
Advances and challenges in immunotherapy of small cell lung cancer
2020-03-13 07:29:46HanfeiGuoLingyuLiJiuweiCui
Hanfei Guo,Lingyu Li,Jiuwei Cui
Cancer Center,The First Hospital of Jilin University,Changchun 130021,China
Abstract Small cell lung cancer (SCLC) is a highly lethal disease,characterized by early metastasis and rapid growth,and no effective treatment after relapse.Etoposide-platinum (EP) combination has been the backbone therapy of SCLC over the past 30 years.It is extremely urgent and important to seek new therapies for SCLC.In the past 5 years,immunotherapy,such as immune checkpoint inhibitors programmed cell death protein-1 (PD-1),cytotoxic T lymphocyte associatedprotein-4 (CTLA-4),has made remarkable achievements in the treatment of patients with SCLC,and it has become the first-line option for the treatment of some patients.Some traditional chemotherapeutic drugs or targeted drugs,such as alkylating agent temozolomide and transcription inhibitor lurbinectedin,have been found to have immunomodulatory effects and are expected to become new immunotherapeutic agents.In this study,we aimed to review the efficacy of new treatments for SCLC and discuss the current challenges and application prospect in the treatment of SCLC patients.
Keywords:Small cell lung cancer (SCLC);immunotherapy;immune checkpoint inhibitors
Introduction
Small cell lung cancer (SCLC) is a poorly differentiated and high-grade neuroendocrine tumor,which accounts for 10%−15% of all lung cancers (1,2).SCLC is characterized by short tumor doubling time (TDT) and metastasis at an early stage.More than half of the patients were diagnosed at extensive disease (ED) (2,3).Chemotherapy combined with chest radiotherapy has been considered as a standard treatment for SCLC patients for the past 50 years (4).Although SCLC patients are still sensitive to current therapy,with an objective response rate (ORR) of 70%,quite a lot of patients develop drug resistance or disease relapse rapidly after remission (4).The median overall survival (OS) is 15−20 months with limited disease (LD)-SCLC and 8−13 months with ED-SCLC (3,5,6).
Current research suggests that the immune system plays a key role in controlling tumor growth and progression,a process known as cancer immune surveillance.Tumors can escape from immune surveillance by inducting regulatory T cells (Tregs) to promote dysfunctions of T cells and natural killer (NK) cells (7).Such immunosuppressive state is observed in patients with SCLC,which can influence the prognosis of these patients (8).For example,inflammation reduction in pre-existent T-cell occurs more commonly in SCLC than in non-SCLC (NSCLC) (9).Immunotherapy may be a new hope for SCLC patients by reversing the immunosuppressive status.Preclinical and clinical trials on immune checkpoint inhibitors and adoptive cell therapy have heralded a new era in the treatment of SCLC.Cellular immunotherapy (CIT),tumor vaccines,and immunomodulators are also being studied.However,there are still challenges that need to be addressed.Seeking biomarkers to achieve precise treatment is also underway(Figure 1).
Immune checkpoint inhibitors
Cytotoxic T lymphocytes (CTLs) is the main force in anticancer immune response (10).In the tumor microenvironment,the immune checkpoint pathway is often overactive and then contributes to an immunosuppressive state.The receptors of immune checkpoint on immune cells,such as the CTL-associated protein 4 (CTLA-4) (11),and programmed-death 1 (PD-1),when engaged by their ligands,CD80/CD86 and PD-L1/PD-L2,respectively,can transmit an inhibitory signal,maintain self-tolerance,and discontinue anti-tumor immune responses (12).The aberrant expression of PD-L1 was reported in 72% of patients with SCLC,which was significantly correlated with LD,and was shown to be an independent predictor for favorable outcome (13).The utilization of immune checkpoint inhibitors can effectively restore and augment CTLs responses,leading to potential anti-tumor immune responses,which is of intriguing interest (14).
Clinically,seven immune checkpoint inhibitor antibodies have been approved by the United States Food and Drug Administration (FDA) for the treatment of a variety of tumors:ipilimumab that blocks cytotoxic T-lymphocyte antigen-4 (CTLA-4),and six antibodies that block PD-1/PD-L1 including pembrolizumab,nivolumab,atezolizumab,durvalumab,cemiplimab and avelumab.To date,the immune checkpoint inhibitors have achieved a promising result in the treatment of recurrent SCLC(Table 1).
