
Comparison of general practice residents’ attitudes and perceptions about training in two programmes in China: a mixed methods survey
2020-01-09 02:26SiqingLianYuXiaJinzhiZhangXiaoningHanChunhuaChiMichaelFetters
Siqing Lian, Yu Xia, Jinzhi Zhang, Xiaoning Han, Chunhua Chi, Michael D Fetters
ABSTRACT Objective To understand general practice (GP) residents'attitudes about their residency training in China.Design Mixed methods survey administered crosssectionally.Setting Two GP training programmes similar in most regards according to current GP training policy of 5 years'undergraduate degree in medicine and 3 years of postgraduate GP residency training-but differing as the Beijing programme has adopted educational innovations beyond the nationally prescribed standard curriculum used by the second Shenzhen programme.Participants 105 (85%) of eligible GP trainees, 35 (90%)in the innovative Beijing programme and 70 (83%) in the standard training Shenzhen programme.Results Overall, residents felt discrimination because of specialty choice, and that they lacked competency as a general practitioner. Many residents commented faculty had negative teaching attitudes. Beijing residents were more satisfied than Shenzhen residents with their training (p=0.001), and felt teaching faculty had sufficient knowledge (p<0.001), and appropriate attitudes towards teaching (p=0.004). Beijing residents more strongly agreed on five items about good future job prospects (all p<0.05).Conclusion These Chinese GP residents identify areas for improvement in their training as well as strengths.Higher satisfaction with faculty teaching and job optimism in Beijing where GP residents receive training from specifically qualified faculty, and can earn special certification, suggest that the educational innovations enhance training and promote positivity about job prospects. These findings imply that GP residents in China face many training challenges that are similar to other international reports, while also implicating benefits of using an innovative curricular approach.
Key points
INTRODUCTION
Since 2010, increasingly the Chinese govern—ment has made training of general practi—tioners a priority to help resolve the nation's healthcare provider shortage. The aim of general practice (GP) residency training is to provide trainees with the skills necessary to practise fully as general practitioners.In 2011, the State Council of the People's Republic of China strengthened the training requirements of general practitioners by implementing standardised training.1Since December 2013, every medical student needs to complete residency training to become an independent physician.2As an illustra—tion of the commitment by the government,in September 2018, the National Health Commission of the People's Republic of China mandated that all general hospitals that were already qualified to provide stan—dardised residency training needed to estab—lish a GP department by the end of December 2019 or face cancellation of the hospital's training certification.3
The Chinese Medical Doctor Association commissioned Wuet al(2018) to examine 72 training programmes in 19 provinces that were developed to trial standardised GP resi—dency training by the National Health and Family Planning Commission.4In the 2017 annual evaluation report they found that most of the GP training programmes were complying with the training requirements, but 50% of hospitals had not established an independent GP department, and in many programmes,the GP training was indistinguishable from other disci—plines. The qualifications of the GP teaching faculty varied greatly as most were from other specialties and had not trained sufficiently in GP teaching. The report concluded the educational background and experiences of faculty in the community health centres needed improvement.4
Depending on the geographic location, GP residency training has different characteristics, financial support and training pathways in China. For example, in a survey of five well— known Chinese GP training institutions, the authors reported that the first GP residency training programme began in Beijing, and that Guangdong has the largest scale of training.5The degree of government financial support for GP training varies by province.For example, in 2012, the highest level of government financial support per programme amounted to ¥560 000(about US$88 900) in Chongqing, and ¥150 000 (about US$23 800) in Beijing,5while there was no financial support in Sichuan.5Lianet al6have documented eight pathways used to train general practitioners in China,but the government has encouraged mostly the ‘5+3'pathway.6The 5+3 pathway comprises 5 years of under—graduate training in medical sciences conferring a Bach—elor of Science degree and then 3 years of postgraduate and clinical training. In 2013, the government chose 64 medical colleges, including Peking University First Hospital, to pilot a “Four— Certificates— In— One programme”that encompasses a physician qualification certificate,standard residency training certificate, master's degree certificate and graduate certificate. Completion of the programme confers a higher level of qualifications based on additional requirements during residency.7
As GP residency training remains relatively new in China, the attitudes of GP residents about their training could provide a perspective on how the training process affects those the system is intended to educate. Previous literature concerning GP residency training has addressed a series of concerns including job burnout,8training satis—faction,9—11policy support, theory courses, and faculty qualifications,910opportunity to learn management of diseases,10personal values, income level, career devel—opment, social respect, and professional risk during GP residency training,1112as well as perspectives about GP residency training,9and factors affecting standardised training quality.13One previous qualitative study exam—ining work—family balance by women GP specialist trainees in Slovenia demonstrated they faced intense burdens at work and home.14Little current literature addresses the workload of GP residency training, the emphasis of training for GP, the impact of GP residency training on physical health and daily life, and gender issues in GP residency training. In addition, few previous studies have leveraged the benefits of mixed methods data collection to examine the GP residents' perspectives about their residency training which have been conducted in China.910Most articles have used pure quantitative methods,811or pure qualitative methods.14
Through this study, we sought to understand GP resi—dents' attitudes and perceptions about GP residency training, and further to compare the findings between two 5+3 GP residency programmes, one 5+3 programme piloting the ‘Four— Certificates— In— One' option in Beijing with the standard 5+3 residency training approach at the other programme in Shenzhen.
