
Primary pulmonary malignant melanoma diagnosed with percutaneous biopsy tissue: A case report
2020-04-07 02:13:18JianMinXiHuanWenXueBingYanJinHuang
World Journal of Clinical Cases 2020年24期
Jian-Min Xi, Huan Wen, Xue-Bing Yan, Jin Huang
Jian-Min Xi, Huan Wen, Jin Huang, Department of Pathology, Hunan Academy of Traditional Chinese Medicine Affiliated Hospital, Changsha 410006, Hunan Province, China
Xue-Bing Yan, Department of Radiology, Hunan Academy of Traditional Chinese Medicine Affiliated Hospital, Changsha 410006, Hunan Province, China
Abstract BACKGROUND Primary malignant melanoma of the lung (PMML) is a rare and highly malignant tumor with a poor prognosis. Here, we report a PMML case diagnosed by computed tomography (CT)-guided percutaneous biopsy, describe its pathological features and review relevant literature to improve our understanding of this tumor.CASE SUMMARY A 64-year-old Chinese female presented with productive cough for 7 mo. A chest CT scan showed a large and space-occupying lesion in Lingual lobe. Positron emission tomography-CT revealed multiple nodules located in the superior lobe apicoposterior segment of her left lung. Brain magnetic resonance imaging showed numerous enhancing nodules, suggesting brain metastasis. Abdominal CT scan did not show any abnormalities. By CT-guided percutaneous biopsy, four pieces of gray and taupe tissues (1 cm length and 0.1 mm in diameter) were obtained. After pathologic examination, the tumor was found to consist of epidermal and nested small round cells, fibrosis and thin-walled blood vessels.The finding was suggestive of malignant melanoma. To confirm the diagnosis,pathological morphology and immunophenotypic features of the biopsy specimens were observed. The patient denied any history of skin tumors. No abnormal lesions were detected in other sites of the body. Molecular testing was positive for wild-type EGFR and KIT gene mutations. Finally, the clinical and pathological findings suggested PMML.CONCLUSION PMML is very rare, and the percutaneous biopsy tissue is limited. Therefore,comprehensive consideration of histology, immunohistochemistry, imaging, and clinical information is important for the diagnosis of PMML.
Key Words: Biopsy; Primary malignant melanoma of the lung; Malignant melanoma;Positron emission tomography-computed tomography; Pathology; Diagnosis; Case report
INTRODUCTION
Malignant melanoma (MM) is a malignant and highly aggressive tumor. It usually arises from embryonic neural crest melanocytes and occurs in the skin or mucosal surfaces. Primary MM of lung (PMML) is extremely rare, accounting for 0.01% of all primary lung tumors[1](Table 1); thus, pathologists have limited experience with the diagnosis of this tumor. The clinical and pathological evaluation criteria recommended by the Armed Forces Institute of Pathology are: (1) A solitary pulmonary tumor; (2) A MM confirmed by immunohistochemistry and/or electron microscopy; (3) No past history of excision or fulguration of cutaneous, mucosal, or ocular lesion; (4) A central pulmonary lesion; and (5) No observable tumor elsewhere at the time of diagnosis[1].Herein, we report a case of PMML diagnosed by computed tomography (CT)-guided percutaneous biopsy tissue and present its pathological morphology and immunophenotypic features with the aim to improve clinical understanding of PMML and avoid misdiagnosis.
CASE PRESENTATION
Chief complaints
A 64-year-old Chinese female was admitted to Hunan Academy of Traditional Chinese Medicine Affiliated Hospital due to productive cough for 7 mo, with blood in sputum,breathlessness and dizziness intermittently. She denied any history of skin cancer. No abnormal lesions were found in other parts of the body, including the skin, head, neck,scalp, anogenital region and eyes.
Laboratory examinations
Gross examination and molecular testing:Four pieces of gray and taupe tissue (1 cm length and 0.1 mm in diameter) were obtained.KITgene mutation was detected in the tumor tissue, while no specificEGFRmutations were found in the patient.
