
Gastric mixed adenoma-neuroendocrine tumor:A case report
2020-04-08 06:08
World Journal of Clinical Cases 2020年22期
Shuzo Kohno,Hiroaki Aoki,Masaich Ogawa,Kazuhiko Yoshida, Department of Surgery,The Jikei University Katsushika Medical Center,Tokyo 125-8506,Katsushika-ku,Japan
Masayuki Kato,Department of Endoscopy,The Jikei University Katsushika Medical Center,Tokyo 125-8506,Katsushika-ku,Japan
Abstract BACKGROUND Gastric mixed adenoma-neuroendocrine tumors (NETs) are quite rare. In the 2019 world health organization classification of tumors of the digestive system,these were designated as a combination of grade 1 or grade 2 NETs and adenomas or tubular adenomas. There are no treatment guidelines for these tumors,and pathological and clinical studies are ongoing. Herein,we review previous case reports and present a case of gastric mixed adenoma-NET.CASE SUMMARY A 66-year-old man underwent gastrointestinal endoscopy for the evaluation of upper abdominal pain. Histopathological examination of the biopsy specimen indicated the possibility of gastric cancer. A histopathological examination by endoscopic submucosal dissection showed a mixed adenoma-NET that was completely excised by endoscopic submucosal dissection. No recurrence was observed on gastrointestinal endoscopy at the 6-mo follow-up.CONCLUSION Clinicians' awareness of this rare tumor is important for its timely diagnosis and treatment.
Key Words: Adenoma; Neuroendocrine tumor; Diagnosis; Pathology; Stomach treatment;Case report
INTRODUCTION
Neuroendocrine tumors (NETs) are a rare type of gastric tumor. Moreover,lesions with a combination of endocrine tumors and gastric adenomas have a very low incidence[1]. There are few case reports[1-8]of gastric mixed adenoma-NETs,and the clinical features are unknown. Advances in immunohistochemical staining and genetic analysis have led to their classification as mixed adenoma-NETs[9]. Gastric mixed adenoma-NETs are not commonly recognized by clinicians and are difficult to diagnose from a forceps biopsy specimen[1,7]. Herein,we report a case of gastric mixed adenoma-NET and review it together with 10 case reports.
CASE PRESENTATION
Chief complaints
A 66-year-old man presented with upper abdominal pain in September 2019.
History of present illness
The patient was receiving outpatient treatment to hypertension.In September 2019,he went to the clinic complaining intermittent epigastric pain and underwent gastrointestinal endoscopy.
History of past illness
The patient had a history of hypertension,hyperlipidemia,and colorectal polyps.
Personal and family history
There is nothing special to mention in personal and family history.
Physical examination
Physical examination was normal.
Laboratory examinations
Laboratory examinations are almost normal.
Imaging examinations
Endoscopy showed a superficial-elevated (0-IIa) granular lesion with a maximum diameter of 10 mm on the anterior wall of the gastric body (Figure 1).
Histopathological examinations
Histopathological examination revealed the proliferation of intestinal-type glands within the gastric mucosa and irregular branching in some of the glands. Despite mild nuclear stratification and enlargement,most of the visible glands were those of adenomas,although some had structurally atypical glands suggestive of a welldifferentiated adenocarcinoma (Figure 2). The change in the surrounding mucosa was diagnosed as atrophic gastritis.
