
Uncontrolled central hyperthermia by standard dose of bromocriptine: A case report
2020-04-07 06:17:32XinGeXueLuan
World Journal of Clinical Cases 2020年23期
Xin Ge, Xue Luan
Xin Ge, Department of Intensive Care Unit, Wuxi 9th Affiliated Hospital of Soochow University,Hand Institution of Wuxi City, Wuxi 214000, Jiangsu Province, China
Xin Ge, Traumatic Center, Wuxi 9th Affiliated Hospital of Soochow University, Hand Institution of Wuxi City, Wuxi 214000, Jiangsu Province, China
Xue Luan, Department of Neurosurgery, Central Hospital of Jinzhou, Jinzhou 121000, Liaoning Province, China
Abstract BACKGROUND Some patients present to the intensive care unit due to noninfectious pathologies resulting in fever, especially acute neurological injuries, including brain trauma and intracranial haemorrhage. The cause has been identified to be central hyperthermia characterized by a high core temperature and a poor response to antipyretics and antibiotics. However, no proper guidelines on how to treat central hyperthermia have been developed for clinical practice.CASE SUMMARY A 63-year-old woman was transferred to our hospital due to injury after a traffic accident. Eight hours after admission, her pupils enlarged bilaterally from 2.5 mm to 4.0 mm. She developed severe coma and underwent decompressive craniectomy. She was diagnosed with central hyperthermia after surgery and was prescribed bromocriptine. The standard dose of bromocriptine could not control her hyperpyrexia, and we prescribed 30 mg a day to control her temperature.CONCLUSION Bromocriptine may be effective in controlling central hyperthermia and have a dosage effect.
Key Words: Central hyperthermia; Bromocriptine; Side effect; Case report
INTRODUCTION
Fever has been reported to be a frequent complication in intensive care unit patients and associated with high mortality and unfavourable prognoses[1]. Noninfectious pathologies resulting in fever, especially acute neurological injuries such as brain trauma and intracranial haemorrhage, affect some patients. The cause has been identified as central hyperthermia, which is characterized by a high core temperature and a poor response to antipyretics and antibiotics[2]. Currently, no guidelines on how to treat central hyperthermia have been developed for clinical practice. However, a multimodal approach that includes the administration of additional medications, such as morphine, fentanyl, surface or intravascular cooling devices, and especially bromocriptine, has been reported[3]. A unique female patient who had central hyperthermia uncontrollable by a standard dose of bromocriptine was treated in our department. We prescribed 30 mg bromocriptine per day to control her hyperpyrexia.The results of a literature search suggest that a high dose of bromocriptine of 30 mg per day to treat central hyperthermia has not been previously reported.
CASE PRESENTATION
Chief complaints
A 63-year-old woman was transferred to our hospital due to injury after a traffic accident.
History of present illness
She was hit broadside, rolled off the car’s roof, and fell to the ground.
Physical examination
In the emergency room, the patient was in a moderate coma [Glasgow Coma Scale(GCS) score 9, E2V2M5]. However, 8 h later, her pupils enlarged bilaterally from 2.5 mm to 4.0 mm. The patient developed a coma (GCS: 6, E1V1M4) and received a computed tomography (CT) scan immediately. Unfortunately, an intracranial pressure monitor was not available in our centre, so a standard fronto-temporo-parietal decompressive craniectomy was performed.
Laboratory examinations
Most of laboratory examinations were normal.
Imaging examinations
The CT scan in the emergency department illustrated that there were specks of blood in the left frontal and temporal lobes and there was no midline shift (Figure 1). Eight hours later, repeat CT showed that the specks of blood in the left frontal and temporal lobes had become haematomas causing a 9 mm midline shift (Figure 2).