Microscopic examination:Histologically, the tumor was composed of small round cells and thin-walled blood vessels, with collagen fiber hyperplasia and few coagulative necrosis. The tumor cells were arranged in sheets, nests and a discohesive pattern and accompanied by vessels (Figures 1 and 2). The tumor cells were mostly medium-sized, rich in cytoplasm and light staining and had no clear boundary.Vacuolated nucleus and nucleoli and frequent mitoses were found in the tumor cells.However, a few of the tumor cells were darkly stained in the nucleus with eosinophilic staining in the cytoplasm. There were also individual cells with plasmacytoid appearance. In some areas, fine melanin granules exited in or out of the cells.
Immunohistochemical detection:Immunohistochemical (IHC) staining showed that the tumor cells were positive for MM markers human melanoma black 45 (HMB-45),Melan A, S-100 and vimentin, and negative for cytokeratin (pan), CD138, transcription termination factor 1, Napsin-A, Cytokeratin-7, P63, P40, synaptophysin,chromogranin-A, neuron-specific enolase, Desmin, CD99 and leukocyte common antigen (Figure 2). The positive rate of Ki67 was about 50%.
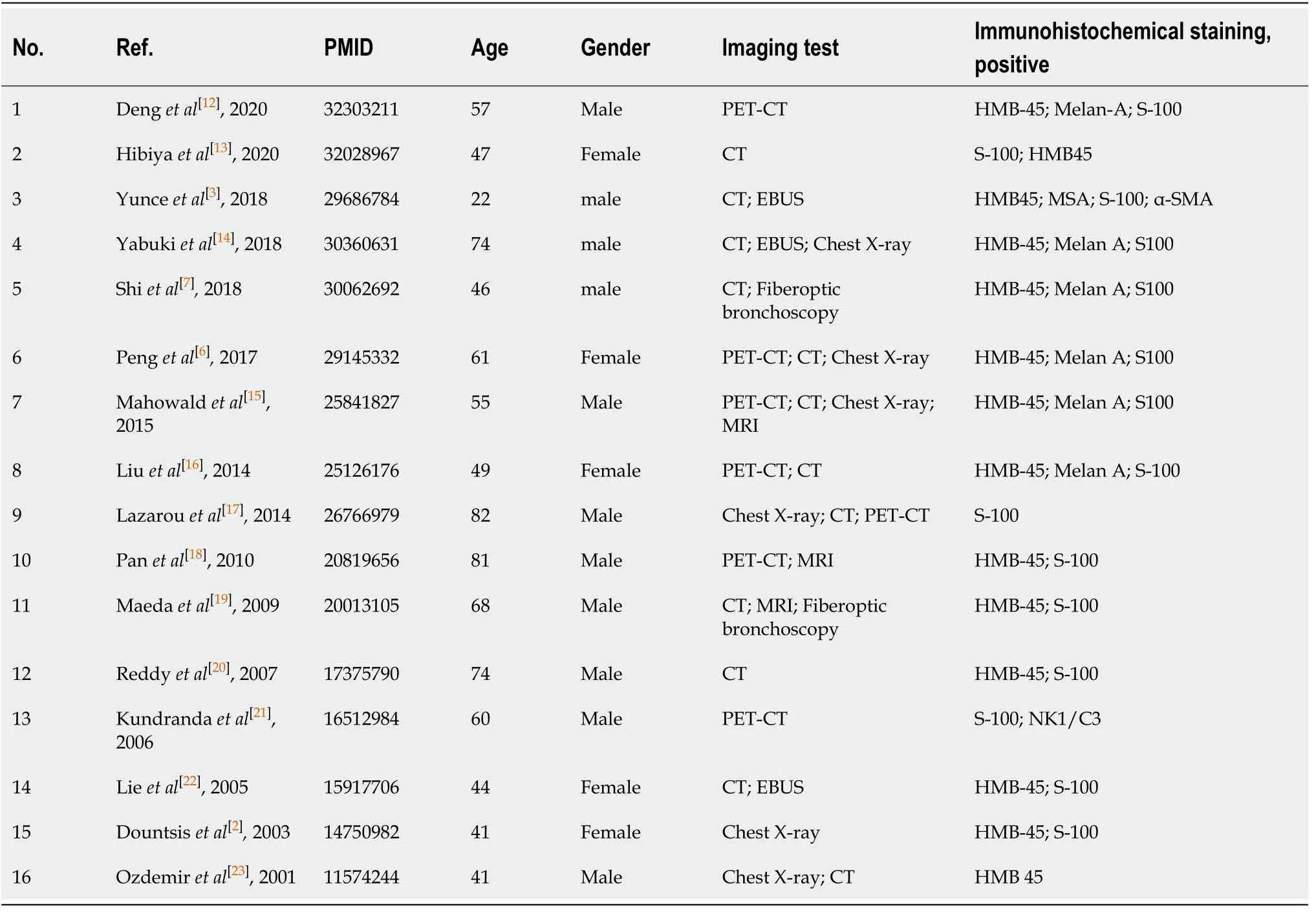
Table 1 Summary of the characteristics of primary malignant melanoma of the lung patients reported in previous case reports
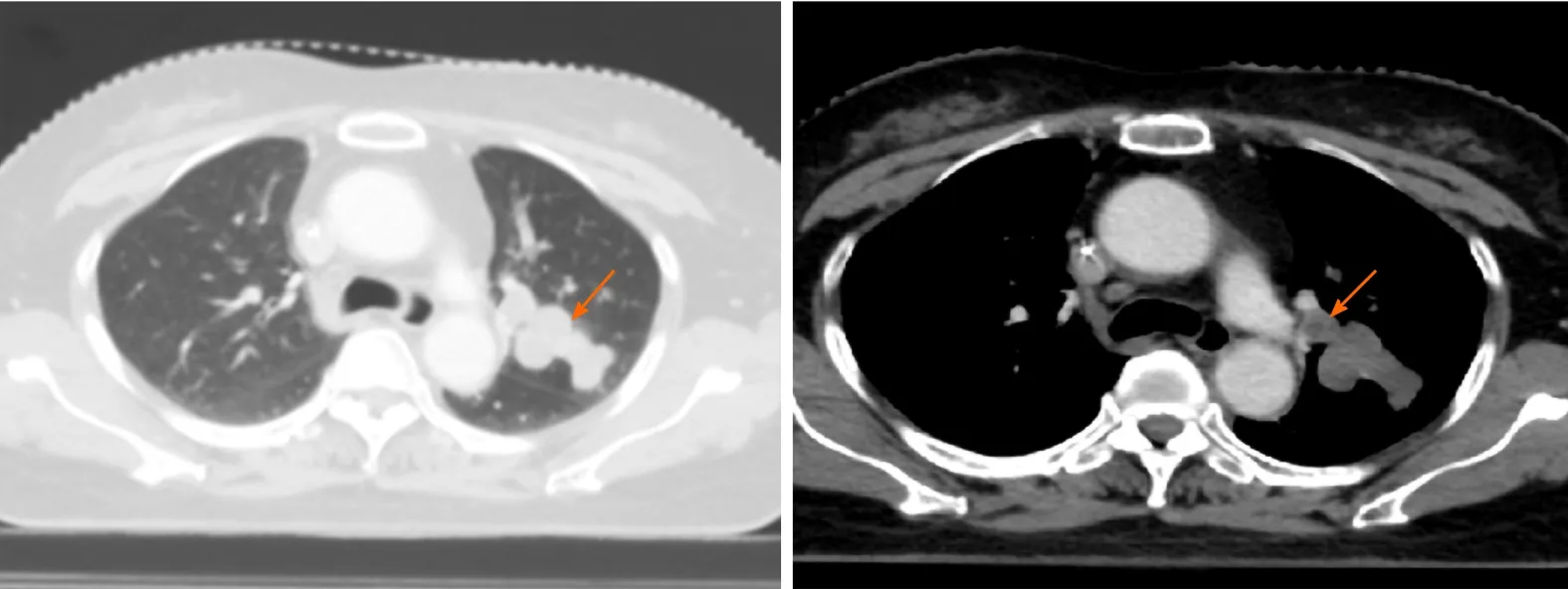
Figure 1 Computed tomography scan shows a large, space-occupying lesion in the Lingual lobe.
