
Intraoperative care of elderly patients with COVID-19 undergoing double lung transplantation:Two case reports
2020-04-08 06:08
World Journal of Clinical Cases 2020年22期
Qi Wu,Ying Wang,Han-Qian Chen,Operating Room,The First Affiliated Hospital,Zhejiang University School of Medicine,Hangzhou 310003,Zhejiang Province,China
Hui Pan,Department of Lung Transplantation Surgery,The First Affiliated Hospital,Zhejiang University School of Medicine,Hangzhou 310003,Zhejiang Province,China
Abstract BACKGROUND Lung transplantation is considered an effective method for treating patients with end-stage coronavirus disease 2019 (COVID-19). The nurses play a pivotal role in lung transplantation for COVID-19 patients.CASE SUMMARY Two elderly patients were admitted to the emergency department due to cough,and the nucleic acid test was positive. The patients were preliminarily diagnosed with COVID-19. The chest computed tomography scan revealed massive lung consolidation,and the patients did not improve after treatment with antiviral drugs,glucocorticoids,antibiotics,and other drugs. Under the support of pure oxygen in extracorporeal membrane oxygenation,the patients’ oxygen levels were still poor,indicating that they were in the terminal stage of viral pneumonia. The patients underwent double-lung transplantation and received intraoperative care.The extracorporeal membrane oxygenation device was removed within a week of the surgical procedure,and the respiratory circulation of the patients were stabilized.CONCLUSION High-quality care for COVID-19 patients undergoing lung transplantation ensures patient safety during operation while protecting the safety of the medical staff.
Key Words: Lung transplantation; Extracorporeal membrane oxygenation; COVID-19;Intraoperative care; Third-level protection; Case report
INTRODUCTION
The outbreak of coronavirus disease 2019 (COVID-19) has rapidly spread globally[1,2].The basic pathophysiological mechanisms of COVID-19 involve binding the spike protein of the virus to the angiotensin-converting enzyme 2 receptor on the cell membranes of the body. This subsequently results in a local and systemic inflammatory response,oxidative stress,and tissue and cell hypoxia when the virus enters the host cell[3]. The progression and outcome of COVID-19 depend on how the immune system responds. In short,mild pneumonia patients may have no obvious clinical manifestations. However,in patients with severe pneumonia,the ailment can quickly progress to acute respiratory distress syndrome,sepsis,metabolic acidosis,disseminated intravascular coagulation,and multiple organ failure,eventually leading to death. In particular,poor prognosis is typical in elderly patients and in people with severe underlying conditions like tumors that weaken immunity[4].
When COVID-19 infection leads to irreversible end-stage respiratory failure,the only surgical procedure that can be performed is lung transplantation. In patients with COVID-19,the three primary medical prerequisites for lung transplantation are as follows:(1) Bilateral respiratory failure should be irreversible after the patients have been kept under ventilator support and extracorporeal membrane oxygenation(ECMO); (2) The nucleic acid test results should continuously be negative after treatment; and (3) The functionality of the other organs should be normal and able to withstand lung transplantation[5].
Intraoperative care plays an important role during lung transplantation. In our study,we have proposed primary nursing methods during double-lung transplantation in elderly patients with COVID-19.
CASE PRESENTATION
Chief complaints
Case 1:A 66-year-old woman who complained of coughing for 13 d,fever for 3 d,and shortness of breath for 2 d was admitted to The First Affiliated Hospital,Zhejiang University School of Medicine,Medical College.
Case 2:A 77-year-old man who complained of coughing for more than 15 d was admitted to the hospital.
History of present illness
Case 1:The nucleic acid test was positive,and the patient was preliminarily diagnosed with COVID-19 and acute respiratory failure.
Case 2:The nucleic acid test was positive,and the patient was preliminarily diagnosed with COVID-19,hypertension,and diabetes.
History of past illness
Case 1:The patient denied any history of hypertension,diabetes,heart disease,kidney disease,tuberculosis,viral hepatitis,and other diseases. She underwent appendectomy 34 years ago.
Case 2:The patient had a history of diabetes for more than 10 years and usually took“xiaoke pills” orally to reduce glucose. He had a history of hypertension for 5 years and usually took “Zhenju antihypertensive tablets” for antihypertensive treatment.
Personal and family history
Case 1:The patient denied any family history of related diseases.
Case 2:The patient denied any family history of related diseases.
Physical examination
Case 1:On admission,the following vital signs were noted:temperature (T):36.9 °C,heart rate:106 bpm,and invasive arterial blood pressure:141/84 mmHg.
Case 2:On admission,the following vital signs were noted:temperature (T):36.1 °C,heart rate:100 bpm,and invasive arterial blood pressure:158/68 mmHg.