Checkpoint inhibitor as first-line treatment for SCLC
IMpower133 is an international,double-blind,randomized,placebo-controlled phase III study that recruited 403 patients from 22 countries to evaluate the efficacy and safety of carboplatin and etoposide combined with atezolizumab as a first-line treatment of ED-SCLC.The median OS was 12.3 months in the atezolizumab group and 10.3 months in the placebo group [hazard ratio (HR)],0.70;95% confidence interval (95% CI),0.54−0.91;P=0.007],while the median progression-free survival (PFS) was 5.2 months and 4.3 months,respectively (HR,0.77;95% CI,0.62−0.96;P=0.02) (15).In the IMpower133 trail,atezolizumab group extended the median OS by 2 months and the median PFS by 0.9 months,immune-related adverse effects (AEs) were more common in the atezolizumab group compared with the placebo group(39.9%vs.24.5%),including rash,hepatitis,fluid-related reactions,pneumonia and colitis.It is the only FDAapproved treatment of SCLC for more than 20 years and is a landmark development in the history of SCLC treatment.However,we need to be aware that the data of OS and PFS gained in IMpower133 were very limited,though significant.In this study the crossover was not allowed and the experimental arm received post-induction maintenance.
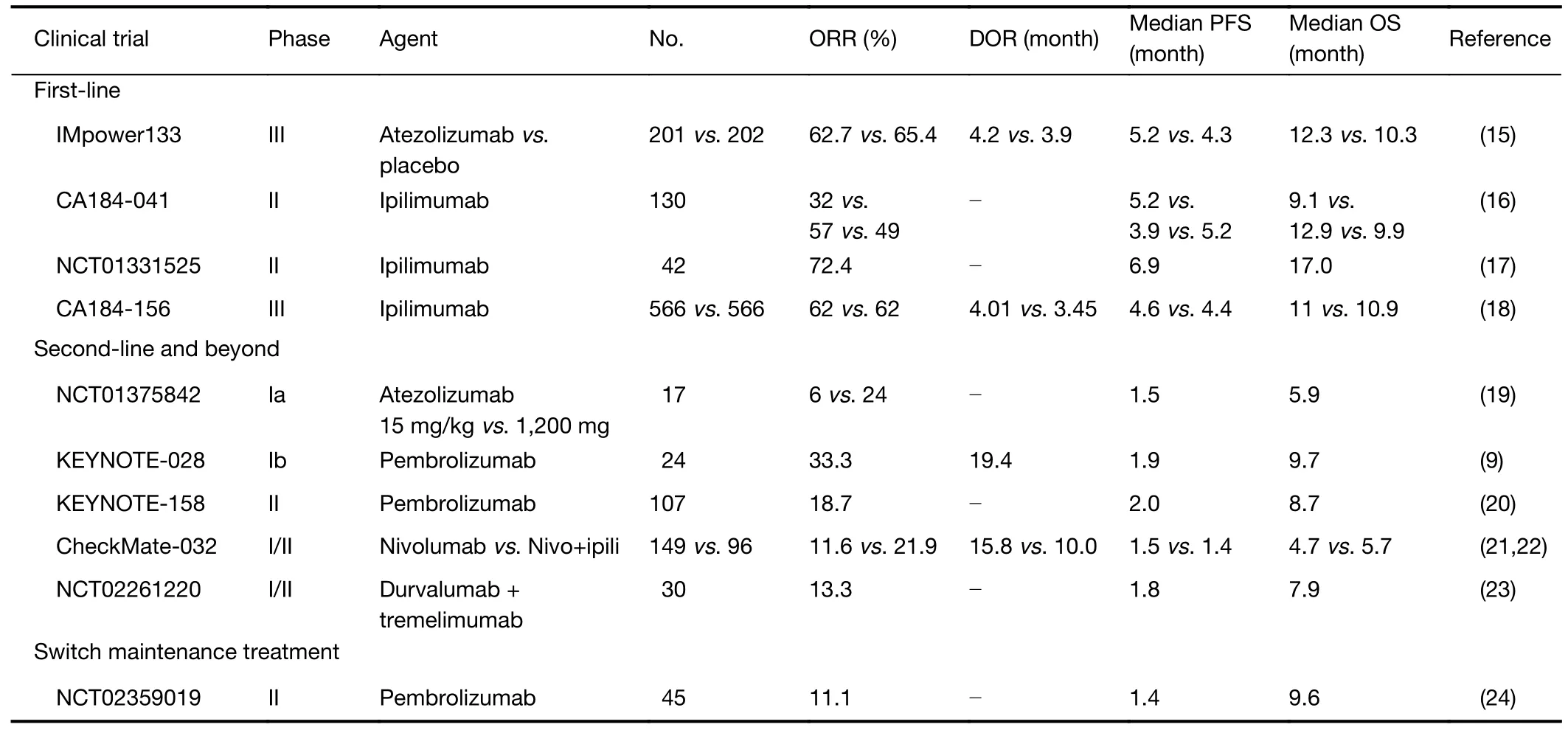
Table 1 Completed clinical trials of immune checkpoint inhibitors in SCLC
A phase II study (CA184-041),which enrolled 130 patients,evaluated the safety and efficacy of ipilimumab in combination with paclitaxel and carboplatin:the median PFS of control,concurrent,and ipilimumab group were 5.2,3.9 and 5.2 months,respectively;the median OS for all three cohorts were 9.9,9.1 and 12.9 months,respectively(16).In another phase II study (NCT01331525),which enrolled 42 patients,ipilimumab in combination with carboplatin and etoposide was used as a first-line treatment for patients with ED-SCLC;the median PFS was 6.9 months,while the median OS was 17.0 months (17).A confirmatory phase III study (CA184-156) showed that ipilimumab in combination with chemotherapy (EP regimen) as a first-line treatment for ED-SCLC,failed to improve OS,PFS,and ORR compared with chemotherapy alone (18).