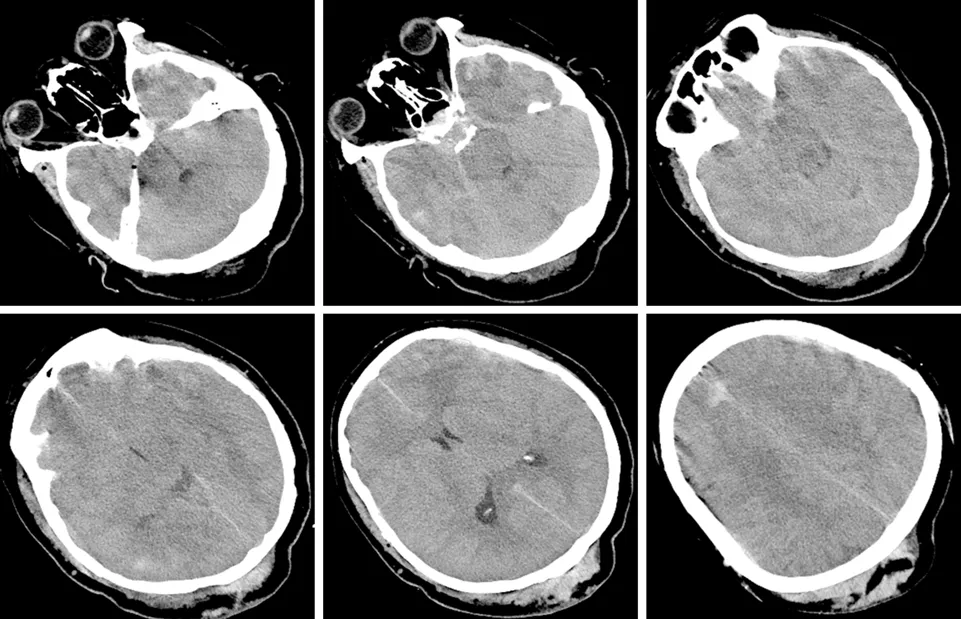
Figure 1 pecks of blood in the left frontal and temporal lobes.
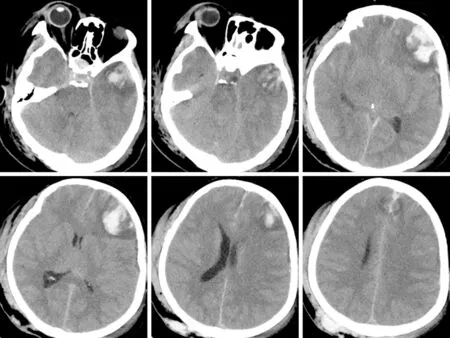
Figure 2 Haematomas in the left frontal and temporal lobes and 9 mm midline shift.
FINAL DIAGNOSIS
Central hyperthermia.
TREATMENT
We decided to increase the dose of bromocriptine. Five milligrams of bromocriptine three times a day was prescribed. Sixteen hours later, her temperature dropped to 37.5°C and remained at this level for a short time; 3 h later, her temperature increased again. This phenomenon was observed three times during the following day. The next day, after obtaining written informed consent from the patient's legally authorized representative, we prescribed 5 mg bromocriptine six times a day. As expected, her temperature dropped to 36.5 °C and remained at this temperature, but her heart rate declined from 95 to 57 per min, and her blood pressure decreased. Five days after her temperature was controlled, we attempted to decrease the dose of bromocriptine to 5 mg four times a day but failed. Her temperature rose again to 40.1 °C and dropped to 38.0 °C for 3 to 4 h. We resumed the previous dose, and her temperature became stable. The side effects of the drug included declines in her heart rate and blood pressure. Her heart rate had decreased to 41 per min but remained stable with vasoactive drugs. Seven days later, we tried to decrease the dose of bromocriptine and failed again. Six weeks after surgery, when bromocriptine had been administered for 34 d, we decreased the dose and managed to successfully stop administration within 2 wk (Figure 3).
OUTCOME AND FOLLOW-UP
Eight weeks after surgery, her GCS score was 5 (E1VTM3). She underwent a magnetic resonance imaging (MRI) scan, which illustrated speck signals in the midbrain,pontine, and pituitarium and multiple damage signals in the left frontal, temporal, and occipital lobes, basal ganglia, thalamus, and corpus callosum (Figure 4). The MRI findings were supportive of the diagnosis of diffuse axonal injury (DAI). She was sent to rehabilitation center. The GCS score was 8 (E3VTM4) 6 mo later.
DISCUSSION
An elevated temperature affects not only the brain but also other organs and may increase the risk of mortality[4]. A noninfectious pathology resulting in fever in a patient with severe TBI is not uncommon, and it is known as neurogenic fever[5].Neurogenic fever is characterized by symptoms of hyperthermia, tachycardia,hyperhidrosis, hypertension, and sometimes seizures, which are referred to as dysautonomia or paroxysmal sympathetic hyperactivity or diencephalic syndrome[6].However, the symptoms of tachycardia, hyperhidrosis, and hypertension were not found in this patient. A previous study indicated that the characteristics of central hyperthermia may be due to the compression of hypothalamic and brainstem thermoregulatory centres[7]. Some areas, including the preoptic area of the hypothalamus, inputs from spinothalamocortical relay pathways, and the lateral parabrachial nucleus at the junction of the pons and medulla, may regulate the thermo-regulating centres[8].
