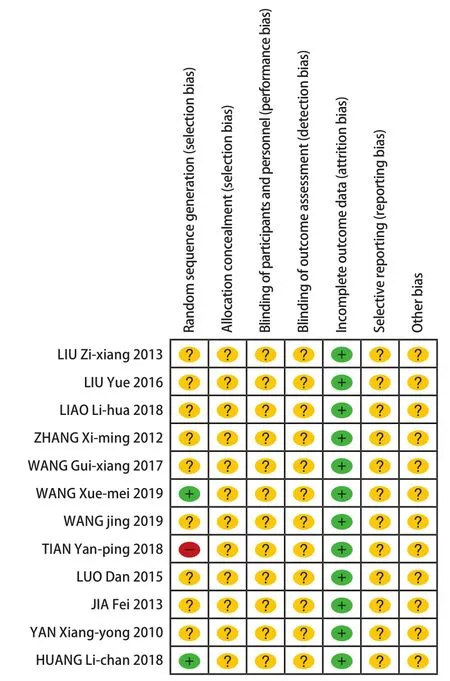
Figure 3. Quality Evaluation on Included Literatures
The 12 clinical study literatures included in this paper all reported clinical efficacy of retention enema for RP with integrated traditional Chinese and western medicine. The total sample size was 941 cases, of which 488 cases were included in the trial group and 453 cases in the control group. Heterogeneity analysis showed that there was no heterogeneity among the results of the clinical study trials (P=0.82,I2=0%), and they could be amalgamated, so the fixed effect model was chosen for data analysis. Results of Meta-analysis showed that in terms of the clinical efficacy on RP, the comparative study between the trial group and the control group was statistically significant (P<0.000 01). The result of combined test analysis wasZ=8.96, and the combined effect size and 95% CI of the clinical efficacy were (OR=5.96,95% CI [5.50, 14.29]), indicating that clinical efficacy of retention enema with integrated traditional Chinese and western medicine on RP is better than that of simple western medicine enema or blank enema. The results are shown in Figure 4.
An "inverted funnel" plot with OR as the abscissa and log[OR] as the ordinate was drawn.Existence of publication bias of the 12 finally included clinical study literatures was analyzed.Results are showed in Figure 5 that it is symmetrical,indicating less publication bias.
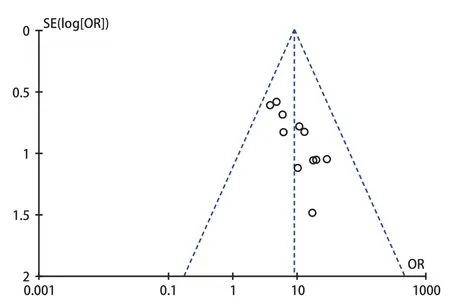
Figure 5. Funnel Plot of Publication Bias

Figure 4. Forest Map of Improvement of Clinical Efficacy
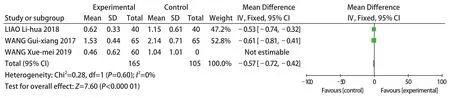
Figure 6. Forest Map of Improvement of Abdominal Pain
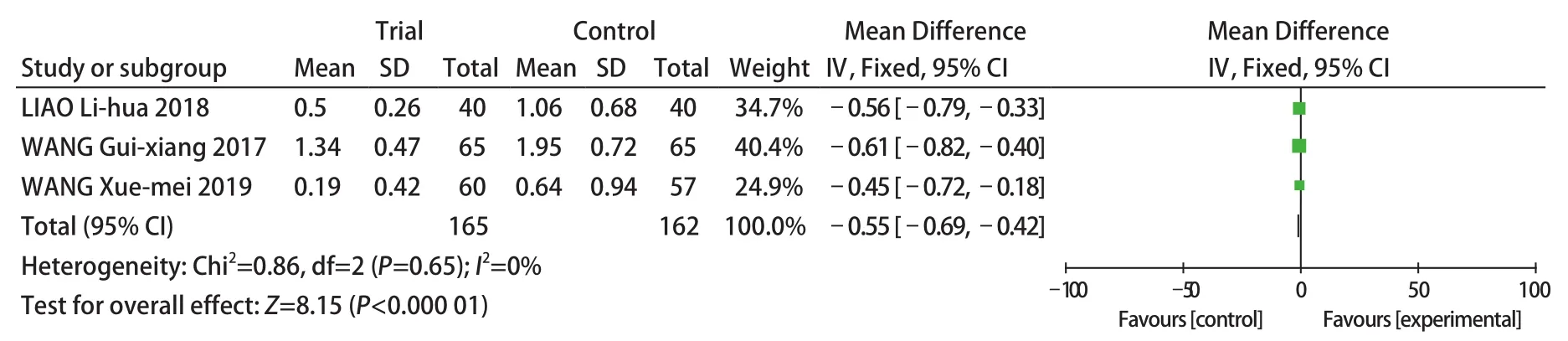
Figure 7. Forest Map of Improvement of Hematochezia
TCM symptoms
Abdominal pain: Among the 12 literatures included in this study, there were 3 literatures comparing the symptom of abdominal pain. The heterogeneity analysis showed that there was no statistical heterogeneity among the clinical study trial results of the 3 literatures (P=0.6,I2=0%). That is, homogeneity of the included clinical studies was good, so the fixed effect model was used for data analysis. The results of Meta-analysis showed that the comparative study between the trial group and the control group show a statistically significant in difference improving the symptom of abdominal pain in RP (P<0.000 01). The result of combined test analysis wasZ=7.60, the MD value was the combined statistical magnitude, and the combined effect size and 95% CI of the data were (MD=-0.57, 95% CI [-0.72, -0.42]). It shows that retention enema with integrated traditional Chinese and western medicine for RP is better than simple western medicine enema or blank enema in alleviating and improving abdominal pain in RP. The results are shown in Figure 6.