Imaging examinations
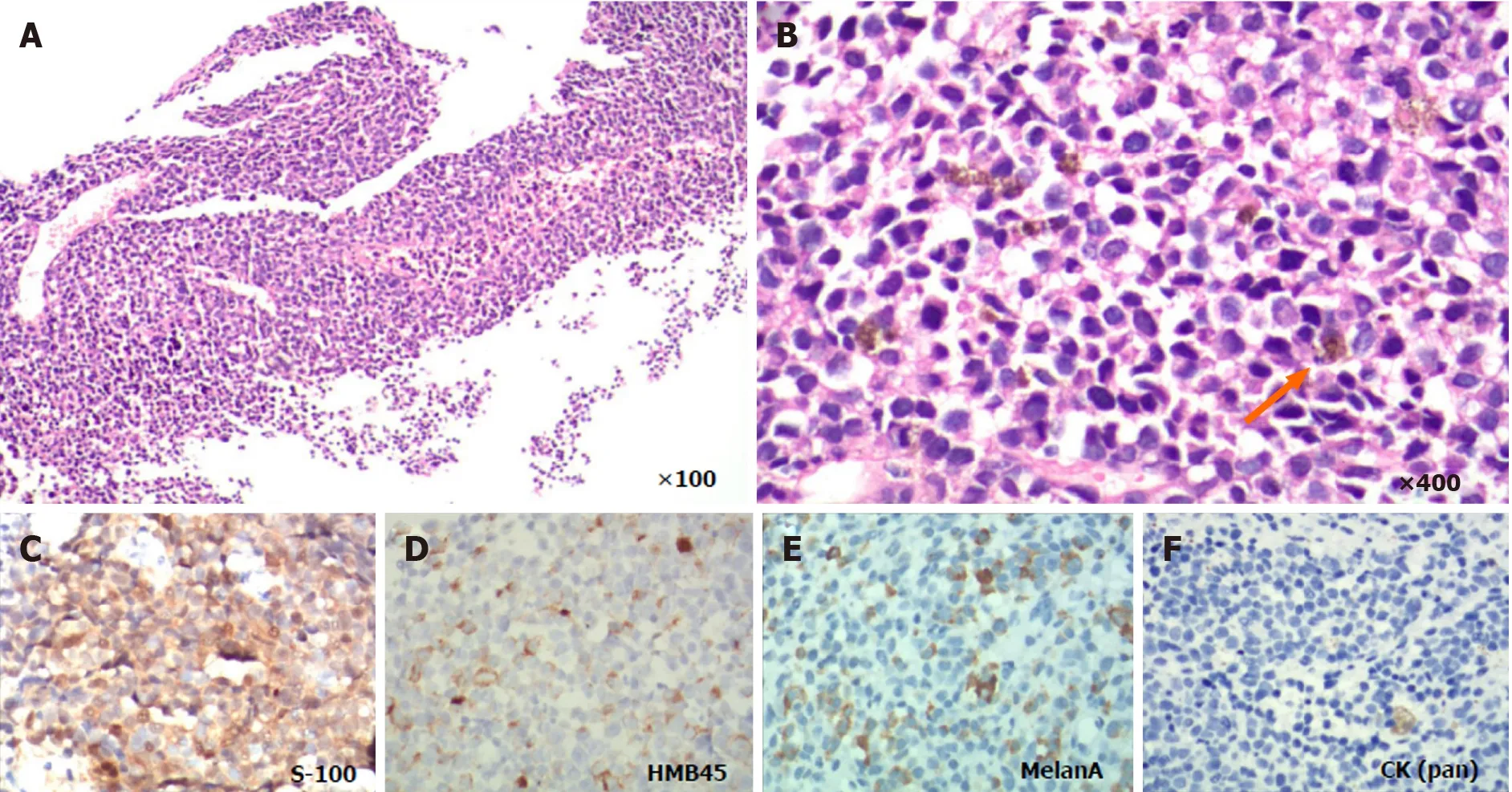
Figure 2 Microscopic examination of the tumor. A and B: Hematoxylin-eosin staining showing the histological feature of the tumor cells. Fine melanin granules exited in or out of the cells (orange arrow); C-E: Immunohistochemical results shown positive staining of human melanoma black 45, S-100 and Melan A,and negative staining of cytokeratin (pan); F: In biopsy tissue (image C-F is magnified 400 ×).
