
Treatment of Kümmell’s disease with sequential infusion of bone cement: A retrospective study
2020-04-07 06:17XingZhangYongChaoLiHongPengLiuBingZhouHuiLinYang
World Journal of Clinical Cases 2020年23期
Xing Zhang, Yong-Chao Li, Hong-Peng Liu, Bing Zhou, Hui-Lin Yang
Xing Zhang, Hui-Lin Yang, Department of Orthopaedics, The First Affiliated Hospital of Soochow University, Suzhou 215006, Jiangsu Province, China
Xing Zhang, Hong-Peng Liu, Bing Zhou, Department of Orthopaedics, Gaoyou People’s Hospital Affiliated to Soochow University, Yangzhou 225600, Jiangsu Province, China
Yong-Chao Li, Department of Spinal Surgery, Shanghai East Hospital, Tongji University School of Medicine, Shanghai 200120, China
Abstract BACKGROUND Percutaneous vertebroplasty (PVP) is an effective method for the treatment of neurologically intact Kümmell’s disease, but bone cement leakage during surgery is a problem that deserves attention.AIM To reduce bone cement leakage and evaluate the effect of the sequential infusion of bone cement during PVP for the treatment of stage I or II Kümmell’s disease.METHODS Patients with Kümmell’s disease treated in our hospital from September 2015 to September 2018 were retrospectively analyzed. Patients meeting the inclusion and exclusion criteria were divided into two groups: Traditional single infusion and sequential infusion (SI). The visual analog scale (VAS) and Oswestry disability index (ODI) were evaluated and compared, and duration of operation, bone cement content and complications were recorded.RESULTS Forty-five patients were included in this study; there were 24 in the traditional single infusion group and 21 in the SI group. The VAS and ODI were significantly different for both groups when compared pre- and postoperatively, whereas the differences between 1 wk postoperatively and at the final follow-up were not statistically. When the VAS and ODI of the two groups were compared, there were no significant differences at any time point. The leakage rate of bone cement was significantly lower in the SI group (14.3%, 3 of 21) than that in the traditional single infusion group (41.7%, 10 of 24).CONCLUSION SI in unipedicular PVP is a safe and effective procedure for neurologically intact Kümmell’s disease, and this technique could decrease the incidence of bone cement leakage.
Key Words: Kümmell’s Disease; Percutaneous vertebroplasty; Bone cement leakage; Back pain; Osteoporosis; Intravertebral vacuum cleft
INTRODUCTION
Kümmell, in 1895, first described the triad of back pain, gradual collapse of the vertebrae and progressive kyphosis following an asymptomatic period of mild vertebral fracture[1-3]. Patients who present with low back pain are treated with percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP), which can effectively alleviate clinical symptoms and prevent continuous vertebral collapse and neurological impairment[4-7]. Although PKP can restore vertebral height with less risk of leaking bone cement, it is cost prohibitive to many patients, especially in developing countries[7]. In patients with intact neurological function who undergo PVP,intraoperative bone cement leakage into blood vessels can cause pulmonary artery embolism or death, and leakage into the spinal canal can compress the spinal cord or nerve roots causing severe pain or even paralysis[5]. Therefore, a safe and effective bone cement infusion technique is essential during PVP. To reduce bone cement leakage, we adopted a sequential infusion of bone cement during PVP for the treatment of stage I or II Kümmell’s disease.
MATERIALS AND METHODS
Patient selection
Patients with Kümmell’s disease treated in our hospital from September 2015 to September 2018 were analyzed retrospectively. Patients were included if they met the following criteria: (1) Age ≥ 55 years with T5-L5 vertebral fractures; (2) Progressive back pain and kyphosis after an asymptomatic or mild symptomatic period regardless of history of mild spinal trauma; (3) Vertebral collapse, intravertebral vacuum cleft sign and intravertebral pseudoarthrosis demonstrated on X-ray and computed tomography and “liquid sign” and “double contour sign” on magnetic resonance imaging; (4) Meet the diagnostic criteria for osteoporosis (World Health Organization),including L1-L4 bone mineral density T value < -2.5 on dual-energy X-ray; (5) Stage I and II Kümmell’s disease based on staging criteria proposed by Liet al[8]; (6) Fractures in a single vertebral segment and receiving PVPviaa unilateral pedicle approach; and(7) Complete initial and follow-up data.