A phase III trial CASPIAN (NCT03043872) showed that first-line durvalumab plus platinum-etoposide significantly improved OS in patients with ES-SCLCvs.a clinically relevant control group (HR,0.73;95% CI,0.59−0.91;P=0.0047).Safety findings were consistent with the known safety profiles of all drugs received (25).
Radiation can lead to apoptosis of tumor cells,and it can expose the immune system to additional antigens and partially reshape the tumor microenvironment by reducing the number of mesenchymal-derived suppressor cells(26,27),thereby activating the local anti-tumor immune response.Therefore,combination of immunotherapy and radiotherapy is a reasonable strategy for the cancer therapy.
A number of clinical studies have been conducted to further determine the safety and clinical activity of immune checkpoint inhibitors as a first-line treatment for SCLC,including pembrolizumab (KEYNOTE-604,KEYNOTE-011,and REACTION/NCT02580994) and atezolizumab(NCT02748889).The results have not yet been announced,and we are looking forward to their findings.
Checkpoint inhibitor as second-line therapy and beyond for SCLC
According to research data,the ORR of SCLC patients receiving various third-line therapy is 21.3%;the duration of response (DOR) is 2.6 months;the median OS is 4.4 months;and the 1-year survival rate is only 11% (28).For SCLC therapy,it is important to follow up the regimen.The checkpoint inhibitors used as second-line therapy and beyond have achieved a promising result in recurrent SCLC with chemotherapy tolerable.FDA has approved nivolumab in the treatment of recurrent SCLC in 2018,and immunotherapy has become an accessible treatment option for SCLC.
Checkpoint inhibitor as monotherapy
As part of the phase Ia study (NCT01375842),17 patients with ED-SCLC received atezolizumab at 15 mg/kg or 1,200 mg via intravenous infusion every three weeks.The ORR of the two groups is 6% and 24%,respectively;the median PFS and OS of all these patients are 1.5 months and 5.9 months,respectively,suggesting that atezolizumab is safe and effective as a monotherapy for SCLC patients (19).
KEYNOTE-028 is a phase Ib trial,which as a monotherapy evaluated the efficacy of pembrolizumab in 24 patients with PD-L1-positive,platinum-refractory EDSCLC,demonstrated an ORR of 33% (95% CI,16%−55%) and a median PFS of 1.9 months (9).In another trial,KEYNOTE-158,pembrolizumab demonstrated an ORR of 18.7% (95% CI,11.8−27.4),median PFS of 2.0 months and median OS of 8.7 months(20).A checkpoint inhibitor as monotherapy for SCLC can provide long-term clinical benefits and causes less toxicity.
A phase III clinical trial,Checkmate-331,reported that nivolumab was ineffective,and thus the administration of this drug was discontinued prematurely.A series of clinical trials have been conducted to compare the efficacy of pembrolizumab and topotecan in patients with recurrence SCLC (NCT02963090).Further studies have also been performed to examine the effectiveness of durvalumab as a first-line treatment for SCLC (MEDIOLA/NCT 02734004).
Double checkpoint inhibitor combination
CTLA-4 acts in T cell activation at an early stage,whereas PD-1/PD-L1 acts in the later stages of T cell activation in tumor immune responses.The combination of these two inhibitors is more effective than either of the two alone.
In a basket phase I/II study,Checkmate-032,dual blockade of PD-1 and CTLA-4 was used to treat patients with relapsed SCLC:the nivolumab at 1 mg/kg plus ipilimumab 3 mg/kg arm achieved an ORR of 23%;and the nivolumab monotherapy arm achieved 10% (21).The results of the expanded cohort of recurrent SCLC patients showed that ipilimumab (3 mg/kg) combined with nivolumab (1 mg/kg) resulted in higher ORR (21.9%vs.11.6%) and long-term OS (5.7 monthsvs.4.7 months) than nivolumab alone (22).Based on the above results,the National Comprehensive Cancer Network guidelines recommend the combination of nivolumab and ipilimumab as a second-line choice for patients with SCLC,while nivolumab was approved by the FDA as a salvage treatment for SCLC.
In a phase I study in 2017,30 patients with ED-SCLC were enrolled to evaluate the safety and clinical activity of durvalumab in combination with tremelimumab(NCT02261220).The results exhibited an ORR of 13.3%,a median PFS of 1.8 months (95% CI,1.0−1.9),and a median OS of 7.9 months (95% CI,3.2−15.8),indicating that durvalumab combined with tremelimumab had a tolerable safety and activity in pretreated ED-SCLC patients who are both platinum sensitive and platinum resistant (23).