METHODS
Study design
We used a state— of— the— art mixed methods survey that was administered cross— sectionally in April 2019.15Our rationale for using a mixed data collection survey was the need to understand the views of residents across the programmes using the survey, to understand GP resi—dents' perspectives about the domains of interest and to link these findings together to achieve an understanding of the breadth and depth of opinions.
Setting
We selected two GP training programmes for study,the Departments of Peking University First Hospital in Beijing, a 5+3 programme also participating in the ‘Four—Certificates— In— One programme,' and Peking Univer—sity Shenzhen Hospital in Shenzhen, China, which is a straight 5+3 programme. Table 1 contrasts the Peking University First Hospital and Peking University Shenzhen Hospital relative to residency programme innovation,working environment, management, financial support and resident numbers.16—21
Data instrument and data collection
We distributed a survey used previously in comparisons of family medicine residents' attitudes about training in Japan and the USA,22and Ethiopia and the USA.23The orig—inal instrument addressed GP residents' demographics items, their attitudes towards GP residency training using 5— point Likert scale questions.2223We expanded on the 43 items used previously to create a 54— item survey to adapt for compelling contemporary issues in China. Specifi—cally, we added questions about future work prospects as a general practitioner (n=8), satisfaction with residency training (n=2) and one additional question about gender issues in GP residency training. We also included open—ended qualitative questions after each of the scales and a final open— ended qualitative question at the end of the survey to encourage resident reporting of their perspec—tives and experiences.
Participant recruitment and enrolment
We sent a recruitment email describing the study to all GP residents and recent graduates for whom there was contact information of the two study programmes. Partic—ipants met inclusion criteria for participation if they reviewed the consent for participation, clicked the survey link and answered the study questions. Residents who declined to click the link and complete the survey were excluded.

TabIe 1 Comparison of selected features of the innovative general practice training programme of Peking University First Hospital with the standard general practice training programme of Peking University Shenzhen Hospital in 2019
Data entry and analysis
Quantitative strand
The quantitative findings were downloaded from the web link into the statistical software SPSS V.16.0 and cleaned.The major study outcomes were resident satisfaction with their education, and how they differed between sites.Demographics were compared between hospitals using χ2tests or Fisher's exact test as appropriate. If the p value was less than 0.05, we interpreted this as a significant difference between these groups. Statistical analysis of the 5— point Likert scales comparing the residents' responses from the two sites was performed using independent group t— test for each of the seven major domains.
Qualitative strand
The qualitative data were downloaded into MSWord. The analysis was conducted using seven steps of the approach recommended by Bachuk.24The text was then translated into English by a study author (SL) to facilitate partici—pation of the international author. All translated English text segments were reviewed for fidelity to the original Chinese by a second author (MDF). As the amount of data was not excessive and did not require software, we analysed the text using manual coding with a priori codes based on the scales in the instrument, namely residency education, patient care, work independence, financial situation, personal situation, gender issues and future work as a general practitioner.