Patients were excluded if they met the following criteria: (1) Severe medical or psychiatric disease; (2) Fresh vertebral fractures; (3) Other pathological fractures such as hemangioma, multiple myeloma and tuberculosis; (4) Neurological signs such as stage III Kümmell’s disease; and/or (5) Coagulopathies. Based on the different ways of bone cement injection, patients were then divided into two groups: Traditional single infusion (TSI group) and sequential infusion (SI group, graded infusion of bone cement into the vertebra). All operations were performed by the same experienced surgeon (Zhang X).
Surgical procedure
Under digital subtraction imaging (DSA) fluoroscopy, a conventional unilateral(mainly left side) pedicle approach was used to complete PVP surgery. The operation time, bone cement content and complications were recorded.
For the TSI group, the bone cement was prepared into a filiform shape and slowly infused into the diseased vertebra under low pressure under DSA. However, in the SI group, the bone cement was prepared and infused twice into the vertebra. First, the bone cement was prepared into a late-phase filiform or early-phase mass shape and slowly infused under DSA to prevent breakage at the anterior edge of the diseased vertebra. We observed that the bone cement gradually filled the entire vertebral fracture from the outflow end without much resistance. Second, the bone cement was prepared into an early- or midphase filiform shape and infused. We observed that the bone cement adhered to the previous cement and diffused into the vertebral trabecular space until thorough diffusion was achieved.
Postoperative outcomes
On postoperative day 1, patients were able to get out of bed with waist support, and bisphosphonates and vitamin D were started to prevent osteoporosis. Patients were encouraged to get sun exposure and exercise. On the second postoperative day, bone cement leakage was evaluated using X-ray according to the method described by Wanget al[9]. On direct postoperative images, the patterns of cement leakage were classified as five types: Type A, through a cortical defect into the paraspinal soft tissues; type B, through the basivertebral foramen; type C,viathe needle channel; type D, through a cortical defect into the disc space; and type E,viathe paravertebral vein[9]. Patients evaluated their degree of symptom relief and improvement in activities of daily living using a visual analogue scale (VAS) and Oswestry disability index(ODI) preoperatively, 1 wk postoperatively and at their last follow-up appointment.
Statistical analysis
The SPSS 20.0 statistical software (SPSS Inc.; Chicago, IL, United States) was used for data analysis. Normally distributed data were expressed as mean ± standard deviation and compared using at-test or analysis of variance. Data not normally distributed were expressed as medians (minimum, maximum)] and compared using the Mann-Whitney U test. Frequency data were expressed as percentages and compared using a Chi-square test or Fisher’s exact test. Differences with aPvalue < 0.05 were considered statistically significant.
RESULTS
Forty-five patients were included in this study; this included 24 in the TSI group and 21 in the SI group. Preoperatively, all patients had chronic back pain that could not be relieved by bed rest and medical management. The baseline data in both groups are shown in Table 1. There were no significant differences in measurement indices between groups (P> 0.05).
Surgery was successful in all patients, and none experienced severe complications such as pulmonary embolism or spinal nerve injury. The median operation time was significantly lower in the TSI group than in the SI group (30 minvs37 min, Mann-WhitneyUtest,P= 0.000). The bone cement was 4.5 (3.0, 5.5) mL in the TSI group and 4.0 (3.0, 5.5) mL in the SI group (Mann-WhitneyUtest,P= 0.490). The median followup period was 26 (14, 48) mo in the TSI group, and 26 (13, 49) mo in the SI group.There was no difference in follow-up duration across groups (Mann-WhitneyUtest,P= 0.741).
The VAS and ODI were significantly different for both groups when compared preand postoperatively (P< 0.05; Table 2), whereas the differences between 1 wk postoperatively and at the final follow-up were not statistically significant (P>0.05;Table 2). When the VAS and ODI of the two groups were compared, there were no significant differences at any timepoint (P> 0.05; Table 2).