CTLA-4 and PD-1 negatively regulate T-cell activation in different ways;thus,dual blockade of CTLA-4 and PD-1 enhances antitumor activity (21,23).However,the risk of developing serious immune-related cardiotoxicity is also increased greatly (29).Approximately 82% of patients who used more than two kinds of immune checkpoint inhibitors developed treatment-related AEs,while only 60% of patients who used one type of immune checkpoint inhibitor developed treatment-related AEs (21).Other immune checkpoint molecules such as lymphocyte-activation gene 3,T-cell immunoglobulin mucin-3,and V-domain immunoglobulin suppressor of T-cell activation have been explored (30).
Checkpoint inhibitor as switch maintenance treatment in patients with SCLC
Pembrolizumab delays drug resistance and is used as a switch maintenance therapy.A single-arm phase II trial investigated pembrolizumab as the switch maintenance therapy for 12 months in ED-SCLC patients after completion of standard therapy (NCT02359019).Of the 45 patients enrolled in this study,5 achieved an objective response,resulting in an ORR of 11.1%.The median PFS was 1.4 months,while the median OS was 9.6 months.Patients treated with pembrolizumab developed AEs including fatigue,nausea,cough,and dyspnea.One patient developed atrioventricular block,while another patient developed type 1 diabetes (24).
The CheckMate-451 study evaluated the effect of nivolumab as switch maintenance therapy.The study included 834 patients with ED-SCLC who did not progress after four cycles of chemotherapy.Results showed no significant increase in OS (31).
Study on prognostic biomarkers of immune checkpoint inhibitors
PD-L1 expression level has been investigated as a potential biomarker to predict response to anti-PD-1/PD-L1 therapy (32,33);however,its effectiveness in SCLC patients remained controversial due to the differences in the positive cutoff level,diagnostic kits,staining antibodies,difficulty in obtaining specimens,and fixation techniques(13,34).An exploratory analysis of biomarkers was conducted in the KEYNOTE-158 trail;the positive rate of PD-L1 in this study was 39% (42/107),and the PD-L1-positive patients had higher ORR (35.7%vs.6.0%) and longer OS (14.9 monthsvs.5.9 months) than PD-L1-negative patients.In CheckMate-032 study,PD-L1 expression was detected by Dako28-8 mAb assay;results showed that approximately 17% of patients were positive for PD-L1.However,the therapeutic effect of nivolumab with or without ipilimumab was independent of the state of PD-L1 expression.In the CheckMate-032 study,an exploratory analysis of tumor mutation burden (TMB) and nivolumab efficacy was conducted,and the results were published on World Conference on Lung Cancer (WCLC)in 2017.A total of 211 patients were evaluated for TMB;the results showed that patients with high TMB showed higher ORR.Moreover,patients with complete response/partial response had higher TMB than those with stable diseases/progressive diseases.In the nivolumab +ipilimumab treatment group,the PFS and OS of patients with high TMB were 7.8 months and 22.0 months,respectively.The study concluded that immunotherapy and high TMB are associated with better clinical benefit,and TMB is a potentially helpful marker to predict response to immunotherapy (35).Due to the small number of SCLC cases and difficulties in sample collection,exploratory studies primarily focus on investigating the potential predictive biomarkers.However,only a few studies used screening criteria.Hence,further studies determining the prognostic biomarkers of SCLC may be beneficial in future clinical practice.
CIT
Patients with SCLC are found to have functional deficiency in a variety of immunocytes (36),such as NK cells,lymphokine-activated killer cells,tumor-infiltrating lymphocytes (TILs),CTLs,cytosine induced killer (CIK)cells,and gamma delta-positive T lymphocytes (γδT).CIT transforms and amplifies immune cellsin vitrothrough cell engineering.For example,the expression of C-X-C motif chemokine receptor 2 (CXCR2) on the surface of T cells is conducive to the delivery of T cells to tumor,and chimeric antigen receptor-engineered T cells (CART) can target tumor-associated antigens (TAAs) to kill tumor cells without human leukocyte antigen (HLA) presentation.
A prospective cohort study of CIT with autologous NK,γδT,and CIK cells as a maintenance therapy for SCLC patients showed that OS was extended to 8.5 months in the study groupvs.the control group (20 and 11.5 months,P=0.005) (37).Another study indicated that chemotherapy combined with CIK-cell therapy significantly improved the ORR of patients with ED-SCLC (40.9% and 9.1%),and the PFS of the combined treatment group was also longer than that of the control group (8vs.4 months,P=0.005)(38).None of these studies have observed severe side effects,indicating that CIT might provide a safe and effective treatment for patients with SCLC.