Hematochezia: Among the 12 literatures included in this study, there were 3 literatures comparing the symptom of hematochezia. The heterogeneity analysis showed that there was no statistical heterogeneity among the clinical study trial results of the 3 literatures (P=0.65,I2=0%), indicating that homogeneity of the included studies was good,so the fixed effect model was used. The results of the Meta-analysis showed that in correcting and improving the symptom of hematochezia in RP patients, comparison on efficacy in the trial group and the control group was statistically significant(P<0.000 01). The result of combined test analysis wasZ=8.15, the MD value was the combined statistical magnitude, and the combined effect size and the 95% CI of the data were (MD=-0.55,95% CI [-0.69, -0.42]). It shows that in correcting and improving the symptom of hematochezia,retention enema with integrated traditional Chinese and western medicine for RP has a better clinical efficacy. The results are shown in Figure 7.
Diarrhea: In this study, there were 2 literatures comparing the symptom of diarrhea. The heterogeneity analysis showed that there was no statistical heterogeneity between the clinical study trial results of the 2 literatures (P=0.22,I2=32%), indicating that homogeneity of the included studies was good, so the fixed effect model was used. The results of the Meta-analysis showed that for the diarrhea symptom in RP, comparison on treatment methods between the trial group and the control group was statistically significant (P<0.000 01). The result of combined test analysis wasZ=6.41, the MD value was the combined statistical magnitude, and the combined effect size and the 95% CI of the data were (MD=-0.69,95% CI [-0.91, -0.48]). Therefore, for correction and improvement of diarrhea, the clinical efficacy of retention enema with integrated traditional Chinese and western medicine for RP is better than that of simple western medicine enema or blank enema.The results are shown in Figure 8.

Figure 8. Forest Map of Improvement of Diarrhea
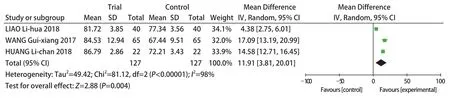
Figure 9. Forest Map of KPS
KPS
KPS was compared in 3 of the 12 literatures included in this study. The heterogeneity analysis showed that there was statistical heterogeneity among the trial results (P=0.004,I2=98%), so the random effect model was used. The results of the meta analysis showed that for treating RP, KPS scores in the trial group and the control group were statistically significant (P<0.000 01). The result of combined test analysis wasZ=2.88, the MD value was the combined statistical magnitude, and the combined effect size and the 95% CI of the data were (MD=11.91, 95% CI [3.81, 20.01]). It indicates that retention enema with integrated traditional Chinese and western medicine for treating RP has statistical significance, compared to simple western medicine enema or blank enema. The results are shown in Figure 9.
DISCUSSION
RP has no corresponding records in ancient literatures. It is a disease caused by extensive use of radiotherapy technology in tumor treatment with its development. According to its relevant clinical symptoms, it can be classified into "dysentery","diarrhea" "hematochezia" "radiation proctitis"and so on in TCM. Chinese scholars believe that the basic pathogenesis of its occurrence is related to fire-heat-toxin pathogens, dampnessheat, stagnation of Qi (气), radioactive rays,phlegm and blood stasis, spleen deficiency,etc. The onset is mostly caused by radiation damage to the rectal mucosa. At present, there are different opinions on the treatment of this disease, without consensus, and each treatment has distinct advantages and disadvantages. There are problems in TCM treatment for RP, such as syndrome differentiation, various prescriptions and inconsistent judgment criteria on clinical efficacy, so that there is no clear, unified and effective method for its treatment. Western medicine mainly treats RP with symptomatic treatments like anti-inflammatory,antibiotics, probiotics, antioxidant antidiarrheal agents, somatostatin, etc.[2]But it has disadvantages like easy to relapse, severe adverse reactions, not suitable for long-term use, and unsatisfactory clinical efficacy. Therefore, for the RP treatment, the latest study believes that efficacy of integrated traditional Chinese and western medicine is better. By retention enema, drugs can directly act on lesions of the rectal mucosa. Therefore, theConsensus on Diagnosis and Treatment for Radiation Proctitisrecommends that "anal dripping retention enema" is the best therapeutic plan for RP[3].