Mixed methods
As the qualitative questions were placed after each scale,we linked the qualitative findings to the overarching construct of each scale. We considered the quantitative and qualitative findings systematically such as to identify qualitative text to provide context for each scale while representing the breadth of responses, gender, and Chinese versus international background. We presented the mixed methods findings using a weaving approach,that is, quantitative scale and related qualitative find—ings addressing common constructs were considered together.24We examined the ‘fit' of the qualitative and quantitative data to look for confirmation, discordance and expansion.25
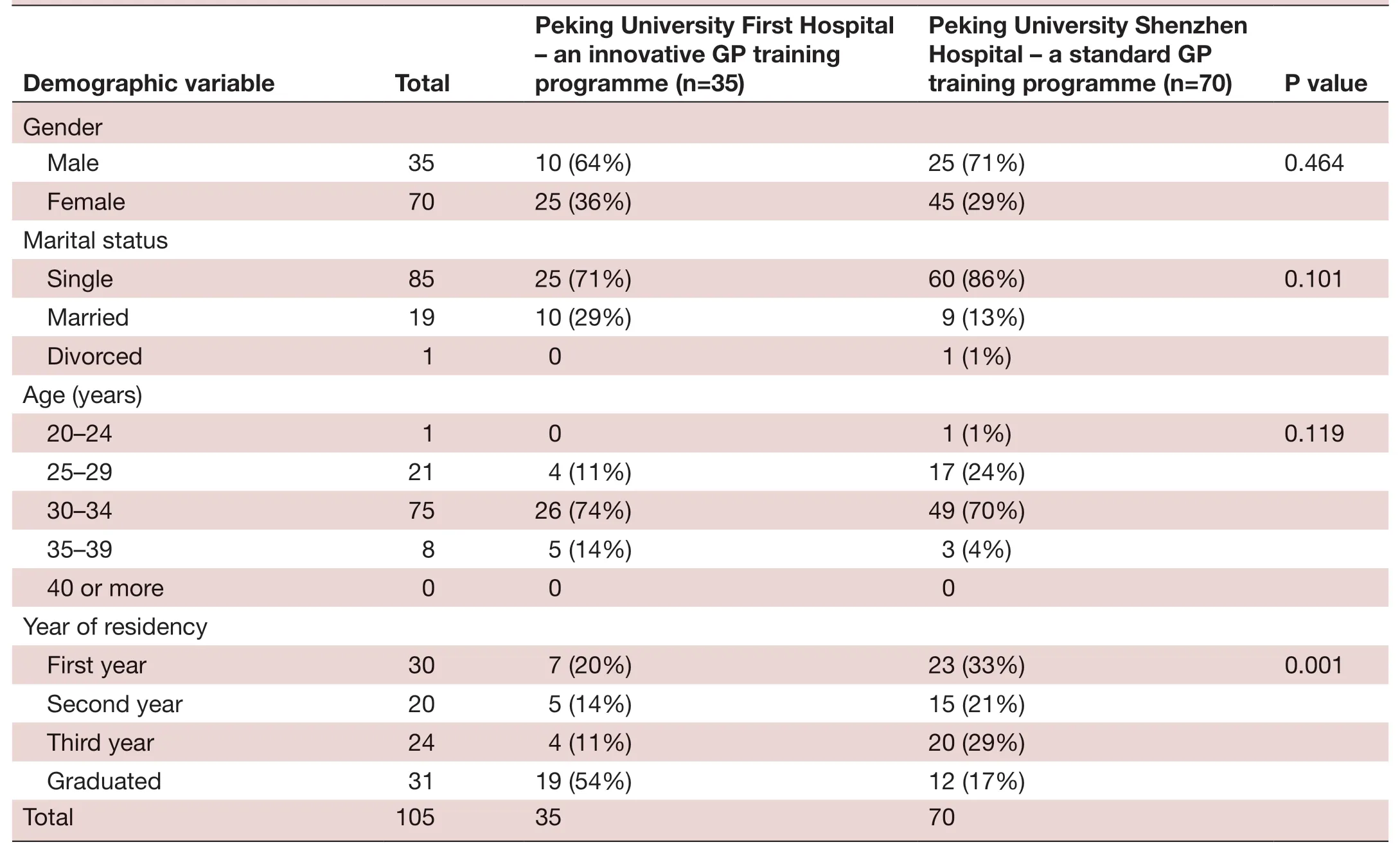
TabIe 2 Participant demographics in the innovative general practice training programme of Peking University First Hospital and the standard general practice training programme of Peking University Shenzhen Hospital
RESULTS
Demographics
The response rate at Peking University First Hospital was 90% (35/39) and at Peking University Shenzhen Hospital was 83% (70/84). There were no significant differences between the programmes relative to gender, marital status and age between Beijing and Shenzhen. The percentage of residency graduates who took the survey was signifi—cantly greater in Beijing than in Shenzhen (p=0.001)(table 2) consequent to a loss of contact information for some Shenzhen graduates.
Perceptions about resident education and patient care
Overall, the residents frequently felt that the curric—ulum needed clarification (mean 1.97, SD 0.904), and frequently or sometimes felt that outpatient training was inadequate (mean 2.4, SD 1.140) (table 3). About patient care, the residents frequently or sometimes felt that there were too many inpatients.
On average, Beijing residents more frequently felt satisfied with their education than Shenzhen (p=0.001).Five features of residency education attributes in Beijing were rated higher. Beijing residents felt more frequently that: their training programme would prepare them to work as a general practitioner (p=0.03), they had good role models (p=0.02) and teaching faculty had sufficient knowledge (p<0.001) and appropriate attitude towards GP training (p=0.004). In contrast, Shenzhen residents felt more frequently that their inpatient training was excessive (p=0.003) and that there were too many inpa—tients (p=0.01).