By specifically identifying the tumor cell surface proteins with major histocompatibility complex,CAR-T cell immunotherapy has shown long-lasting and potential therapeutic effects on patients with malignant hematopathy and has been approved in the treatment of B-cell acute lymphoblastic leukemia (39).Some cell surface molecules are highly expressed in SCLC and are potential targets of CART therapy,such as delta-like protein 3 (DLL3),CD56,and CD47.DLL3 is expressed in about 80% of SCLC patients according to previous studies,while almost nonexistent in normal people (40).A phase I,first-inhuman study was conducted to evaluate the safety and tolerability of AMG 119,a CAR-T cell therapy targeting DLL3 in patients with relapsed/refractory SCLC(NCT03392064).CD56R-CAR-T cells were able to inhibit SCLC tumor cells growthin vivo(41).CD47 is overexpressed in SCLC and plays an important role in blocking phagocytosis,improving tumor survival,metastasis,and angiogenesis (42).CD47-CAR-T cells can effectively kill a variety of cells with high expression of CD47.Therefore,CD47-CAR-T cells are expected to be a potential treatment for SCLC (43).
CIT is an effective anti-tumor immune method,but its efficiency against SCLC is still under investigation due to the difficulty in achieving the efficiency and standardization of immune cell amplification and preparationin vitro(44).Immunosuppressive factors in the tumor microenvironment can also limit its clinical application:impenetrable of T cells due to tumor capsule,outer fibrosis (45) and activation of immune checkpoint pathway (46).Combination of radiofrequency or chemotherapy and CIT was also associated with improvements in clinical outcomes of patients with solid tumors (47,48).This finding has demonstrated that the combination of CIT with other therapies may have a promising effect.Moreover,the results of multi-center,large-sample clinical studies will be used as reference in the future research.
Tumor vaccines
Tumor vaccines can bind to tumor antigen to stimulate dendritic cells (DC) and activate CD8 T cells,induce cellular and humoral immune responses (49,50),and enhance the effect of antibody-dependent cell-mediated cytotoxicity (ADCC).TAA is a protein expressed by unmutated genes,which is significantly overexpressed in tumor cells but rarely expressed in normal cells.Several TAAs have been found in SCLC cells,such as the fucosyl-GM1 (51),ganglioside GD3,polysialic-acid (52),and P53 protein (53).
As an anti-fucosyl-GM1 antibody,BMS-986012 inhibits SCLC growthin vitrowhen used alone or in combination with chemotherapeutic or immunomodulatory agents (51).A phase I/II trial is ongoing to evaluate the safety and efficiency of BMS-986012 in combination with platinum and etoposide as first-line therapy for ED-SCLC(NCT02815592).
INGN-225 is a p53 vaccine based on adenovirustranduced DC (DC-Ad-p53 vaccine),which can yield a substantial T-cell response and enhance the chemotherapeutic effect in 40%−57% of patients with ED-SCLC(53).However,a phase II clinical trial showed that DC-Adp53 vaccine failed to improve ORRs to the second-line chemotherapy (54).As its safety profile and therapeutic immune potential remain,combination with the other immunotherapeutic agents are reasonable options,and another phase II clinical study examined the efficiency of INGN-225 combined with chemotherapy in patients with SCLC (NCT00617409).
However,most clinical trials on tumor vaccines based on TAAs have failed to improve the OS of patients (55-58).TAA may be not an ideal therapeutic antigen as these antigens are expressed in normal cells and are likely to lead to autoimmune phenomena and serious side effects,and the immune system is usually highly tolerant to an antigen of its own origin.Therefore,it is difficult to stimulate the response of the patients’ immune system (59).The use of a combination of therapies may enhance the effect of tumor vaccines.
Antibody-drug conjugates (ADC)
A monoclonal antibody has high specificity of binding to antigen and displays good molecular targeting function.ADCs can kill tumor cells by specifically identifying TAAs in tumor cells (60).
By conjugating toxin tesirine to DLL3 monoclonal antibody,rovalpituzumab tesirine (Rova-T) can specifically identify and target SCLC cells.In a phase I study,disease control rate (DCR) of 68% was detected in recurrent or refractory SCLC patients treated with Rova-T monotherapy,and it was higher (88%) in the high DLL3 subgroup(DLL3 expression >50%) (61).In a phase II study(TRINITY),the effects of Rova-T as first-line or secondline treatment in DLL3 positive (≥25% tumor cells expressing DLL3 by immunohistochemistry) SCLC patients were detected,the results showed that Rova-T was more effective in third-line treatment in patients with high expression of DLL3 (≥75%),but the ORR is only 18% in the overall population (62).
A phase III study MERU (NCT03033511) is ongoing to evaluate the efficacy of Rova-T as maintenance therapy for patients with SCLC following first-line chemotherapy.Another phase III study TAHOE (NCT03061812) in ongoing to compare Rova-Tvs.topotecan in subjects with advanced or metastatic SCLC.