The patient underwent a CT scan of the lung, and the results showed a large, spaceoccupying lesion in the Lingual lobe. Positron emission tomography-CT (PET-CT)revealed multiple nodules located in superior lobe apicoposterior segment of her left lung. Nodules were partly integrated, well-demarcated and smooth. The largest nodule was 26 mm × 19 mm and irregular. The lesions were mostly accompanied with bronchus and lymph-vessel from peripheral to hilum of the lung. PET-CT also showed multiple left hilar lymph node metastases, and no metabolic abnormalities were detected in other parts of the body, including the head, neck, other parts of the chest,abdomen and pelvis. Brain magnetic resonance imaging showed numerous enhancing nodules, suggesting brain metastasis. The patient was clinically diagnosed with primary lung cancer. To obtain a specific pathological diagnosis, a CT-guided percutaneous biopsy of the lesions was performed, and then the small tissue samples were sent for pathological evaluation.
FINAL DIAGNOSIS
All of the aforementioned clinicopathological features were suggestive of PMML.
TREATMENT
Beginning in July 2019, the patient was given two cycles of chemotherapy TP regimen(paclitaxel 270 mg/m2intravenous (IV) on day 1 of a 21-d cycle) plus cisplatin (120 mg/m2IV on days 1-3 of a 21-d cycle) and taxotere and cyclophosphamide regimen(240 mg/m2IV on day 1 of a 21-d cycle) plus carboplatin (500 mg/m2IV on days 1-3 of a 21-d cycle). Four months later, the tumor had rapidly progressed, and the patient was treated with nivolumab (3 mg/kg every 2 wk.). About 1 mo later, the clinical reexamination confirmed the disease progression, and then oral imatinib was prescribed at 400 mg once daily for 4-wk cycles.
OUTCOME AND FOLLOW-UP
In February 2020, the patient was discharged, and it was recommended to continue imatinib anti-tumor therapy (data collection period was from November 2019 to February 2020) (Figure 3). No additional follow-up information was obtained from the patient at the time of manuscript writing.
DISCUSSION
MM usually occurs in the tissues where the melanocytes are located, such as skin,eyes, meninges, oropharynx, and anal canal, accounting for 1%-3% of malignant tumors[2]. Skin melanoma is the most common type of primary melanoma. The PMML is extremely rare, accounting for only 0.01% of all primary lung tumor[1,3]. The incidence of PMML is similar in male and female, and the mean age at diagnosis is 59.1 years (range from 29-90 years)[4,5]. The pathogenesis of PMML remains controversial[6,7]. At present, three hypotheses have been mainly proposed to explain the occurrence of PMML: (1) During embryotic development, melanocytes in the body can migrate not only into the epidermis and dermis of the skin but also into internal organs, such as esophagus, throat, brain, and lung; (2) Melanocytes may be transformed from bronchial gland in submucosa; and (3) Potential stem cells located in the lower respiratory tract can differentiate into melanocytes. Hence, those melanocytes can further develop into PMML.
However, PMML has no specific clinical symptom and can easily be misdiagnosed as tuberculosis or lung carcinoma. In addition, some primary skin MM can be metastasized, and then their primary lesions disappear, so it is quite difficult to diagnose primary or metastatic MM of lung[8]. The patient in this report presented common clinical manifestations, including recurrent cough and occasional hemoptysis,which were not specific from other respiratory infectious disease and lung tumors. The other clinical characteristics include no previously resected pigmented skin lesion.Unlike lung carcinoma, CT scan of this patient showed that the tumor was multinodular and well-demarcated, most of which was accompanied with tracheobronchial lymph nodes. Magnetic resonance imaging of the brain showed brain metastasis.Whole-body PET-CT revealed no lesions in other parts of the body. That is, there were no other detectable tumors at the time of diagnosis. The pathological diagnosis showed that the tumor cells had darkly stained nuclei and eosinophilic cytoplasm. In some areas, fine melanin granules exited in or out of the cells. The tumor cells were arranged in sheets, nests and a discohesive pattern and were accompanied by vessels.IHC staining showed that tumor cells were positive for the MM markers HMB-45 and Melan-A, which were valuable for the diagnosis of MM[2,3,6,7].