Qualitative comments about resident education were provided by 21 (60%) Beijing residents and 22 (28%)Shenzhen residents. Sixteen (45%) Beijing residents and 16 (22%) Shenzhen residents provided comments about patient care. Among them, four Beijing and 11 Shenzhen residents commented they needed more training time in outpatient care. But when care occurred, at least for some, there was another concern as voiced by a female Beijing resident who said:
There are too many outpatients to summarize the cases very well, and the teacher can't teach well. Buteven if there is time to teach, it is possible that they deal with cases in the specialist's way and cannot show general practitioners how to treat patients in clinic.Moreover, I hope my teachers can educate about con—sultation and follow— up skills which cannot be learned in the ward.
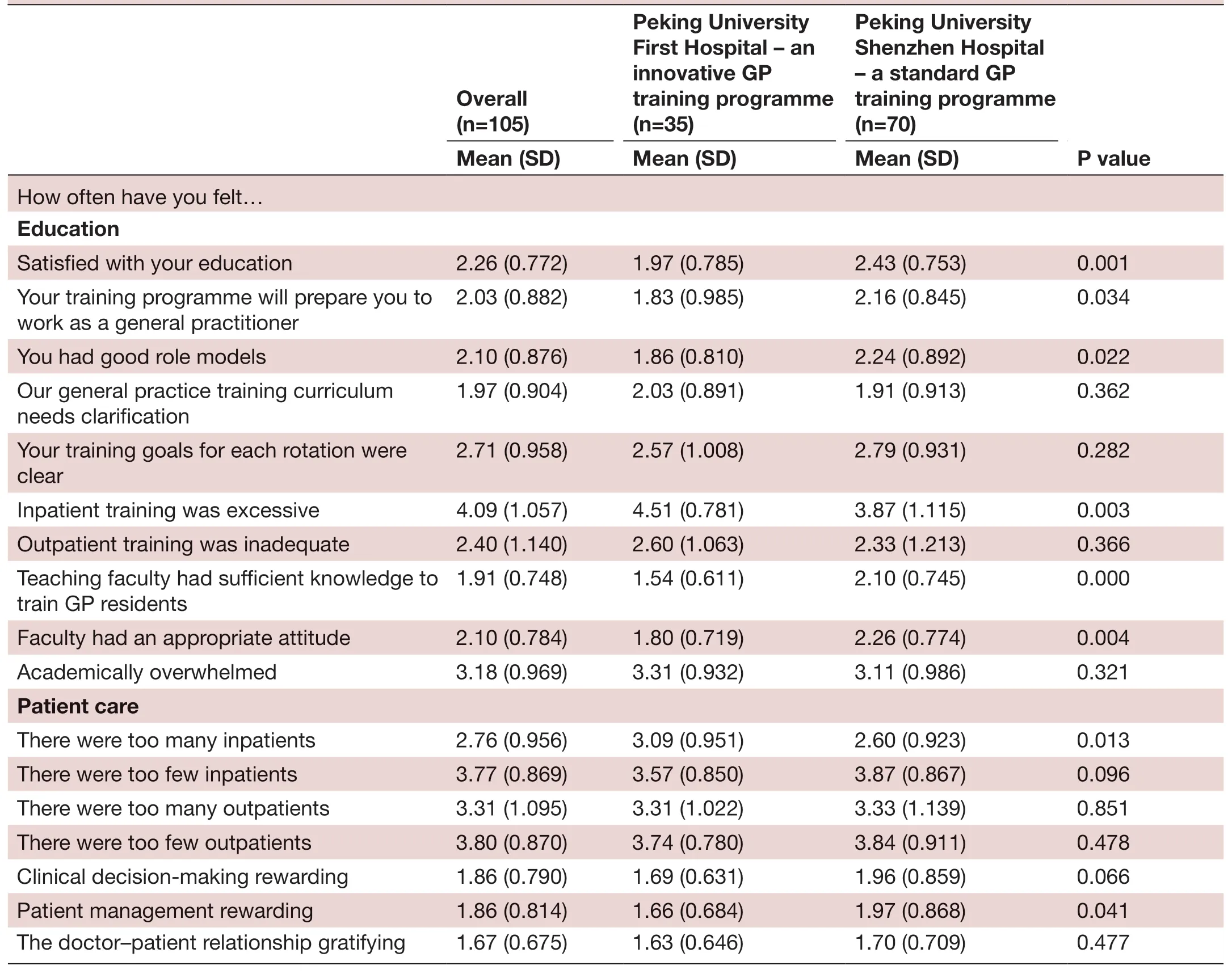
TabIe 3 Family medicine residents’ attitudes about residency education and patient care in the innovative general practice training programme of Peking University First Hospital and the standard general practice training programme of Peking University Shenzhen Hospital
One resident in Beijing and seven in Shenzhen commented about negative faculty attitudes. For example, a female resident from Shenzhen commented,‘A teaching faculty member said that the general practi—tioner's role is to care for colds, and coughs—the job is very relaxed. They also ignore GP residents. In this situa—tion, I felt discrimination.'
