
lmpact of training specificity on exercise-induced cardiac troponin elevation in professional athletes:A pilot study
2020-02-24 06:38
World Journal of Cardiology 2020年1期
Johan O Wedin,Department of Clinical Physiology,Sundsvall County Hospital,Sundsvall 851 86,Sweden
Johan O Wedin,Nicolena S Nyberg,Anders E Henriksson,Department of Clinical Chemistry,Sundsvall County Hospital,Sundsvall 851 86,Sweden
Anders E Henriksson,Department of Natural Sciences,Mid Sweden University,Sundsvall 851 70,Sweden
Abstract
Key words:Athlete;Exercise;Floorball;Sports medicine;Yo-Yo IR2 test;Myocardial injury;Cardiac troponin
INTRODUCTION
Cardiac troponin (cTn) is a highly specific biomarker of cardiac myocyte injury and necrosis[1,2].Asymptomatic elevation of cTn in athletes following strenuous and continuous-type endurance events is common[3,4],but the mechanisms and clinical relevance are unknown[5].We previously reported that high-sensitivity cardiac troponin T (hs-cTnT) elevation occurs after floorball games with intra-individual reproducibility[6].cTn response to high-intensity intermittent exercise remains poorly examined and inconsistent due to assay differences and variability in sampling frequency and exercise mode[7].
According to the training specificity principle,physical adaptations are related to exercise mode,duration,and frequency[8].Thus,an exercise routine similar to the competitive element is desirable.Continuous exercise tests are inadequate in intermittent team sports such as football[9],whereas intermittent tests such as the Yo-Yo Intermittent Recovery (IR) test correlate with match performance[10].Despite this,little is known about the impact of the training specificity principle on cTn release.Looking at endurance athletes in a meta-analysis,Shaveet al[11]found a greater magnitude of cTn elevation after running than cycling.However,these results were based on earlier generation assays as well as single blood draws post-exercise that failed to detect late cTn peaks[12].
Floorball is a popular Scandinavian intermittent team sport and among the fastest growing sports in Sweden[13].Depending on player position and time played,there are individual differences in physical effort and cardiac load during a game.Laboratorybased studies with exercise manipulations give a better understanding of how cardiac work influences the release of cTn[14].The use of standardized physical tests correlates with a defined physical effort and levels of cardiac biomarkers.
The aims of this study were to investigate the response of hs-cTnT to high-intensity intermittent exercise compared to continuous exercise in standardized settings,and to examine hs-cTnT release kinetics up to 24 h post-exercise.
MATERIAL AND METHODS
Participants and experimental design
Nine male elite floorball players were invited to participate in the study.The participants were screened for cardiovascular disease using the Lausanne Recommendations questionnaire,physical examination,two-dimensional echocardiography,and resting 12-lead ECG interpreted according to recommendations in athletes[15].All participants were informed in detail of the experimental procedures and gave their written consent for participation.The study was approved by the regional ethics committee,and all procedures adhered to the Declaration of Helsinki.
Two different types of standardized exercise tests,a cycle ergometer test and a Yo-Yo IR2 test,were carried out on different occasions with a 6-mo interval.All testing sessions were performed indoors in air-conditioned facilities with a set temperature of 20°C and a humidity of approximately 50%.The participants were instructed to avoid all physical activity 48 h prior to the tests.Venous blood samples were collected before the tests and 0,2,6,and 24 h after the tests to measure levels of hs-cTnT.Blood lactate levels were measured before and at different timepoints after the cycle ergometer test.
Cycle ergometer test
A cycle ergometer test was performed on a computer-controlled,mechanically braked cycle ergometer (Ergomedic 839;Monark,Vansbro,Sweden).The initial workload was set to 120 W and the resistance was increased 20 W every minute up to 300 W where,if reached,the participants pedaled until exhaustion.Pedal rate was kept constant at 60-65 revolutions per min.A 12-lead electrocardiogram (ECG),including heart rate (HR),was monitored throughout the test (Cardiolex EC Sense Software,Cardiolex,Solna,Sweden).No participant was asked to terminate prematurely due to adverse cardiovascular events,and the ECG gave no indication of ischemia or arrhythmias.All participants (n= 9) reported leg fatigue as the cause of termination.