Laboratory examinations
Case 1:The patient was ventilatedviaveno-venous ECMO (VV-ECMO) with the ventilator in tracheostomy (pressure-controlled mode). The arterial blood gas analysis results were as follows:fraction of inspired oxygen:100%,positive end-expiratory pressure:27 cmH2O,personality sensitivity:7 cmH2O,oxygen saturation:88%,lactic acid:1.8 mmol/L,bicarbonate:24.6 mmol/L,partial pressure of carbon dioxide:39 mmHg,partial pressure of oxygen:57 mmHg,and blood pH:7.42. The routine blood tests showed white blood cell count:10.1 × 109/L,neutrophil (%):92.5%,lymphocyte(%):4.9%,lymphocyte count:0.3 × 109/L,platelet count:136 × 109/L,hemoglobin:87 g/L,fibrinogen level:5.56 g/L,D-dimer:36 μg/L,IgG level:782-1131 mg/dL(pretransplantation),653-1349 mg/dL (post-transplantation),and glutamic-oxaloacetic transaminase:36 U/L.
The stool and urine volumes of the patient were normal. The drugs administered to the patient included lopinavir and ritonavir tablets (2 pills,twice daily),arbidol dispersible tablets (2 pills,thrice daily),methylprednisolone (40 mg,q12h),gamma globulin (5 g,q6h),and tazocin (4.5 g q8). The nucleic acid test results were continuously negative after treatment.
Case 2:The patient was ventilatedviaVV-ECMO with the ventilator in the tracheostomy (pressure-controlled mode). The arterial blood gas analysis results were as follows:fraction of inspired oxygen:40%,positive end-expiratory pressure:5 cmH2O,personality sensitivity:20 cmH2O,partial pressure of carbon dioxide:39 mmHg,and partial pressure of oxygen:57 mmHg. Laboratory tests revealed the following:white blood cell count:5.9 × 109/L,red blood cell count:3.20 × 109/L,platelet count:56× 109/L,hemoglobin:98 g/L,serum procalcitonin (0.28 ng/mL),B-type natriuretic peptides (1226 pg/mL),high-sensitivity cardiac troponin (375 ng/mL),albumin (47.9 g/L),globulin (19.0 g/L),direct bilirubin (25 μmol/L),indirect bilirubin (24.6 μmol/L),high-sensitivity C-reactive protein (111.04 mg/L),prothrombin time (16.8 s),and IgG level:1211-3533 mg/dL (pretransplantation). The nucleic acid test results were continuously negative after treatment.
Imaging examinations
Case 1:The computed tomography (CT) scan showed massive lung consolidation and edge unclear (Figure 1A).
Case 2:The CT scan showed patchy and cable-shaped ground glass density,and height shadows can be seen on both sides of the lungs with unclear edges and uneven internal density (Figure 2A). No obvious positive foreign body in trachea and bronchus. No obvious changes in the morphology of the heart and great vessels; no obvious pericardial effusion. No obvious rib dislocation fracture.
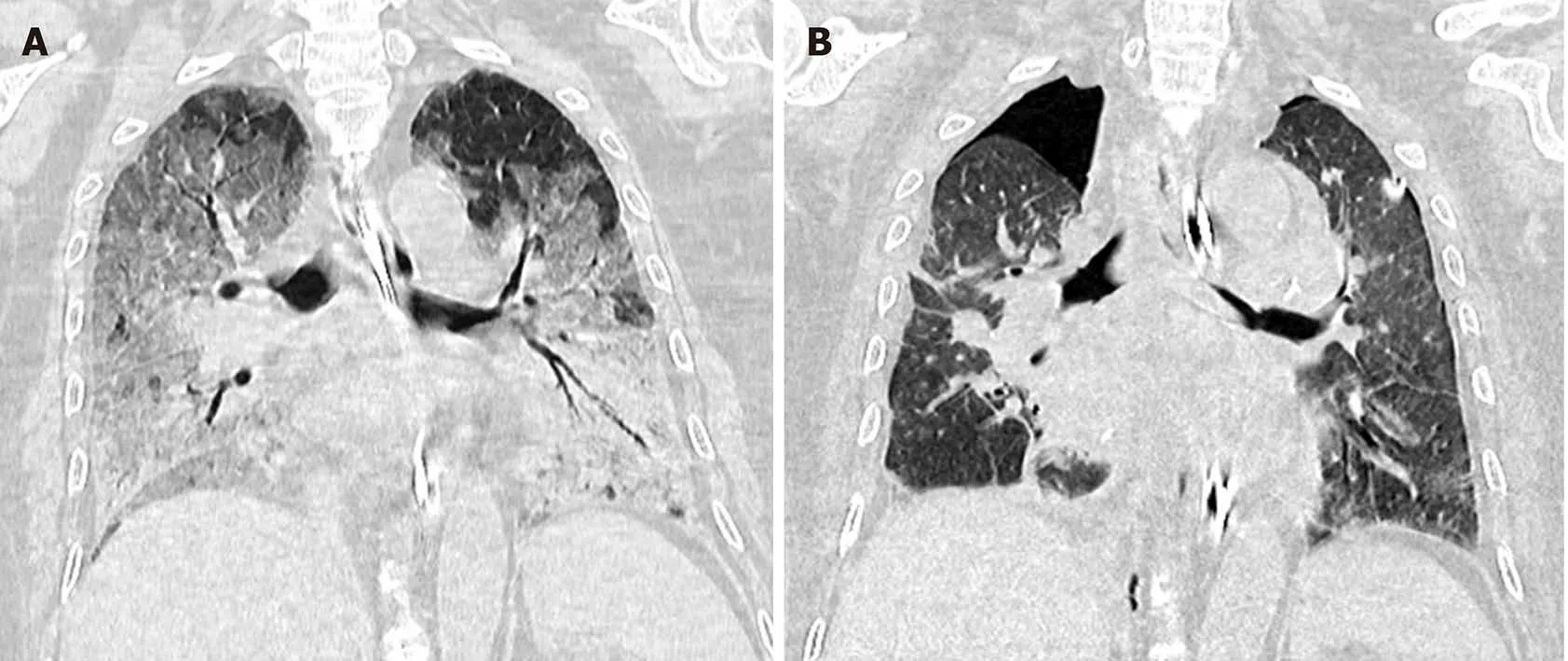
Figure 1 Chest computed tomography scan of Case 1. A:Pretransplantation; B:Post-transplantation.
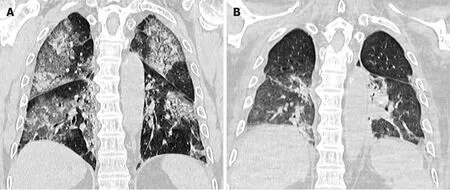
Figure 2 Chest computed tomography scan of Case 2. A:Pretransplantation; B:Post-transplantation.
FINAL DIAGNOSIS
The final diagnoses of these cases were COVID-19 and the terminal stage of viral pneumonia.
TREATMENT
After a discussion with the medical staff,it was concluded that the patient was in the terminal stage of viral pneumonia,and thus emergency lung transplantation was planned. Finally,we performed a double-lung transplant for the patient after 2 wk.