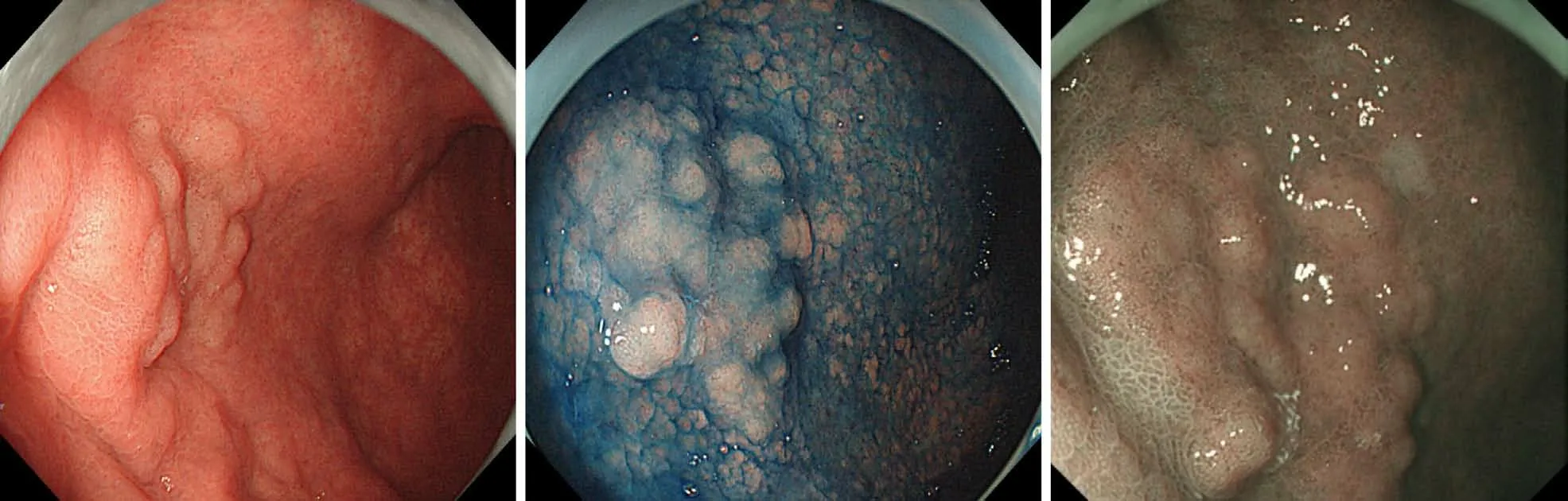
Figure 1 Gastroendoscopy findings. Endoscopic findings showed granular superficial elevated (0-IIa) lesion with a maximum diameter of 10 mm on the anterior wall of the gastric body.
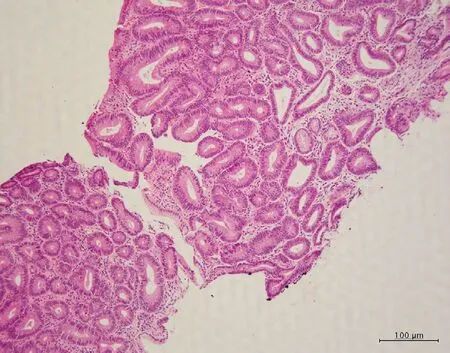
Figure 2 Pathologic examination. Microscopic examination (hematoxylin and eosin-stain) of biopsy specimen showed many ducts for adenomas,but some of them have structural atypical ducts,suggesting well-differentiated adenocarcinoma.
FINAL DIAGNOSIS
These cells resected by endoscopic submucosal dissection (ESD) were categorized as grade 1 (G1) NET cells. There was no submucosal invasion. Based on the histopathological features,the lesion was interpreted as a mixed adenoma-NET.
TREATMENT
Therefore,the patient underwent ESD in November 2019. The ESD-resected specimen measured 30 mm × 30 mm,and hematoxylin and eosin staining showed slightly elevated lesions with many superficial tubular or dilated glands without fusing. The glands were lined by moderately atypical epithelial cells,indicating a diagnosis of tubular adenomas (Figure 3). Immunohistochemically,these atypical cells were weakly positive for p-53,and scattered neuroendocrine cells (synaptophysin +chromogranin A) were present in the deep adenoma. Many cords and sheets of small neuroendocrine-type cells that formed small clusters or sheets were observed. These cells were diffusely positive for synaptophysin and keratin. Staining for chromogranin A occasionally tested positive,whereas testing for Ki-67 was rarely positive (< 1%),and for p-53 was negative (Figure 4). No molecular pathological examination was performed.