Yo-Yo IR2 test
The participants completed a Yo-Yo IR2 test that consisted of repeated shuttle runs between a starting line and finishing line marked by cones 20 m apart.A third cone was placed 5 m behind the starting line.The running speed was dictated by beeps from a CD player,using the Team Beep Test Software 4.1 for PC (Bitworks Design,Cheltenham,United Kingdom).The initial speed was 13 km/h and increased progressively for each covered level;2 km/h after the first level,1 km/h after the second level,and then 0.5 km/h for the following levels.Between each running bout of 2 x 20 m,the participants had a 10 s period of active recovery jogging around the cone behind the starting line[16].A test supervisor was placed at each end line to ensure that the participants completed the full distance.When a participant first failed to complete a shuttle run in the designated time (i.e.,before the beep),a warning was given by the supervisor at the end line.When a participant failed to complete a shuttle run a second time or felt unable to complete another shuttle due to exhaustion,the test was terminated.The performance time was registered.HR was measured throughout the test using a Polar S810 HR monitor (Polar Electro Oy,Kempele,Finland).
Laboratory assays
Blood samples for plasma analysis were collected into 3.5 mL lithium heparin vacutainer gel tubes,and blood for analysis of blood lactate concentration was collected into 3 mL sodium heparin vacutainer tubes.The same experienced phlebotomist collected all blood samples,which were immediately transported to the laboratory for analysis.For quantitative measurement of plasma hs-cTnT,the Elecsys 2010 system (Roche Diagnostics GmbH,Mannheim,Germany) was used according to the manufacturer’s instructions.The hs-cTnT assay had a limit of blank of 3 ng/L,a 5 ng/L limit of detection,and a 99th percentile myocardial damage cutoff point of 14 ng/L.The coefficient of variation (CV) was 7% at the cutoff level.Venous blood lactate levels were measured using an amperometric method on a Radiometer ABL825 Flex (Radiometer,Copenhagen,Denmark) according to instructions,with a total CV < 4% across the analytical range (0-30 mmol/L).
Statistical analysis
Continuous variables were calculated as median (interquartile range),and categorical data were expressed as absolute numbers with percentages.The highest achieved heart rate in the tests is referred to as peak HR.Differences between pre-exercise and post-exercise plasma hs-cTnT concentrations and differences in hs-cTnT concentration between exercise modes were assessed using paired Wilcoxon rank-sum test.Results were considered statistically significant whenPvalues were < 0.05.All calculations were performed with IBM SPSS 23.0 (IBM,Armonk,NY,United States).
RESULTS
Cardiovascular screening showed no signs of cardiovascular abnormalities in the nine participants included in the study.Baseline characteristics of the participants are presented in Table1.There was no difference in training volume since all participants played for the same floorball team.The performance time was significantly longer in the cycle ergometer test than in the Yo-Yo IR2 test (10.1 minvs7.4 min,P= 0.018).Median peak HR achieved in the Yo-Yo IR2 test (196 bpm) were significantly (P=0.021) higher than that in the cycle ergometer test (190 bpm).The average HR was higher in the Yo-Yo IR2 test (171 bpmvs159 bpm,P= 0.008).Baseline hs-cTnT concentrations and changes 0,2,6,and 24 h after completion of each exercise mode are shown in Figure1,Table2,and Table3.Median hs-cTnT concentration was significantly higher at 2 and 6 h post-exercise (P= 0.028 andP= 0.038,respectively) in the Yo-Yo IR2 test compared to the cycle ergometer test (Table2).