Perceptions about independence as GP residents
As shown in table 4, overall residents felt sometimes a ‘lack of self— identity as a general practitioner', ‘discrimination because of specialty choice' and ‘lack competency as a general practitioner'. As illustrated in table 3, there were no significant differences between Shenzhen and Beijing residents from perceptions about independence as GP residents. Qualitatively, 16 (45.7%) residents in Beijing and 16 (23%) in Shenzhen provided comments about independence as GP residents. One Beijing and four Shenzhen residents commented that they disagreed with managing patients independently during residency training for they were inexperienced. One male Beijing resident commented:
Nowadays, [regarding] the work of residents after Bachelor of Science degree, they cannot be giv—en much responsibility because their patient man—agement experience is limited. Asking for advice is necessary—as seniority grows, [they] can have more responsibility. But GP residents only have one year of rotations in the ward and will leave the ward after hav—ing grown up.
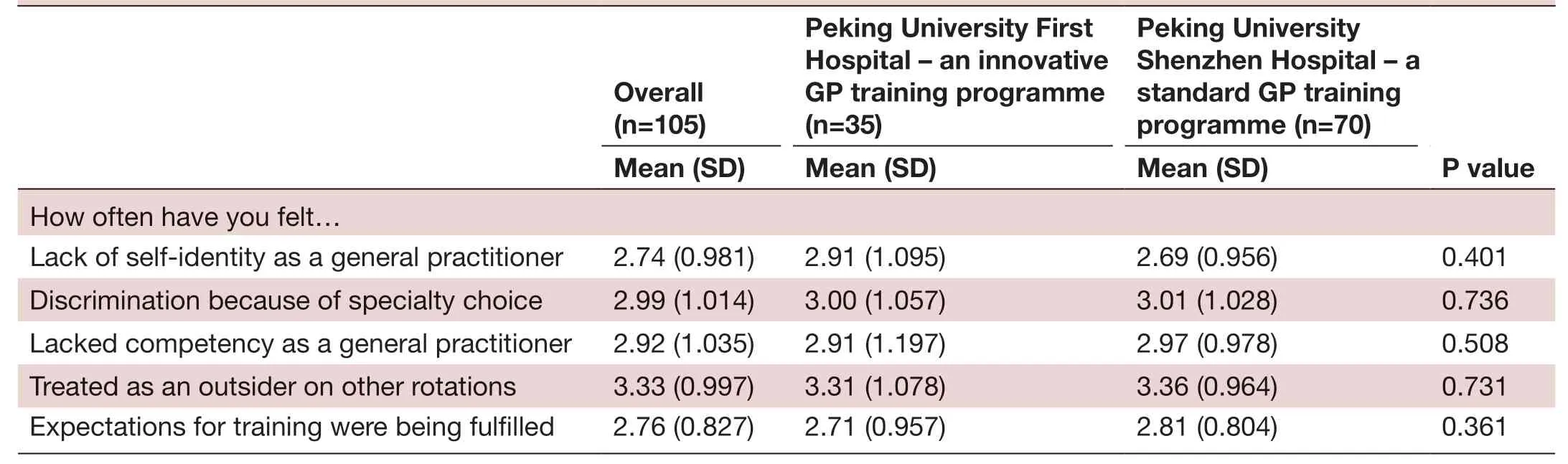
TabIe 4 Family medicine residents’ attitudes about independence as a general practice resident in the innovative general practice training programme of Peking University First Hospital and the standard general practice training programme of Peking University Shenzhen Hospital
Impact of residency training on personal life
As in table 5, the residents overall felt they lacked suffi—cient financial support during residency training (average score <3). About their personal life, residents sometimes felt sleep deprived. There were no significant differences between Shenzhen and Beijing residents relative to their perceptions about finances and personal lives (table 5).Qualitative responses about finances were provided by 22 (34%) Beijing residents and 12 (17%) Shenzhen residents. Six residents in Beijing and four in Shenzhen commented that their payment needed to be increased or was too low. For example, a female Beijing resident said, ‘Can improve the payment properly, after all, resi—dents do the most fatiguing work with the least salary.'Ten (29%) Beijing residents and 11 (16%) Shenzhen residents provided comments about their personal life.About their personal life, one Beijing and one Shenzhen resident felt despised or looked down on.