The patient was in the supine position under general anesthesia. The clamshell incision was chosen as the optimal surgical approach,and aortic intubation and right atrial efflux were performed to establish central venoarterial (VA) ECMO after opening the pericardium[6]. A parallel ECMO pattern with VV and VA was established with adjustable capacity. After separation of the lungs,pulmonary artery,pulmonary vein,and bronchus,the transplanted lung’s right side was removed depending on the patient’s lung functionality. Further,the trimmed lung underwent anastomoses based on the order of bronchus,arteries,and veins. The right lung was ventilated gradually,and unilateral pulmonary circulation was opened. The middle lobe of the right lung was removed for volume reduction. Similarly,left pneumonectomy and transplantation were performed. Once hemodynamic stabilization was achieved and the removal of right atrial and aortic intubation,VA ECMO was stopped. After strict hemostasis,the incision was closed layer by layer,and thoracic drainage tubes were placed on both sides.
Perioperative nursing measures
Preoperative preparation:A hundred-level laminar flow operation room was prepared for the donor’s lung. The negative pressure operation was selected for lung transplantation,and the circulating nurse set an appropriate temperature. Before the surgical procedure,the filter net at the return air inlet was disinfected by spraying a 2500 mg/L chlorine-containing disinfectant. This was followed by the nurse turning on the negative pressure system,which left the operating room in a state of high purification and negative pressure (differential static pressure ≥ 5 Pa). Equipment and objects not required for the surgical procedure were removed from the operating room. Objects in the operating room that would be difficult to clean were covered,and the operating table mattress was protected using an antipenetration sheet. The entire surgical procedure required four nurses’ involvement,which included two circulating nurses who were responsible for transferring the items (one nurse was present in the operating room and the other was in the buffer zone,outside the operating room) and two scrub nurses. According to the third-level protection standard,all the personnel involved in the surgical procedure possessed personal protective equipment(disposable medical protective clothing,disposable isolation garment,goggle,protective mask,N95 face mask,etc.). The disinfection process was performed by using chlorine-containing disinfectants (2500 mg/L) of 500 mL and 3000 mL for return air port and object surface,respectively,chlorine-containing disinfectants (5000 mg/L) of 10000 mL for soaking surgical instruments,and 75% alcohol of 800 mL for protective masks. The surgical instruments used were:One ECMO,one defibrillation monitor,one blood gas analyzer,two sets of electric attractors,one ambulatory cardiac telemetry monitor,and drainage tubes. As VA ECMO was established during the operation,the nurses had to prepare two sets of all the surgical items and use the instruments separately as required.