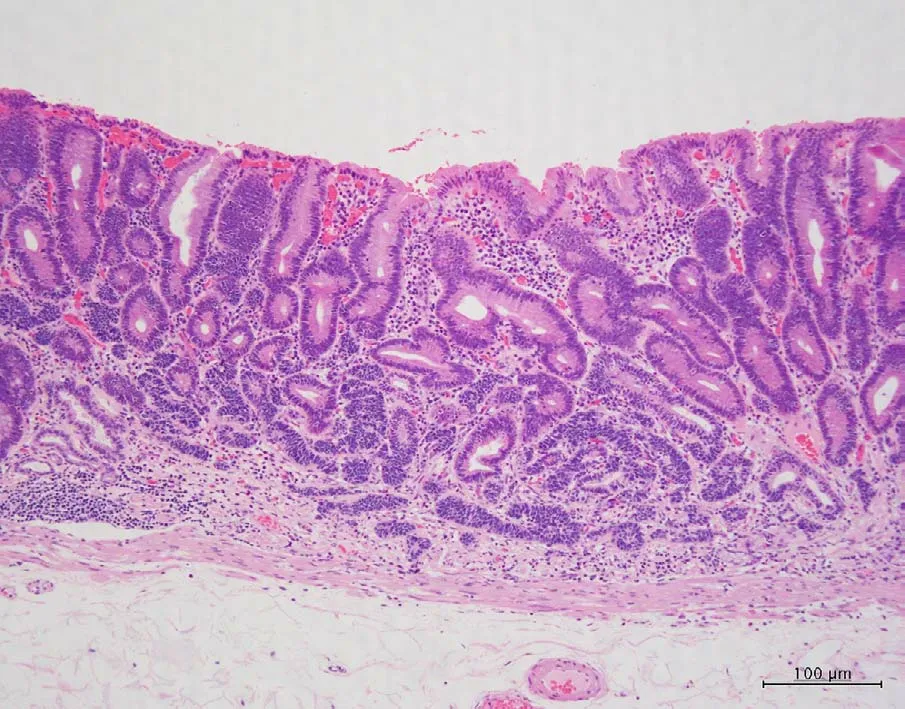
Figure 3 Pathologic examination. Microscopic examination (hematoxylin and eosin -stain) of resected gastric membrane showed mixture of superficial mucosal adenoma and deep mucosal neuroendocrine tumor.

Figure 4 Immunohistochemical staining for synaptophysin,chromogranin,Ki-67,and p-53. A:Immunohistochemical staining with synaptophysin showed diffuse staining in the cytoplasm of neuroendocrine tumor (NET); B:Immunohistochemical staining with chromogranin slightly stained the NET cytoplasm; C:Immunohistochemical staining with Ki-67 showed a MIB-1 index of 1% or less in the NET region; D:Immunohistochemical staining with p-53 showed almost no staining.
OUTCOME AND FOLLOW-UP
After ESD,the patient was discharged from the hospital without complications.Endoscopic examination conducted 6 mo after ESD showed no tumor recurrence.
DISCUSSION
Composite glandular carcinoid tumors of the digestive tract was first reported in 1988 by Moyanaet al[10]Owing to research progress,the definition of this lesion has changed over time. This lesion has received multiple names,including carcinoid tumor in adenoma,NET in adenoma,mixed adenoma well-differentiated neuroendocrine tumor,and mixed adenoma-NET[1-8]. Tumors with a mixture of glandular and neuroendocrine components in the gastrointestinal tract were classified as mixed neuroendocrine-non-neuroendocrine neoplasms (MiNEN) or mixed adenoma-NET following the 2019 World Health Organization (WHO) classification[9]. MiNEN includes mixed adenocarcinoma-neuroendocrine carcinoma or mixed adenoneuroendocrine carcinoma and mixed adenocarcinoma-NET. Mixed adenoma-NET has been classified separately from MiNEN in the 2019 WHO classification based on characteristic findings that were identified through advances in immunohistochemical staining and genetic testing[9]. Gastric mixed adenoma-NET is a rare tumor that is composed of G1 or grade 2 (G2) NETs as well as adenomas or tubulovillous adenomas. According to the 2019 WHO classification,neuroendocrine tumors (well-differentiated NETs with relatively low malignancy) are designated as G1 and G2 NETs. G1 and G2 are classified by the Ki-index[11,12]. As a typical pathological feature,the neuroendocrine component is generally located within the deep central portion of the polyp,whereas the adenomatous component occupies most of the periphery[1].