Perceptions about future work prospects
As shown in table 6, the residents agreed or were neutral that they would be respected by other physicians as a general practitioner in the future career. In the training programme comparison, Beijing residents on average were more positive on five items addressing future work optimism. They agreed at a higher level they would have job opportunities (p=0.005), would be able to practise the same spectrum of care as their training (p=0.02), would be paid fairly for their work as a general practitioner(p=0.003) and would be respected by patients (p=0.006)and other physicians in the future as a general practi—tioner (p=0.001).
Qualitative responses about future work as a general practitioner were provided by 10 (29%) Beijing residents and 7 (16%) Shenzhen residents. Five Beijing residents while only one Shenzhen resident commented working as a general practitioner would have a bright future. A female Beijing resident said, ‘The employment pros—pects in big cities are good.' Two Shenzhen residents and one Beijing resident commented the future is not good enough. A female Shenzhen resident commented:
[The future job] is not clear. Community clinics have too many administrative and public health jobs. At present, we have been doing clinic check— ups, regis—tration, recording data, filling out forms. We do not have any further understanding of GP. Now I have found a job, [and will] wait and see what happens.It is not in line with my expectations. I may look for opportunities to transfer to a hospital.
Three Beijing residents and one Shenzhen resident commented that the spectrum of training cannot prepare them to become a good general practitioner. Two Beijing and four Shenzhen residents demanded more respect from the society and other medical specialists. One female Beijing resident commented, ‘I hope to get the recognition from society, at least [respect for my] identity from peers.'
Gender issues in GP training
Overall, the residents felt gender issues arose infrequently(table 7). There were no differences between Beijing and Shenzhen residents on seven items about gender differ—ences. However, subanalysis by gender showed that in Shenzhen, male residents more frequently felt that being a female general practitioner provides an advantage(p=0.006), while female residents there more frequently felt that being a male general practitioner provides an advantage (p=0.05). Qualitative findings confirmed these findings. Ten (29%) Beijing and 7 (10%) Shenzhen residents responded about gender issues. Seven Beijing and two Shenzhen residents said treatment of males and females was the same.
DISCUSSION
GP is a discipline newly developing in China, still with limited numbers of residents and relative inexperience educating them.26As important stakeholders, GP resi—dents' attitudes provide an important reference for improving GP residency education.
Overall trends in attitudes across the two Chinese GP training programmes
Overall, the residents identify challenges of lack of respect, discrimination, achieving competency as general practitioners and negative teaching faculty attitudes.Their concerns are validated by previous literature. In large Chinese hospitals, doctors receive higher salaries,have higher reputations and have better career oppor—tunities than general practitioners.26The educational level in hospitals is higher than community health organ—isations.6These factors likely contribute to lower social status, but do not justify pejorative attitudes.
Feelings of incompetence seem attributable to a lack of sufficient clinical experience. While GP residents manage patients in the ward, they only have 1 year of ward rotations while other residents spend more time there. Currently, most GP residents only shadow in the clinic, while other residents can manage outpatients.These findings reinforce the importance of more hands on clinical experience for GP residents, of having trained teaching physicians as important for improving resident competency,27and for teaching faculty to have an unbi—ased attitude towards GP residents and give them equal opportunities to practise.
In a previous study examining family medicine resi—dent attitudes in Japan and America, faculty knowledge and teaching attitudes were associated with improved resident satisfaction.22Specifically, a sample of residents in America felt discrimination because of their choice of family medicine in 1991, but in 1995, both Japanese and American residents reported less feelings of discrim—ination.22These findings suggest that respect from other specialists can be improved. In Gossaet al's cross— national study of USA and Ethiopia (where family medicine only began in 2013), most differences in views about residency education among the US and the Ethiopian groups were overall not significant, but the Ethiopian residents were more frequently satisfied with their residency education than residents in a comparison programme in the USA(p=0.07).23These findings imply that even if the educa—tion system is in an early stage of development, resident satisfaction with education can be influenced positively depending on the circumstances of the program.