Intraoperative care:The circulating nurses used temperature control blankets to maintain the temperature of the patient’s limbs. The temperature changes of the extremities were frequently noted to ensure that the body temperature was maintained above 36.5 °C throughout the operation. Aortic intubation,right atrial intubation,and other conditions may lead to severe circulatory fluctuations or serious arrhythmia during the surgery. Therefore,the circulating nurses closely monitored the patient’s vital signs and detected any abnormal changes in a timely manner. In the case of an abnormal heart rate,blood pressure,or blood oxygen saturation,the nurses immediately notified the doctors to pause the operation,followed by the preparation of rescue equipment and active cooperation with the doctor to rescue the patient. The scrub nurses were responsible for assisting the physicians in disinfecting the patient’s skin at the surgical site and preparing sterile towels. The nurse had to replace the instrument in contact with the trachea in a timely manner. The nurses used sterilized magnet needle boxes to place the used stitches sequentially in pairs to avoid losing them. After the operation,the surgical supplies were simultaneously checked by a circulating nurse and a scrub nurse. Once all the items were accounted for accurately,a circulating nurse,along with an anesthesiologist,ensured that the drainage tubes were unblocked,and the catheter was secured to prevent it from pulling off. Finally,the nurses covered the patient using a disposable bed sheet and escorted the patient to the intensive care unit isolation room for handover to the intensive care unit isolation room nurses after the operating room nurse had worn protective equipment.
Postoperative disinfection:The surgical waste generated during the operation was treated as medical waste by the circulating nurse and placed inside double yellow garbage bags. These bags were sealed tightly with gooseneck ties and sprayed with 2500 mg/L chlorine-containing disinfectant,and then placed inside a single yellow garbage bag. This method ensured that the bag was packed twice at each layer (four layers in total),and each packaging layer was free of damage and penetration. Finally,the bags were labeled as COVID-19 and transferred into the special box. Similarly,the sharp instruments were placed in a plastic sharp ware box,sterilized similar to that mentioned above,followed by being labeled as COVID-19 and transferred to the special box for medical waste. Prior to being cleaned and sterilized using conventional methods,the surgical instruments were disinfected by soaking them in 10 L of chlorine-containing disinfectant at a concentration of 5000 mg/L for 30 min. Further,the surgical instruments were double sealed in a special container to prevent leakage and labeled as COVID-19. The surfaces in the operating room,such as instrument tables,operating tables,and the floor,were sterilized with 2500 mg/L chlorinecontaining disinfectants. Hygroscopic materials could be used to remove visible pollutants that might exist due to blood,body fluids,and secretions. Ultraviolet light was used to disinfect the air for more than an hour while closing the laminar flow and air supply port. The circulating nurses should also inform the hospital’s relevant departments to replace the air filter and high-efficiency filter on time[7].
OUTCOME AND FOLLOW-UP
The ECMO device was removed within a week of the surgical procedure,and the respiratory circulation of the patients was stabilized. CT scan of Case 1 at 12 d after transplantation showed symmetrical bilateral thorax,atrophy of the lung tissue,slightly patchy high-density shadows in both lungs,and lung parenchyma consolidated with bronchial signs (Figure 1B). CT scan of Case 2 at 16 d after transplantation revealed a small amount of gas density shadow in the thoracic cavity on both sides (Figure 2B). The volume of both lungs was compressed by about 15%.Multiple patchy increased density shadows in both lungs with unclear boundaries were noted. Inflammation and collapse of both lungs were improved compared to that prior to transplantation.
DISCUSSION
Currently,lung transplantation is a preferred treatment option for selected patients with end-stage pulmonary disease. Globally,approximately 4000 such procedures take place each year[8]. In comparison to intraoperative cardiopulmonary bypass,the use of VA ECMO decreases the risk of bleeding,hemolysis,and subsequent blood transfusion in patients with lung transplantation[9,10]. During the surgical procedure,the patient was placed in a lateral position,and a routine thoracotomy was performed after the establishment of VV-ECMO. Once the patient’s circulation had stabilized at the end of the operation,the VV-ECMO catheter was removed.