Although gastric lesions with mixed adenomas and NETs are rare,there are several reports showing similar cases[1-8]. 1 shows a report of gastric mixed adenoma-NETs.Eleven cases,including our case,have been reported. The average age was 65.1 years,and one of the cases was a female and the remaining cases were males. The average length of the tumor was 14.7 mm. The depth of invasion of the tumor was submucosal in 2 cases,mucosal in 8 cases,and unknown in 1 case. Treatment was ESD in 5 cases,polypectomy in 3 cases,gastrectomy in 2 cases,and unknown in the last case. No deaths were observed during the follow-up period. Endoscopic macroscopic findings included sessile polyps in 5 cases,0-IIa type polyp in 1 case,the endoscopic findings were unknown in 5 cases. Gastric adenoma-NET was diagnosed by forceps biopsy in 3 cases and by evaluation of the pathological specimen obtained by polypectomy in 2 cases. One case was diagnosed as adenoma,another case was suspected to be an adenocarcinoma,and the diagnoses of the remaining four cases were unknown.According to Leeet al[7],who reported three cases among the unknown cases,the pathological diagnosis of mixed adenoma-NET by forceps biopsy was difficult(Table 1).
In our case,an early gastric cancer was suspected before ESD,but histopathological examination led to a final diagnosis of gastric mixed adenoma-NET. This lesion may be misdiagnosed as an adenocarcinoma due to the mixture and fusion of the gastric adenoma and neuroendocrine cells in some areas[1,7]. When an adenoma is investigated by endoscopy,malignant findings are often unevenly distributed and it is difficult to reliably diagnose the presence of malignancy or NET component by biopsy[1,7,13,14].Localized endocrine neoplasia occurs frequently in both benign and malignant gastrointestinal tumors,whereas a truly mixed glandular endocrine neoplasia is a very rare tumor. Moreover,an accurate diagnosis based on histopathological examination of the biopsy specimen is difficult due to the presence of similar characteristics in MiNEN[15]. Mixed adenoma-NETs are considered difficult to diagnose by biopsy. To avoid a missed diagnosis,recognition of this disease is important. Consequently,diagnosis often requires histopathological examination by excision in addition to forceps biopsy[1].
The optimal treatment should be selected based on detailed results of the histopathological examination of the resected lesion. G1 NET is considered a low malignant potential tumor,although a few cases of lymph node metastasis in the same lesion have been reported,further research is required to ascertain the malignant potential of NETs[16,17].
To date,there are no therapeutic guidelines for mixed gastric adenoma and NET lesions. Hence,treatment is directed at the more aggressive and invasive lesions of the two components. Complete resection is the only treatment when the adenomatous part of the stomach is the more aggressive component. After the gastric cancer component is diagnosed as more aggressive,it is classified as MiNEN,and the treatment is performed following treatment for gastric cancer[18]. In cases where the NET component has a stronger or more aggressive malignant potential,we treated for NET following the recommended treatment methods[16,19]. Lymph node dissection is useful for lesions that are at high risk for lymph node metastasis[16]. Resection with lymphnode dissection is recommended in accordance with the NET classification and tumor size[16]. In NETs,the possibility of lymph node metastasis is defined by the size and depth of invasion; therefore,preoperative diagnosis is essential for lymph node dissection during tumor resection. Among NETs < 1 cm that invade the lamina propria or submucosa,the incidence of lymph node metastasis is reported to be 3.4%.Endoscopic resection may be appropriate for intraepithelial tumors < 2 cm,and perhaps tumors < 1 cm invading into the lamina propria or submucosa[16]. Thus,we believe that a combined therapeutic strategy and the application of current knowledge would lead to better treatment. Given that this is a rare disease,accurate diagnosis through histopathological analysis of the lesions and scrutinization of recent information is important to determine the treatment plan.