TabIe 6 General practice residents’ attitudes about work prospects according to training site and respondent gender in the innovative general practice training programme of Peking University First Hospital and the standard general practice training programme of Peking University Shenzhen Hospital
Differences between the two programmes
Compared with the standard 5+3 programme of Shen—zhen, Beijing residents who benefit from the 5+3 and Four—Certificates— In— One programming more frequently felt satisfied with their education, and that teaching faculty had sufficient knowledge and appropriate teaching atti—tudes. Even though most teaching faculty in GP in Beijing are from other specialties and lack experience teaching GP residents, their affiliation with the culture of the academically rigorous Peking University Health Science Center might influence teaching faculty knowledge and training attitudes. The GP training system in Peking University First Hospital improved after strict selection of faculty.18Nearly 20 specialists who were candidates to become GP resident teaching faculty took part in transfer training, but only half of them earned a GP certificate,a status conferring qualification to work in a GP clinic.These findings support the importance of educating other specialists as GP trainers.28
Overall, Beijing residents more favourably perceived their future job prospects as general practitioners. While we cannot conclusively attribute causality of the differ—ences to availability of the Four— Certificates— In— One system, these findings suggest that the intensive training of faculty, and the additional opportunities through the‘Four— Certificates— In— One' programme positively impact Beijing resident optimism about job prospects compared with Shenzhen residents who lack the same opportunity.
These differences aside, for the majority of items exam—ined, for example, training content, finances, personal life and gender issues, there were no substantial differ—ences between the residents' attitudes in Beijing and Shenzhen. Indeed, the residents in both programs indi—cated favourable ratings for a number of items. The lack of differences suggests their overall ratings may reflect the status of GP training in China more generally. For example, in Liu's study in Shanghai, 55.8% (125/224)of residents felt their outpatient time was insufficient,54.0% (121/224) of residents wanted more opportunities to manage patients independently and 24.3% (111/457)of GP residents felt the teaching faculty did not have suffi—cient understanding of general medicine philosophy.9In Wanget al's study, 59.4% (76/128) of GP residents felt the educational content was too specialised.11
Addressing the challenge of other specialist discrimination
These findings illustrate a problem with, or at least the perception of specialists discriminating against GP resi—dents. In Huanget al's (2018) study, among 768 GP resi—dents, only 57.8% (n=444) reported they would like to continue to work as general practitioners in the future,and overall, they reported negative attitudes about the level of social respect.13Among 288 medical students in Wanget al's11study, 24.7% (n=71) of students felt general practitioners had lower social status, and 28.5% (n=65) of students felt general practitioners could not gain respect from other physicians.29Unfortunately, similar challenges exist even in mature international settings.
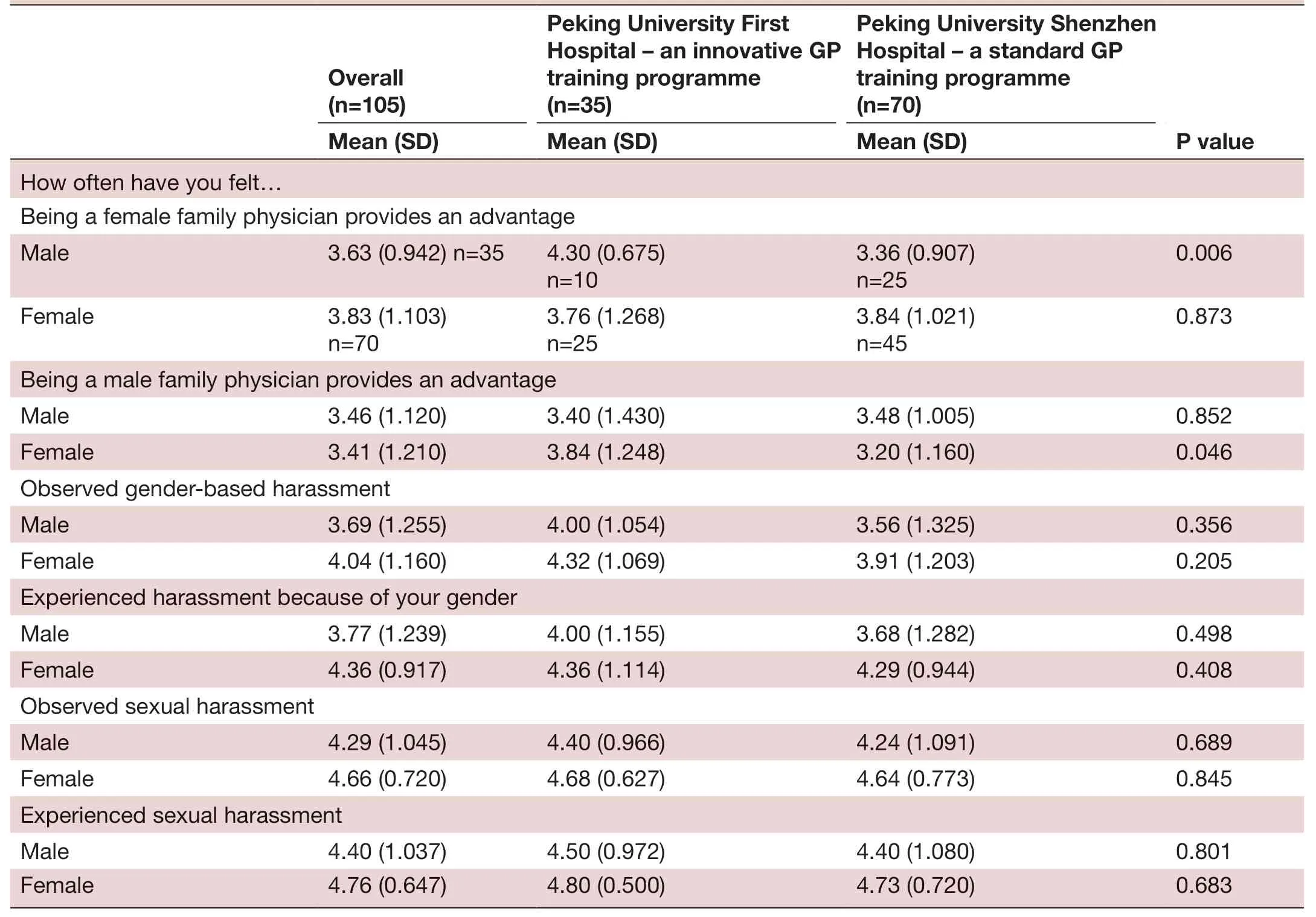
TabIe 7 General practice residents’ attitudes about gender issues according to training site and gender of the respondents in the innovative general practice training programme of Peking University First Hospital and the standard general practice training programme of Peking University Shenzhen Hospital