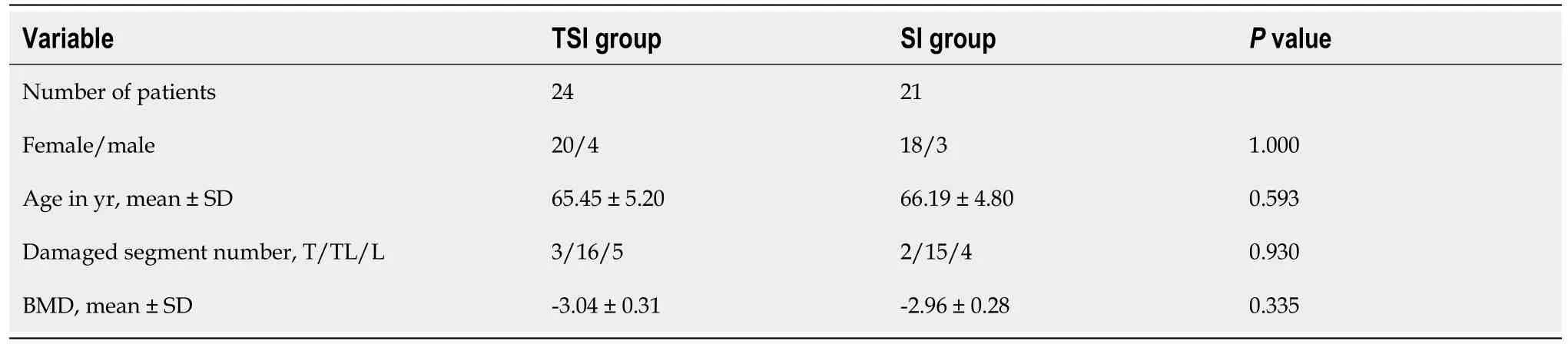
Table 1 The baseline data in both groups

Table 2 Visual analog scale and Oswestry disability index before and after surgery
In the TSI group, the total leakage rate of bone cement was 41.7%. There were four cases of leakage into the paravertebral soft tissueviathe bone cortical defect, two cases of basivertebral foramen leakage and four cases of intervertebral disc space leakage,without obvious clinical symptoms. In the SI group, the total leakage rate of bone cement was 14.3%. There were three cases of intervertebral disc space leakage, without obvious clinical symptoms. The leakage rate of bone cement was lower in the SI group than in the TSI group (Pearson chi-squared test,P= 0.043).
DISCUSSION
Even though Kümmell’s disease is common and has low morbidity when recognized,it often remains undiagnosed because it is mistaken as osteoporotic vertebral compression fractures. Kümmell’s disease was actually not accepted as a condition until 1951 when delayed vertebral collapse was discovered on X-ray[10]. With the widespread use of imaging, increasingly more clinicians have begun to diagnose the disorder and report it[5,11-14].
Kümmell’s disease develops progressively. The vertebral body is intact or slightly fractured in the early stage, vertebral collapse and instability occur in the middle stage and there is obvious vertebral collapse and progressive kyphosis in the later stage[1-3,14].In this study, patients in both groups had chronic disease, and they still had persistent back pain after nonsurgical treatment. Nonsurgical managements such as analgesia,immobilization and bed rest are ineffective for Kümmell’s disease, and long-term bed rest is also harmful to elderly patients. Therefore, surgical intervention should be performed as early as possible for patients with Kümmell’s disease to prevent further vertebral collapse and kyphosis.
With the development of minimally invasive spinal surgery, PVP and PKP have gradually been used in the treatment of Kümmell’s disease to stabilize the vertebral body and decrease pain[4-7]. In this study, Kümmell’s disease was treated with PVPviathe vertebral pedicle unilaterally in both groups, achieving satisfactory clinical efficacy. The VAS and ODI were significantly different in both groups pre- and postoperatively. At the final follow-up, the VAS and ODI were not significantly different in either group compared with those at 1 wk postoperatively. The two groups were not significantly different for the VAS and ODI pre- and postoperatively or at the final follow-up. These results demonstrate that both sequential infusion and one-time infusion of bone cement can effectively stabilize the vertebral body and eliminate the micromovement of the fracture block, leading to a positive analgesic effect.
During the PVP operation, bone cement leakage into blood vessels can cause pulmonary artery embolism or death, and leakage into the spinal canal can compress the spinal cord or nerve roots causing severe pain or even paralysis[5]. Therefore, it is of great significance to reduce and avoid bone cement leakage during PVP surgery.Compared with osteoporotic vertebral compression fractures, the main complication of treating Kümmell’s disease with PVP is bone cement leakage, with the leakage rate being far higher than in patients with osteoporotic vertebral compression fractures without Kümmell’s disease[6]. Pehet al[5]reported that the leakage rate of bone cement in PVP for Kümmell’s disease can be up to 79%, which may be related to vertebral rupture. Haet al[6]demonstrated that in the treatment of osteoporotic vertebral fracture patients with an intravertebral cleft sign, the leakage rate of bone cement in PVP is 75%.