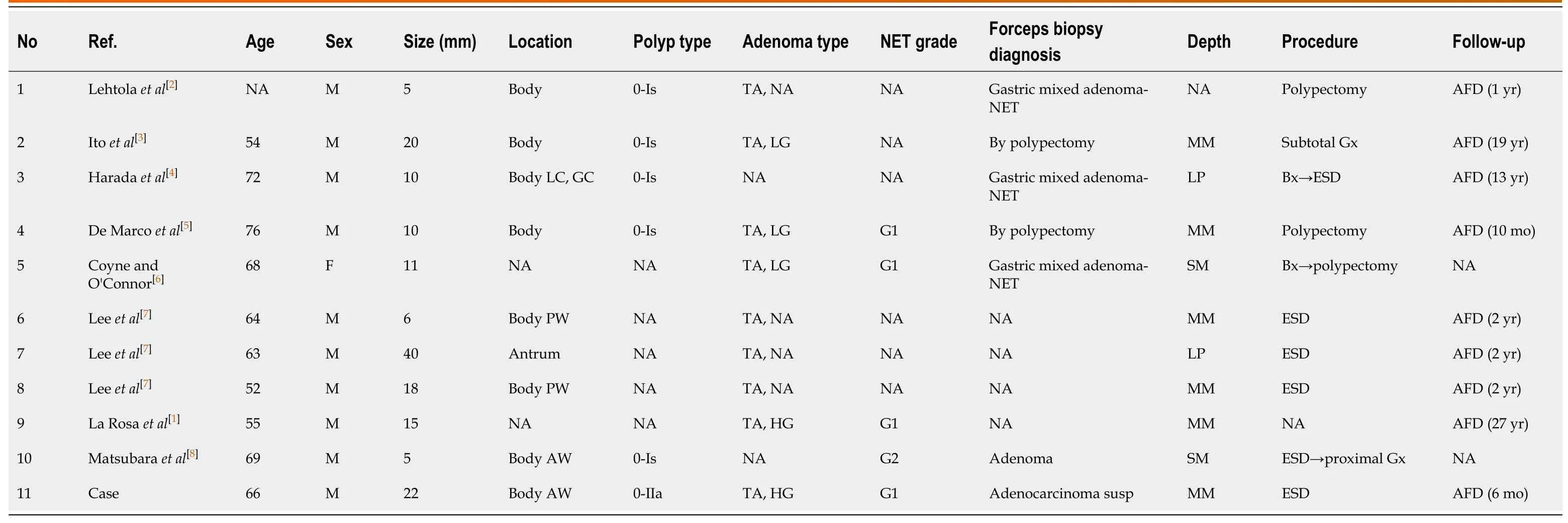
Table 1 Review of the literature,clinicopathological features of gastric mixed adenoma- neuroendocrine tumor
CONCLUSION
Mixed adenoma-NET may be found in gastric polyps,and its recognition is necessary for diagnosis and treatment.
ACKNOWLEDGEMENTS
We would like to thank Dr. Nomura K in the Department of Pathology for his guidance on the diagnosis of pathological tissues and the interpretation of lesions.
 World Journal of Clinical Cases2020年22期
World Journal of Clinical Cases2020年22期
- World Journal of Clinical Cases的其它文章
- COVID-19:A review of what radiologists need to know
- Holistic care model of time-sharing management for severe and critical COVID-19 patients
- Bioequivalence of two esomeprazole magnesium enteric-coated formulations in healthy Chinese subjects
- Osteoprotegerin,interleukin and hepatocyte growth factor for prediction of diabetes and hypertension in the third trimester of pregnancy
- High serum lactate dehydrogenase and dyspnea:Positive predictors of adverse outcome in critical COVID-19 patients in Yichang
- Risk factors analysis of prognosis of adult acute severe myocarditis