Sacituzumab govitecan (IMMU-132) is another ADC that conjugates the active metabolite of the topoisomerase-1 inhibitor camptothecin (irinotecan) into an antibody that binds to Trop-2,a calcium-transducing transmembrane glycoprotein widely expressed in SCLC (63).In a phase II trial,IMMU-132 for the treatment of patients with recurrent metastatic SCLC,reported an ORR of 14% and a DCR of 35%,respectively,and a median OS of 7.5 months (64).Based on this study,IMMU-132 has received FDA Fast Track Designation in SCLC.ADC treatment has brought hope to the SCLC,which would also be a pioneer in the individualized treatment of SCLC.
Immunotherapy with immunomodulators
Immunomodulator regulation consists of positive immune regulation,including some cytokines,and negative immune regulation,such as immune checkpoints,which have been described in the previous paragraphs and will not be repeated here.In recent years,some monoclonal antibodies attached to a chemotherapeutic drug targeting signaling pathways or gene replication have been found to have immunomodulatory effects,which may provide new strategies for immunotherapy.
Cytokines
Widely used in CIT to induce and amplify lymphocytes,cytokines can directly stimulate immune cells and enhance their cytotoxicity.Several cytokines have been approved by FDA for cancer treatment,such as high-dose IL-2 for melanoma and renal cell carcinoma,and interferon-α (IFNα) for adjuvant therapy for stage III melanoma (65).
IFN-α can enhance ADCC and antigen presentation,inhibit angiogenesis and induce tumor apoptosis (66).In two phase II trials conducted on patients with LD-SCLC or ED-SCLC,both studies showed statistically significant survival benefit (P<0.05) in patients treated with IFN-α plus chemotherapyvs.chemotherapy alone (67,68).By contrast,a phase II study showed the addition of IFN-α and 13-cis-retinoic to paclitaxel did not improve the outcomes of patients with recurrent SCLC (69).
IFN-γ is mainly produced by NK and NKT cells,which has several anti-tumor and immunomodulatory effects (70).However,the anti-tumor role of IFN is complex and controversial.IFN-γ can activate the Janus kinase-signal transducer and activator of transcription (JAK-STAT)pathway by phosphorylating JAK1 and JAK2 proteins,and the sustained type II interferon signaling promotes epigenomic changes associated with STAT1 in tumors (71).In vivostudies,IFN-γ increased the expression of HLA and reduced the expression of gBK protein;cells treated with IFN-γ then were killed by the CTL more effectively (67).However,earlier trials of IFN-γ were discontinued due to lack of statistically significant results or dose-dependent toxicity.However,IFN remains a potential auxiliary therapy in patients with SCLC,and further trials are needed to identify its effect.
Immunotherapy targeting macrophage-stimulating agent
RRx-001 is a macrophage-stimulating agent with the ability to partially reverse resistance to chemotherapy in SCLC patients by epigenetic effects.RRx-001 can synergize with chemotherapy,radiotherapy and immunotherapy (72),as well as protect normal tissues against cisplatin-induced toxicities (73).
A phase II clinical study,QUADRUPLE THREAT(NCT02489903),showed that the SCLC patients who had undergone RRx-001 treatment and restarted etoposideplatinum (EP) treatment showed an ORR of 26.9% in the intention-to-treat population,median OS were 8.6 months.RRx-001 followed by re-challenge with platinum plus etoposide chemotherapy is effective and tolerable,the most common treatment-emergent adverse event from RRx-001 was mild discomfort at the infusion site (23%) (74).
Immunotherapy targeting myeloid-derived suppressor cells(MDSCs)
MDSCs can inhibit the functions of T cells and other immune cells.Pre-clinical studies have found that the coculture of T cells and MDSC from patients with SCLC can induce the apoptosis of T cells (75),and the content of MDSC in peripheral blood is related to the prognosis of SCLC patients (76).Apolipoprotein E (ApoE) binds to MDSC cell surface receptor LRP8 and induces apoptosis of MDSC (77).RGX-104 (GW3965) is an agonist of nuclear hormone receptor (LXR),which can induce the transcription and expression of ApoE.RGX-104 combined with PD-1 inhibitor showed a synergistic effect on activating anti-tumor immunity in animal models (78).Research on the treatment of recurrent solid tumors(including SCLC) by RGX-104+/− Nivo is also under way(NCT02922764).
Toll-like receptor 9 (TLR9) agonist
TLRs are mainly expressed in B cells and DC;activation of TLR9 can activate the innate and acquired immunity.Lefitolimod (MGN1703) is a TLR9 agonist,which can connect to DCs,then release IFN-α,and activate mononuclear cells,NK cells,T cells and NKT cells,thereby producing chemokines IP-10.Lefitolimod can also promote the secretion of various inflammatory factors by binding to TLR9 expressing B cells,and promote the differentiation of B cells into plasma cells to produce antibodies (79).In the previous phase I and II studies,lefitolimod was found to activate anti-tumor immune response and demonstrated early signs of immunotherapy efficacy,as well as tolerability (80,81).