In recent years, the incidence of tumors has been "constantly high". As a common treatment for tumors, radiotherapy will inevitably cause RP in patients undergoing pelvic radiotherapy. The occurrence of this disease will seriously affect the efficacy and quality of life in patients with tumors, and the various treatment methods for this disease are difficult to achieve significant clinical efficacy, and sometimes even backfire and have a counterproductive effect. In view of the lack of effective treatment methods, a number of relevant clinical studies have been carried out in recent years. According to the latest study, retention enema with integrated traditional Chinese and western medicine has obvious advantages. However, due to problems in the early studies, such as few cases enrolled in the groups, lack of comprehensive study content, imperfect study methods and so on, further study is necessary.
Therefore, a method in evidence-based medicine was applied in this study to explore clinical efficacy of retention enema with integrated traditional Chinese and western medicine for RP. When comparing the retention enema with integrated traditional Chinese and western medicine with single western medicine or blank enema, it was found that the retention enema with integrated traditional Chinese and western medicine had better clinical efficacy. This treatment plan also had significant advantages in improving and correcting symptoms of diarrhea, abdominal pain, hematochezia, etc.In terms of KPS scores, when comparing the trial group with the control group, the study result is also statistically significant. The significance of this study result is that it not only provides certain evidencebased medical support for evaluation on the clinical efficacy of retention enema with integrated traditional Chinese and western medicine for RP, but also provides an idea and reference of diagnosis and treatment for clinicians during clinical diagnosis and treatment. Through literature collection, expansion of the study base and comprehensive analysis,efficacy of retention enema with integrated traditional Chinese and Western medicine was analyzed more accurately and efficiently from multiple angles.Supported by scientific data, necessity, rationality and high efficiency of retention enema treatment with integrated traditional Chinese and western medicine was also evaluated more accurately and objectively.However, this study also has its shortcomings.First of all, although a Chinese and English search was conducted, after many times of screening,the final clinical study literatures included were all Chinese literatures, which lacked a certain degree of comprehensiveness. The included literatures were generally of low quality in trial study methodology,and plans for allocation concealment and blinding were not mentioned. In terms of KPS data, there was statistical heterogeneity, which might be related to the small number of included clinical studies. Therefore,this study only conducted a preliminary systematic review on the retention enema with integrated traditional Chinese and western medicine for RP, in order to appeal to more and in-depth understandings,which need to be proved by more rigorous designed,high-quality and multi-center randomized double-blind clinical controlled trials.
猜你喜欢
阅读(低年级)(2022年2期)2022-03-12 14:08:09
中国民间疗法(2021年7期)2021-07-22 06:43:42
中国民间疗法(2021年8期)2021-07-22 05:53:16
阅读(低年级)(2021年11期)2021-03-08 10:47:52
医学综述(2021年2期)2021-01-29 06:51:58
作文评点报·低幼版(2020年42期)2020-12-14 03:53:59
摄影与摄像(2020年11期)2020-09-10 07:22:44
中国继续医学教育(2015年6期)2016-01-07 07:38:47
中国医疗美容(2015年1期)2015-07-12 10:06:58
中国医疗美容(2015年1期)2015-07-12 10:06:21
 World Journal of Integrated Traditional and Western Medicine2020年11期
World Journal of Integrated Traditional and Western Medicine2020年11期
- World Journal of Integrated Traditional and Western Medicine的其它文章
- INSTRUCTION FOR AUTHORS
- Summary on Professor QIAO Bao-zhang's Experience in Syndrome Differentiation and Treatment for Pancreatic Cancer
- Summary on SHANG Hong-tao's Experience in Treating Alopecia of Spleen Deficiency with Shengyang Sanhuo Decoction (升阳散火汤)
- A Study on the Correlation Between Cerebral Small Vascular Disease and Constitution Types of Traditional Chinese Medicine
- A Randomized Controlled Clinical Trial on Efficacy and Safety of Electroacupuncture on Oral Oxycodone Hydrochloride Prolonged-Release Tablets Related Constipation