In this case study, the MRI findings confirmed the diagnosis of DAI. DAI is a rotational acceleration-deceleration traumatic brain injury due to strain or shearing forces. DAI has three distinctive structural features[9]: (1) Diffuse supratentorial damage to axons (grade I); (2) A focal lesion in the corpus callosum (grade II); and (3)A focal lesion or lesions in the rostral brain stem (grade III). Therefore, this patient represents a severe case because the MRI scan showed all of these features.Hypothalamus injuries have been associated with autonomic dysfunction symptoms observed in DAI cases[9]. The compression of the hypothalamus and brainstem may result in the deregulation of the selective loss of warm-sensitive neurons, progesterone or prostaglandin hormonal changes leading to modifications in the firing rate of heatsensitive neurons in the medial preoptic nucleus, or osmotic changes detected by the organum vasculosum laminae terminalis[10]. Bromocriptine is a dopamine D2 agonist drug that acts on the hypothalamus and the corpus striatum. Its efficacy in the treatment of central hyperthermia[3]and paroxysmal sympathetic hyperactivity[11]has been reported in previous studies because of its effects on dopaminergic transmission.A dose of 7.5 mg per day has been reported and indicated to be effective[3]. We tried to prescribe the same dose to control central hyperthermia but failed. On the basis of the clinical findings, we increased the dose to 30 mg per day, which was successful. The side effects of bromocriptine at high doses during treatment were bradycardia and hypotension. It was found that the higher the dosage of bromocriptine, the worse the bradycardia and hypotension. We used vasoactive drugs such as atropine and norepinephrine to stabilize hemodynamics in patients and succeeded. We attempted to decrease the dose of bromocriptine twice but failed due to severe side effects.Therefore, we conclude that both the effect of bromocriptine in controlling hyperpyrexia and the dosage effect were demonstrated in this study.
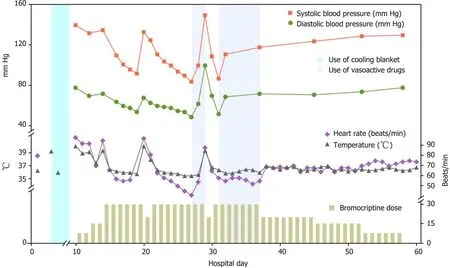
Figure 3 Fluctuations of marked temperature, blood pressure, heart rate, and dose of bromocriptine and treatments with cooling blanket and vasoactive drugs were noted during the clinical course.
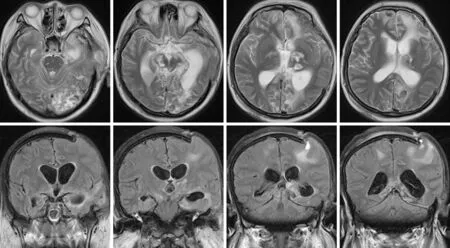
Figure 4 Speck signals in the midbrain, pontine, and pituitarium and multiple damage signals in the left frontal, temporal and occipital lobes, basal ganglia, thalamus, and corpus callosum.
CONCLUSION
This case report demonstrates that bromocriptine may be used to control central hyperthermia, and the dose may affect the clinical effect. Central hyperthermia caused by severe DAI can be treated with high doses of bromocriptine. Side effects should be considered and, if required, managed with vasoactive drugs.
ACKNOWLEDGEMENTS
The authors would like to thank the patient and her family.
 World Journal of Clinical Cases2020年23期
World Journal of Clinical Cases2020年23期
- World Journal of Clinical Cases的其它文章
- Novel triple therapy for hemorrhagic ascites caused by endometriosis: A case report
- Discontinuous polyostotic fibrous dysplasia with multiple systemic disorders and unique genetic mutations: A case report
- Primary breast cancer patient with poliomyelitis: A case report
- Symptomatic and optimal supportive care of critical COVID-19: A case report and literature review
- Multiple ectopic goiter in the retroperitoneum, abdominal wall, liver,and diaphragm: A case report and review of literature
- Acute celiac artery occlusion secondary to blunt trauma: Two case reports