On the bright side, it appears proactively intervening can improve relations. In Alberta College, Canada, family physicians perceived a lack of respect.30An intervention implemented by the faculty of medicine department and family medicine department improved relation—ships between general practitioners and other specialists;improved support of each other's roles; changed negative attitudes by promoting the expertise and role of family medicine to others; and demonstrated maintenance of comprehensive skills.30
Strength and limitations
To our knowledge, this study represents the first inten—tionally designed mixed data collection survey in the field of primary healthcare in China. The study demon—strates one example of many mixed methods research designs that can be used in primary healthcare.3132The use of scales followed by qualitative questions to provide a more comprehensive understanding about the construct of interest provides a model for other researchers to use in mixed data collection surveys.In this study, the quantitative findings measured the frequency of attitudes about survey items, and allowed for statistical comparison between the two programmes.In addition, the qualitative findings provided a more nuanced understanding about the study scale results.We recommend researchers in other countries consider using mixed methods designs in their work to fully explore the complexities of traning and clinical practice.A mixed methods approach may be particularly useful for investigating the complexity and reality of issues in low and middle— income countries.
While the study was conducted in only two residency sites, these were chosen specifically to compare two 5+3 programmes, one with the Four— Certificates— In— One educational innovation versus a typical programme.Future research in more programmes with this innova—tion could provide additional insight, though many of these findings resonate with previous resident surveys in Japan and the USA,22and Ethiopia and the USA.23
CONCLUSIONS
Creating and nurturing respectful relationships between general practitioners and other specialists connotes a critical priority for alleviating many challenges in GP training. These findings show higher satisfaction with faculty teaching and higher job optimism in the Beijing programme with educational innovations. In sum, these findings reinforce the value of educational innovations for enhancing training and promoting optimism among residents for future work as general practitioners.
Twitter Michael D Fetters @mdfetters
Acknowledgements The authors gratefully acknowledge Melissa A. Plegue, who provided statistical consultation guiding the analysis.
Contributors SL, YX, CC and MDF contributed to the planning of the study. SL, YX,JZ and XH contributed to collection of data for the study. SL, YX, JZ, XH, CC and MDF contributed to the authoring and reporting of the study findings.
Funding This study was funded by University of Michigan Medical School.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was reviewed and approved by the Peking University First Hospital Human Research Ethics Committee. Ethical review number: (2019)Scientific research number 89.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iD
Michael D Fetters http:// orcid. org/ 0000- 0001- 8521- 5681
 Family Medicine and Community Health2019年4期
Family Medicine and Community Health2019年4期
- Family Medicine and Community Health的其它文章
- Association of metabolic NCD risk factors with oral, breast and cervical precancers and cancers in India
- Exploring the influencing factors for non- utilisation of healthcare facilities during childbirth: a special mixedmethod study of Bangladesh and 13 other low- and middle- income countries based on Demographic and Health Survey data
- Improving patient satisfaction through improved telephone triage in a primary care practice
- Improving sexual and reproductive health knowledge and practice in Mozambican families with media campaign and volunteer family health champions
- Factors for self- assessment score of interprofessional team collaboration in community hospitals in Japan
- How French general practitioners adapt their care to patients with social difficulties?