In a phase II IMPULSE study on patients with EDSCLC,subgroup analysis indicated that immunotherapeutic maintenance treatment combined with lefitolimod reduced the risk of death in patients with low frequency of activated CD86+B cells (HR,0.53;95% CI,0.26−1.08) and in patients with chronic obstructive pulmonary disease (HR,0.48;95% CI,0.20−1.17) (82).
New role of traditional drugs in immune moderation
An increase in genomic aberrations and rapid cell proliferation in SCLC resulted in DNA damage and genomic instability.Poly (ADP-ribose) polymerase (PARP)is a family of enzymes involved in DNA repair.The expression of PARP enzyme in SCLC cells was significantly higher than that of normal lung epithelial cells and other lung cancer tissue subtypes (83).By inhibiting DNA repair and promoting apoptosis of tumor cells,PARP inhibitors can enhance the efficacy of radiotherapy,alkalinizing agents and platinum drug chemotherapy (84).They are able to promote CCL5 secretion,activate type I IFN,and induce PD-L1 expression;DNA damage also triggers the release of various molecular signals,which can enhance the anti-tumor immune response (85).
Temozolomide (TMZ) is an oral alkylating agent that causes apoptosis as its cytotoxic effect.A phase II study in patients with recurrent SCLC showed a significantly higher ORR in the TMZ+veliparib group compared with the TMZ group (39%vs.14%;P=0.016).However,there was no significant difference in the median PFS and OS between the two groups (86).Another phase II study evaluating the combination of cisplatin and etoposide with or without veliparib in ED-SCLC patients also demonstrated modest improved efficacy;the ORR of veliparib and placebo groups was 71.9%vs.65.6%,respectively.Median PFS was 6.1 and 5.5 months,while the median OS was 10.3 and 8.9 months,respectively (87).
Lurbinectedin (PM1183),a transcription inhibitor,blocks transcription and induces DNA double-strand breakage,leading to aberration and apoptosis of tumor cells during mitosis (88).In the preclinical model,lurbinectedin can reduce tumor-related macrophages and inflammatory tumor microenvironment (89).In a phase I study,results from lurbinectedin and doxorubicin in relapsed SCLC have shown remarkable activities with manageable tolerance,with an ORR of 57.7% and a DCR of 69.2%.As a secondline treatment,it showed durable response rates of 91.7%and 33.3% in patients with sensitive diseases and resistant diseases,respectively (90).
Conclusions and expectation
Immunotherapy is the most promising treatment for SCLC in recent years.Nivolumab is the first FDA-approved third-line immunotherapy for SCLC (35).In the IMpower133 study,atzolizumab combined with chemotherapy as first-line therapy also showed improvement in OS (15).Tumor vaccines,immunomodulators,cellular immunity and other immunotherapy methods play an increasingly important role in comprehensive tumor therapy.Reasonable treatment timing and optimal combined strategy are the hotspots of SCLC immunotherapy (Table 2).
Immune checkpoint inhibitors have brought changes in the treatment mode of SCLC,but they are only limited to a small number of patients with limited efficacy (20).Their development also strongly promotes the development of biomarkers.Several immune-based biomarkers have been evaluated,including TILs in tumor cells (44),secretion of immune factors (e.g.,cytokines),expression of cell surface molecules (e.g.,PD-L1),and gene signatures/patterns(dMMR,MSI-H) (35).Efforts are underway to identify predictive immune-based biomarkers that may help select patients who may benefit from immunotherapy (91).Personalized medicine will be used in the therapeutic management of SCLC patients in the near future.
Immunotherapy,targeted therapy and chemotherapy act on different targets and cells,and the combination of these drugs is expected to achieve greater therapeutic effects.The PACIFIC trial of NSCLC showed that PFS and OS were significantly longer in the radiotherapy+durvalumab group,especially in PD-L1 positive patients (92).SCLC is sensitive to radiotherapy (2);immunotherapy combined with radiotherapy is expected to further improve the survival benefit of SCLC patients (26,27).In addition,various therapeutic combinations of novel drugs are being explored,some of which have provided a strong theoretical basis for further clinical trials of SCLC.
In addition,more traditional targeted therapies have been found to have immunomodulatory effects.For example,DNA repair inhibitors (such as PARP inhibitors)have been found to have immunomodulatory effects while improving the efficacy of chemotherapy (85),which can open up new strategies for combined therapy.In addition to these emerging drugs and clinical studies,several new drugs and therapeutic combinations have been evaluated in preclinical studies or are at the early stage of clinical development.
Overall,therapeutic strategies for SCLC have made breakthroughs in recent years.However,the tumor immune microenvironment is dynamic and complex,and the tumor cells can escape immune surveillance in various ways,leading to the immune tolerance and poor efficacy of the immunotherapy (93).Research on biomarkers to screen effective population,improve treatment response rate,and combine with other therapies needs to be further explored(94).Large randomized phase III trials are still needed todetermine the effectiveness and optimal combination strategy of those therapies (95).