Cycle ergometer test
All participants had normal baseline levels of hs-cTnT (< 14 ng/L) prior to the cycle ergometer test.Median values of hs-cTnT increased post-exercise but were below cutoff at all timepoints post-exercise (Table3).The peak median hs-cTnT concentration of 7.8 ng/L was observed 6 h post-exercise,a significant (P= 0.021)increase from baseline.All concentrations normalized within 24 h post-exercise.The maximal individual value observed was 12.6 ng/L (6 h post-exercise),having increased 133% from baseline.The median percentage change in hs-cTnT compared to baseline peaked 2 h post-exercise (28% increase in hs-cTnT concentration).
Median concentration of lactate was within the reference interval (0.5-2.2 mmol/L)before the cycle ergometer test,increased significantly (P< 0.001) to 14.7 mmol/L immediately after the test,and returned within reference in all participants within 2 h post-exercise.A lactate concentration > 4.0 mmol/L indicated that the cycle ergometer test had an anaerobic character.
Yo-Yo IR2 test
All participants had normal hs-cTnT baseline levels (< 14 ng/L) prior to the Yo-Yo IR2 test.Increased median hs-cTnT levels was observed at all timepoints post-exercise,with the peak median concentration at 6 h post-exercise of 10.6 ng/L,a statistically significant increase from baseline (P= 0.008).Median values of hs-cTnT post-exercise were below cutoff at all timepoints post-exercise,but the 75th percentile value rose above the cutoff at 2 and 6 h post-exercise.All concentrations normalized within 24 h post-exercise,and the median value 24 h post-exercise (5.7 ng/L) was nonsignificant when compared to baseline (P= 0.260).Individually (Figure1),a total of three of nine participants had hs-cTnT levels above cutoff at 6 h post-exercise.The highest individual value was observed 6 h post-exercise (22.6 ng/L) and corresponded to a 178% increase from baseline.The hs-cTnT median percentage change in hs-cTnT concentration was higher after the Yo-Yo IR2 test compared to the cycle ergometer test,98%vs28% at 2 h post-exercise and 107%vs27% at 6 h post-exercise.
DISCUSSION
This is the first study to compare serial hs-cTnT release after two different standardized exercise modes in professional athletes adapted to high-intensity intermittent exercise.The primary finding was that hs-cTnT release among floorball players was significantly higher after completion of an intermittent test (Yo-Yo IR2 test) than after a continuous cycle ergometer test.Concentrations of hs-cTnT exceeded the 99th percentile cutoff in one-third (3 out of 9) of the participants after the intermittent test,but in none (0 of 9) after the continuous cycle ergometer test.Our findings support the theory that the training specificity principle impacts the release of cTns.These findings were observed in standardized settings and expand previous work from field-based studies.The results suggest that physicians must be aware that release of cTn commonly occurs following short high-intensity intermittent exercise,and not exclusively after long-term strenuous efforts.
In daily clinical practice,the results of laboratory tests assist in decision making.cTns are a cornerstone in the diagnosis of myocardial infarction (MI).In patients with signs of myocardial ischemia,acute MI is defined by one troponin concentration >99th percentile together with a rising or falling pattern[2].With increasing sensitivity of cTn assays,the rise or fall of cTn concentration in serial blood samples is important to differentiate acute from chronic myocardial injury[17],but the magnitude of increase or decrease has not been determined.With high-sensitivity assays,even minor numerical changes above the 99th percentile cutoff arising from biological and/oranalytical variations could prompt important clinical decisions.The reference change value (RCV) might aid the interpretation in such small cTn elevations,as it takes both analytical and biological variation into account.The RCV describes the maximum size of a difference that can occur by chance[18].Thus,a relative change in cTn that exceeds the RCV is considered clinically significant and may indicate acute myocardial necrosis.Vasileet al[19]found that,for the Roche hs-cTnT assay,short-term RCV over a 6 h period was 84%.Two other groups also evaluated the Roche hs-cTnT assay in healthy individuals and found lower RCV,62% and 40% respectively[20,21].We found that the percentage change was significantly higher after the Yo-Yo IR2 test.The median percentage change 6 h post-exercise exceeded the upper RCV suggested in the studies mentioned above.This indicates that the change could be considered clinically significant.By the same reasoning,the percentage change in the cycle ergometer test could be explained by biological and/or analytical variation.