Genetic assays were also performed to identify the driver mutations. The results showed that theKITgene was mutated, and noEGFRgene mutation was found.Mutations in c-KITmostly occur in acral, mucosal, and chronically sun-damaged melanomas. As an important factor for cell differentiation, proliferation, and survival,c-KIThas been used in clinical trials of advanced melanoma to inhibit its function[9-11].Based on these findings, this case met the above diagnostic criteria and was diagnosed as PMML.
Although histologically it is difficult to distinguish PMML from lung squamous-cell carcinoma (SCC), it should be known that IHC staining of SCC is usually negative for HMB-45 and Melan-A. Primary melanoma often appears as a solitary nodule or mass,often involving the bronchial lumen.
A chest CT scan also can help find the abnormalities in the lungs. Usually, CT scan shows a mild or moderate enhancement of the PMML, which is different from the obvious enhancement of lung carcinoma. However, radiological detections cannot distinguish between primary and metastatic lesions. Therefore, it is necessary to ask medical history in detail (i.e.black spots and moles, skin ulcers and injuries) and to take physical examination of skin, mucosa, anal canal and vulva to check for pigmentation. Then, combined with the pathologic histology and immunophenotypic analysis of the tumor, PMML can be diagnosed.
Histopathological examination is still the gold standard for PMML diagnosis, but there are still many difficulties in the detection process. These include the difficulty to distinguish PMML from lung SCC. It should be known that IHC staining of SCC is usually negative for HMB-45 and Melan-A, and primary melanoma often appears as a solitary nodule or mass, often involving the bronchial lumen. Furthermore, when microscopic observation shows that the lesions are composed of small round cells and negative for carcinoma makers, the following points should be noted: Were the round cells morphologically diverse and diffusely distributed? Were tumor vessels pretty rich? Were tumor cells friendly to vessels? and were melanin granules inside or outside the tumor cell? If the answers are all yes, then MM may be taken into consideration. Consideration of MM should be verified by IHC staining of MM markers. Moreover, it is necessary to pay attention to the differential diagnosis of PMML and some diseases that are also composed of similar small round cells, such as lymphomas, extramedullary plasmacytoma, rhabdomyosarcoma and primitive neuroectodermal tumor.
CONCLUSION
PMML is an extremely rare, highly malignant neoplasm with a poor prognosis.Histopathological examination is a reliable gold standard for confirmation of a PMML diagnosis. Because of the morphological and immunophenotypic variations, the diagnosis of PMML remains difficult and should be distinguished from the diagnosis of other cancers. IHC staining is helpful for the differential diagnosis of PMML.Currently, with the in-depth study of the molecular biological characteristics and genetic variation of melanoma, targeted immunotherapy may further benefit clinical treatment and has broad prospects[12-23].
ACKNOWLEDGEMENTS
We thank the patient and her family for their support.
 World Journal of Clinical Cases2020年24期
World Journal of Clinical Cases2020年24期
- World Journal of Clinical Cases的其它文章
- Primary duodenal tuberculosis misdiagnosed as tumor by imaging examination: A case report
- Successful endovascular treatment with long-term antibiotic therapy for infectious pseudoaneurysm due to Klebsiella pneumoniae: A case report
- Idiopathic adulthood ductopenia with elevated transaminase only: A case report
- Takotsubo cardiomyopathy associated with bronchoscopic operation: A case report
- Extracorporeal shock wave therapy treatment of painful hematoma in the calf: A case report
- Rare case of drain-site hernia after laparoscopic surgery and a novel strategy of prevention: A case report