COVID-19 belongs to class B infectious diseases and is managed as a class A infectious disease,which has been stipulated according to China’s infectious disease prevention law. Lung transplantation is an optimal treatment method for patients with end-stage COVID-19. Nevertheless,bilateral lung transplantation for COVID-19 patients is a severe acute transplant procedure with a high degree of process and outcome uncertainty. Meanwhile,it is highly challenging in terms of the medical staff’s occupational exposure risk and the amount of physical strength required for continuous rescue under the third-level protection condition.
Firstly,the donor lung should be stored at a low temperature. During lung implantation,the scrub nurses should cover the donor’s lung’s surface with a salinesoaked gauze pad at 0-4 °C,which should be replaced frequently. This is performed so that surface cooling can guarantee the donor lung to be at a low temperature for an extended period. This allows ample time for anastomosis.
Due to the extended duration of double-lung transplantation and limitations of pulmonary ischemia,the nurses should help the patient to be positioned accurately and make positional changes as required during the operation. When the operation begins,the patient is placed in a supine position with the upper limbs fixed on a hand rest at a 90° angle to prevent brachial plexus nerve injury. The patient’s shoulders and bilateral pelvis are fixed using a fixation frame,and the knees are fixed with a restraint band. The operating bed is tilted at an angle within the range of 30°-45° toward the left or right,depending on the operating condition. The scrub nurses are responsible for placing pillows under the patient’s head to avoid pressure on the ears and using a foam dressing on the sacrococcygeal,iliac,heel,or ankle regions to prevent pressure sores. Owing to potential hematologic consequences and the cannulas’ positions and sizes,the patient should be monitored for limb ischemia,which occurs in 13% to 25%of the patients who receive VA ECMO[11]. The catheter is prevented from coming in contact with the skin through the use of foam dressing. Compression from the catheter should be avoided,especially when changing the patient’s position,to prevent instrument-related pressure injury.
For ECMO patients,the circuit is maintained by an ECMO specialist and a critical care nurse,who monitors the circuit for problems,maintains circuit connections,and evaluates the tube for cracks in a timely manner[12]. Due to extended trauma over a long time with complicated drugs in lung transplantation,the circulating nurse needs to mark the established catheter and check the circuit every 30 min. When the operation is in progress,the nurses should prepare the necessary crystalloid fluid,plasma substitute,blood products,and rescue medicines in advance based on the doctor’s instructions. In addition,the volume infused,blood transfusion amount,intraoperative blood loss,effusion volume,and urine output of the patient are accurately monitored and recorded. After lung transplantation,the pulmonary vascular permeability increases due to ischemia and other injuries,and lymphatic drainage is significantly maladjusted,resulting in pulmonary edema[13].Therefore,it is necessary to limit the intraoperative input and adjust the infusion speed and fluid volume based on the urine volume. To keep the lungs dry,colloids and blood products are used to keep the patient in a reasonable dehydration state.
Also,the nurses should closely monitor the patient’s vital signs during the operation and ensure that the patient’s limbs are kept warm by regularly observing the changes in the temperature of the extremities. This temperature should be maintained above 36.5 °C. In particular,cardiac arrest may occur during transit after surgery.Therefore,the nurses should regularly monitor the patient’s vital signs to ensure safe transit. Once the patient’s vital signs begin to show large fluctuations and equipment issues are eliminated,the nurse should help the doctor perform first aid and then prepare for a re-thoracotomy operation.
CONCLUSION
In conclusion,nurses must provide excellent intraoperative care for patients with COVID-19 undergoing lung transplantation. In comparison with traditional lung transplantation,the nurses should ensure adequate preoperative preparations,monitor the condition of various catheters in a timely manner,cooperate with the team to complete the operation,and perform the final disinfection. While ensuring a successful operation,the nurses can provide high-quality care and safety to patients with COVID-19,thus preventing the infection of the medical staff.
 World Journal of Clinical Cases2020年22期
World Journal of Clinical Cases2020年22期
- World Journal of Clinical Cases的其它文章
- COVID-19:A review of what radiologists need to know
- Holistic care model of time-sharing management for severe and critical COVID-19 patients
- Bioequivalence of two esomeprazole magnesium enteric-coated formulations in healthy Chinese subjects
- Osteoprotegerin,interleukin and hepatocyte growth factor for prediction of diabetes and hypertension in the third trimester of pregnancy
- High serum lactate dehydrogenase and dyspnea:Positive predictors of adverse outcome in critical COVID-19 patients in Yichang
- Risk factors analysis of prognosis of adult acute severe myocarditis