Table1 Baseline characteristics of the 9 participants included in the study
In the present study,the performance time was significantly longer in the cycle ergometer test.Therefore,it seems that differences in exercise times had no impact on hs-cTnT concentration.Also,peak lactate concentration in the cycle ergometer test was not different from the previously observed values in the Yo-Yo IR2 test[10],indicating performance of similar high-intensity exercise in both tests.All participants reported leg fatigue as cause of termination in the cycle ergometer test,which might have restricted them from reaching higher HR[22].The results showed significantly higher average and peak HR in the Yo-Yo IR2 test,which indicates that a Yo-Yo IR2 test is more appropriate than a cycle ergometer test for assessment of cardiovascular demands among floorball players whereas cycle ergometer demands leg muscle strength.
cTn assays detect myocardial cell damage and necrosis[1,2],but it is still debated to what extent exercise-induced cTn elevation is a physiological or pathological finding.As exercise-induced cardiac biomarker elevations mainly lack correlation to impaired left ventricular function,elevations have been interpreted as physiological[5,23].A prolonged and biphasic cTn release is indicative of release of structurally bound troponin from necrotic cardiomyocytes[24].Most studies report a small,transient leakage of cTn from the cytosolic pool,possibly because of affected sarcolemmal integrity caused by reversible ischemia[25,26]or increased reactive oxygen species production[27].Mechanical stretch of cardiomyocyte integrins,a consequence of increased preload and afterload during exercise,has also been suggested as a cause of troponin release from living cardiomyocytes[28].Higher peak HR in the Yo-Yo IR2 test results in a greater cardiac output and thus ventricular strain could explain why we observed higher hs-cTnT levels.It has also been shown that skeletal muscle damage can cause increases in circulating levels of cTn.In patients with chronic skeletal muscle damage,elevation of noncardiac cTn can mimic an acute myocardial injury[29,30].It is therefore possible that skeletal rather than cardiac muscle is the source of circulating cTn found in the athletes participating in this study.
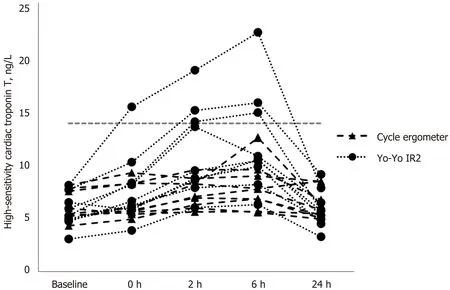
Figure1 lndividual baseline high-sensitivity cTn concentration and changes 0,2,6 and 24 h after completion of the cycle ergometer test and the Yo-Yo lR2 test.
Serial blood specimen collection during the recovery period enables examination of post-exercise cardiac biomarker kinetics and is important to obtain a maximal concentration.In line with other studies recently reviewed by Bakeret al[31],we observed an early peak of cTn elevation (6 h post-exercise),but it is possible that the true hs-cTnT peak was missed in our study.Therefore,a higher sample frequency during the first 6 h post-exercise could be considered in future studies.The small degree and rapid clearance of cTn elevation in the present study argue against myocardial injury and cardiomyocyte necrosis.Accordingly,it seems to reflect a physiological response to exercise.However,the intra-individual reproducibility first observed by Sahlénet al[32],and recently supported in our previous study[6],suggest that some individuals might be susceptible to exercise-induced cTn elevation.This phenomenon should be examined in future studies as it raises the question whether some individuals are susceptible to exercise-induced myocardial damage.This might be an important aspect to consider in the clinical significance of exercise-induced cTn release.