The vertebral anterior wall is mostly ruptured in Kümmell’s disease, so bone cement leakage occurs easily in PVP. In order to prevent bone cement leakage from the rupture point of the vertebral anterior wall and improve the safety of surgery, we performed sequential infusion and found that the leakage rate of bone cement was significantly lower (14.3%) than that in TSI group (41.7%). In the SI group, there were three cases of bone cement leakage but not from the rupture mouth at the anterior edge of the vertebral body, suggesting that the graded infusion of bone cement can effectively prevent bone cement leakage from the rupture mouth of the vertebral anterior wall. In the SI group, the push rod was pressed as closely as possible to the fracture at the anterior edge of the vertebral body, and the higher viscosity bone cement was slowly infused to first block the fracture. Then the lower viscosity bone cement was infused so that it could disperse in the vertebral body. However, the operation time in the SI group was longer than in the TSI group. In addition, the leakage rate of bone cement in both groups was lower than reported in the literature,and the possible reason is that the infusion of bone cement was continuously monitored with the aid of DSA.
In patients with Kümmell’s disease, there are liquid or gas cavities in the vertebral body. During infusion, the bone cement can flow freely without resistance and fill the entire cavity symmetrically. In this study, therefore, the bone cement was infused into the entire vertebral bodyviathe unilateral vertebral pedicle without bilateral puncture.
Wanget al[15]reported a case of delayed bone cement displacement after treatment of Kümmell’s disease with PKP, leading to progressive back pain. The possible reason for the displacement is that rupture and collapse of loose trabecular bone may have occurred during balloon dilatation, forming high-density bone. In the secondary infusion, the bone cement may have poorly dispersed and failed to adhere, resulting in bone cement displacement. In this study, there was no displacement of the bone cement in either of the two groups, which may have been due to diffusion into the honeycomb-shaped bone during PVP so that the bone cement was firmly fixed in the vertebral body.
A limitation of this study is that it is retrospective and may be prone to selection bias. However, bias is limited through strict inclusion and exclusion criteria and matching of patients. Second, the sample size was small and the follow-up period was short in both groups. Finally, the specific condition of bone cement leakage after PVP was not evaluatedviacomputed tomography imaging.
CONCLUSION
This study indicates that sequential infusion in unipedicular PVP is a safe and effective procedure for neurologically intact Kümmell’s disease. This technique could decrease the incidence of bone cement leakage.
ARTICLE HIGHLIGHTS
Research background
Percutaneous vertebroplasty (PVP) is an effective method for the treatment of neurologically intact Kümmell’s disease, but bone cement leakage during surgery is a problem that deserves attention.
Research motivation
To reduce bone cement leakage and evaluate the effect of the sequential infusion of bone cement during PVP for the treatment of stage I or II Kümmell’s disease.
Research objectives
To compare the clinical effect of sequential bone cement infusion and traditional bone cement infusion in the treatment of stage I or II Kümmell’s disease.
Research methods
Patients with Kümmell’s disease treated in our hospital from September 2015 to September 2018 were retrospectively analyzed. Patients meeting the inclusion and exclusion criteria were divided into two groups: Traditional single infusion (TSI group) and sequential infusion(SI group). The visual analog scale (VAS) and Oswestry disability index (ODI) were evaluated and compared, and duration of operation, bone cement content and complications were recorded.
Research results
Forty-five patients were included in this study, 24 in the TSI group and 21 in the SI group. The VAS and ODI were significantly different in both groups pre- and postoperatively. At the last follow-up, the VAS and ODI were not significantly different between the two groups compared with those at 1 wk postoperatively. The two groups had no significant differences in the VAS and ODI pre- and postoperatively and at the last follow-up. The leakage rate of bone cement was significantly lower in the SI group (14.3%, 3 of 21) than that in the TSI group (41.7%, 10 of 24).
Research conclusions
Sequential infusion in unipedicular PVP is a safe and effective procedure for neurologically intact Kümmell’s disease, and this technique could decrease the incidence of bone cement leakage.
Research perspectives
The role of sequential infusion in reducing the leakage of bone cement should be evaluated in a large sample multicenter randomized controlled study.
 World Journal of Clinical Cases2020年23期
World Journal of Clinical Cases2020年23期
- World Journal of Clinical Cases的其它文章
- Understanding the immunopathogenesis of COVID-19: Its implication for therapeutic strategy
- What is the gut feeling telling us about physical activity in colorectal carcinogenesis?
- Latest developments in chronic intestinal pseudo-obstruction
- Correlation between ductus venosus spectrum and right ventricular diastolic function in isolated single-umbilical-artery foetus and normal foetus in third trimester
- Clinical efficacy of integral theory–guided laparoscopic integral pelvic floor/ligament repair in the treatment of internal rectal prolapse in females
- Application value analysis of magnetic resonance imaging and computed tomography in the diagnosis of intracranial infection after craniocerebral surgery