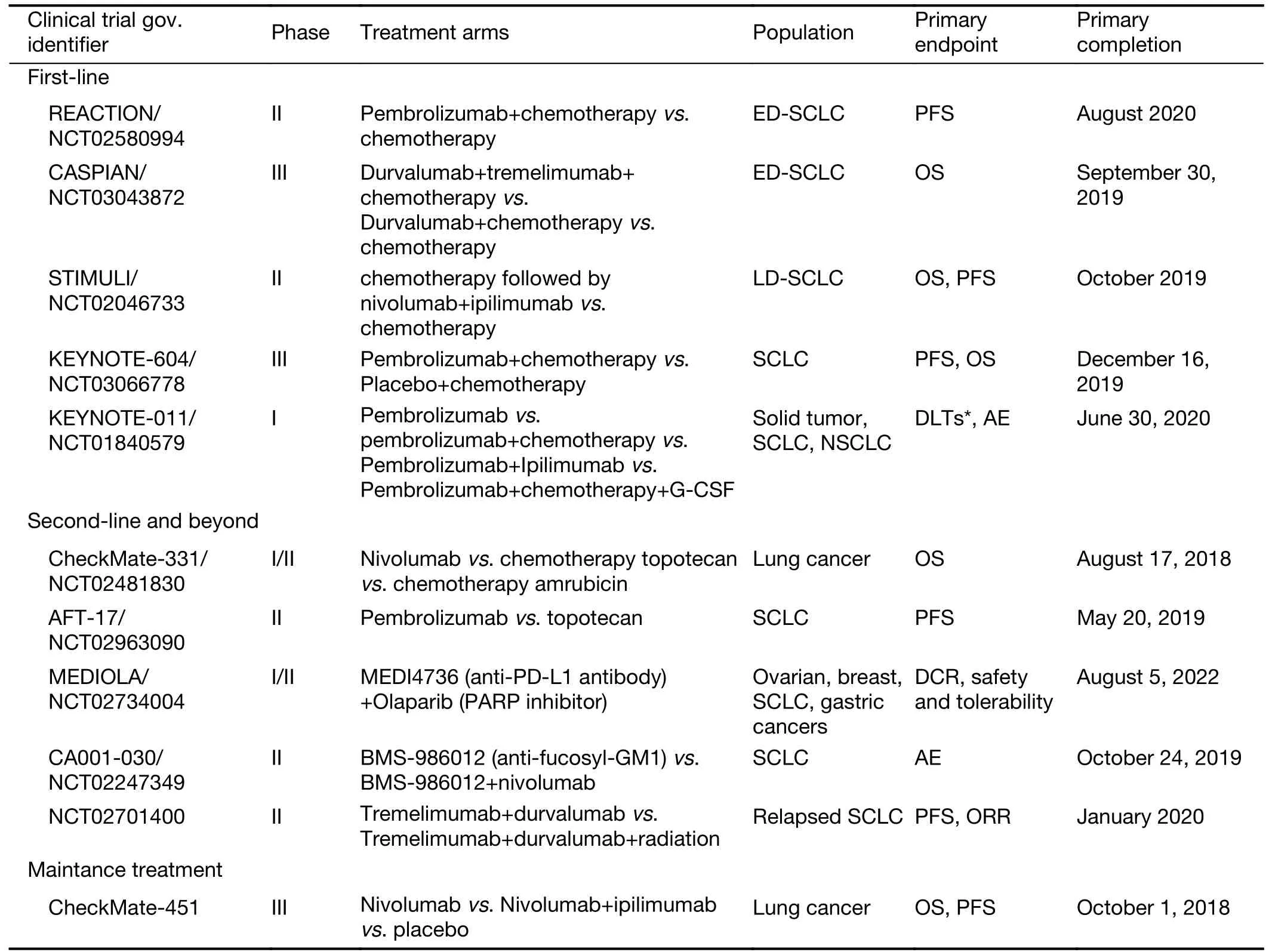
Table 2 Ongoing clinical trials of immune checkpoint inhibitors in SCLC
Acknowledgements
This study was supported by the Ministry of Science and Technology Foundation (No.2016YFC1303804) and the National Natural Science Foundation of China (No.81672275).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2020年1期
Chinese Journal of Cancer Research2020年1期
- Chinese Journal of Cancer Research的其它文章
- A nomogram to preoperatively predict 1-year disease-specific survival in resected pancreatic cancer following neoadjuvant chemoradiation therapy
- Spectral CT imaging parameters and Ki-67 labeling index in lung adenocarcinoma
- PGC-MG7 combination could be used as a follow-up panel for monitoring dynamical progression of gastric precancerous diseases
- Tumor-associated macrophages regulate gastric cancer cell invasion and metastasis through TGFβ2/NF-κB/Kindlin-2 axis
- A CT-based radiomics nomogram for prediction of human epidermal growth factor receptor 2 status in patients with gastric cancer
- Prognostic impact of D2-plus lymphadenectomy and optimal extent of lymphadenectomy in advanced gastric antral carcinoma:Propensity score matching analysis