There are some limitations to consider when analyzing the results of this study.First,the sample size was small,and the results may not be applicable in a larger population.This study should therefore primarily be hypothesis-generating for future work.Nonetheless,we detected differences between exercise modes that could be interpreted as clinically relevant and beyond both biological and analytical variation.Second,pulse watches can overestimate HR[33]but the pulse watch used in this study has been validated to ECG[34].However,future studies of similar rationale should aim to use ECG for a reliable comparison of HR.Third,we did not perform post-exercise assessment of cardiac structure and function with echocardiography,making the significance of post-exercise hs-cTnT elevation uncertain in this study group.Fourth,including a group of professional endurance athletes for comparison would add strength to the conclusion that troponin release is dependent on the training specificity principle.
In professional athletes adapted to high-intensity intermittent exercise,we found that hs-cTnT was significantly elevated after high-intensity intermittent but not after continuous exercise.The principle of specificity should be considered when designing future studies to avoid underestimating exercise-induced cTn elevation in athletes.Peak hs-cTnT concentration was observed after 6 h indicating that serial assessment post-exercise is important to observe maximum values.As the relevance of exerciseinduced cTn elevation remains unclear,it should be cautiously interpreted in the clinical setting.

Table2 Exercise test variables in the cycle ergometer test compared to the Yo-Yo lR2 test

Table3 Comparison of plasma levels of high-sensitivity cTn after the cycle ergometer test and Yo-Yo lR2 test
ARTICLE HIGHLIGHTS
Research background
Release of biomarkers of myocardial damage such as cardiac troponins (cTns) is common after strenuous endurance exercise.
Research motivation
Although it is widely recognized that continuous exercise can induce release of cTns into the bloodstream,data on intermittent exercise are scarce.Furthermore,the principle of training specificity has never been investigated.
Research objectives
This study examined how training specificity impacts high-sensitivity cardiac troponin T (hscTnT) release.
Research methods
In this observational study,nine professional floorball players performed two different exercise tests:A continuous incremental cycle ergometer test and a Yo-Yo Intermittent Recovery 2 (Yo-Yo IR2) test.Serial assessment of hs-cTnT was performed after the cycle ergometer test and the Yo-Yo IR2 test (baseline,0,2,6,and 24 h).
Research results
No hs-cTnT elevation above the myocardial damage cutoff (≥ 14 ng/L) was shown after the cycle ergometer test,whereas hs-cTnT levels rose over the cutoff in three of nine participants after the Yo-Yo IR2 test.The hs-cTnT levels peaked at 6 h after both tests,but were significantly higher after the Yo-Yo IR2 test compared to the cycle ergometer test (median hs-cTnT concentration 10.6 ng/Lvs7.8 ng/L,P= 0.038).All levels returned to baseline within 24 h.
Research conclusions
High-sensitivity cardiac troponin T was significantly elevated after intermittent but not continuous exercise.
Research perspectives
The principle of training specificity should be considered when designing future studies and sampling should continue at least 24 h post-exercise to avoid misinterpretation of hs-cTnT elevation.
ACKNOWLEDGEMENTS
We gratefully acknowledge the floorball players for their participation in this study.The technical assistance from D.Hecht von Saldern,P.Rehnstrand,S Svensk,J.Smedberg,and T.Medin is appreciated.Finally,we thank N.Olofsson for his valuable statistical advice.
 World Journal of Cardiology2020年1期
World Journal of Cardiology2020年1期
- World Journal of Cardiology的其它文章
- ls there a role for ischemia detection after an acute myocardial infarction?
- Diagnosis and treatment of heart failure with preserved left ventricular ejection fraction
- Radial artery access site complications during cardiac procedures,clinical implications and potential solutions:The role of nitric oxide
- Prognostic impact of body mass index on in-hospital bleeding complications after ST-segment elevation myocardial infarction
- Phrenic nerve displacement by intrapericardial balloon inflation during epicardial ablation of ventricular tachycardia:Four case reports
- Salmonella typhimurium myopericarditis:A case report and review of literature