
The effect of empowerment education on depression level and laboratory indicators of patients treated with hemodialysis: a meta-analysis
2019-10-17 03:38:02YuNanJiYanHuiLiuLingLiXieChenYangLiZhenHuaHou
Frontiers of Nursing 2019年3期
Yu-Nan Ji, Yan-Hui Liu, Ling-Li Xie, Chen-Yang Li, Zhen-Hua Hou
School of Nursing, Tianjin University of Traditional Chinese Medicine, Tianjin 300193, China
Abstract: Objective: The objective of this study was to evaluate the effect of empowerment education on depression level and laboratory indicators of patients treated with hemodialysis.Methods: We searched databases including Cochrane Library, Web of Science, Embase, PubMed, Chinese Biomedical Literature Database (CBM), Chinese Academic Journals Full-text Database (CNKI), VIP, and Wanfang. We included all the researches about the application of empowerment education in patients treated with hemodialysis. We used RevMan 5.3 to analyze the data after assessing the quality of researches.Results: We included 10 studies eventually. The results of meta-analysis showed that the self-eff i cacy [MD = 1.10, 95% conf i dence interval (CI; 0.71, 1.48), P < 0.01], depression [MD = -6.94, 95% CI (-8.53, -5.34), P < 0.01], serum creatinine [Scr; MD = -116.46,95% CI (-171.90, -61.03), P < 0.01], albumin [Alb; MD = 2.93, 95% CI (2.00, 3.86), P < 0.01], and blood urea nitrogen [BUN;MD = -0.95, 95% CI (-1.89, -0.01), P = 0.05] in the empowerment education group had signif i cantly statistical difference compared with those in the usual education group. However, there was no signif i cant difference in hemoglobin [Hb; MD = 3.03, 95% CI (-0.64,6.70), P = 0.11] between two groups.Conclusions: Empowerment education can improve the self-eff i cacy in patients treated with hemodialysis, relieve depression, and improve Scr, Alb, and BUN. However, there is no signif i cant improvement in Hb; it needs further exploration in clinical practice.
Keywords: empowerment education · hemodialysis (HD) · depression · laboratory indicators · meta-analysis
1. Introduction
At present, with the increase in the incidence of endstage renal disease, the number of hemodialysis patients in China is increasing, even is higher than the growth rate of the world.1As a long-term traumatic replacement therapy, hemodialysis not only reduces the patient's related symptoms and prolongs the survival period but also causes a variety of physiological and psychological problems in the patient, which seriously affects his or her quality of life.2,3A study4has shown that depression is a common emotional disorder in maintenance hemodialysis patients, with an incidence of 30%-100%. As a new model of health education, empowerment education has changed the passive obedience of the patients in the traditional education and makes the passive patients to be active, and it also can manage the self-management.5In recent years, empowerment education has shown a good effect on improving biochemical indicators such as glycosylated hemoglobin (Hb).6Research on the application of empowerment education in hemodialysis patients has also been deepened and has attracted more and more attention. The study of McCarley7shows that empowerment can stimulate self-care and self-management in hemodialysis patients. A qualitative study of the empowerment education in 27 hemodialysis patients by Christian et al.8found that the patient's satisfaction with the empowerment process is 100%, and half of the respondents said that they were willing to participate in the empowerment education.
However, there are still differences in the role of Hb and other biochemical indicators in hemodialysis patients, and most of the studies have the problems of relatively small sample size and scattered cases. Therefore, the purpose of this study was to evaluate the effect of empowerment education on self-efficacy, depression,blood creatinine, Hb, albumin (Alb), and other biochemical indicators of hemodialysis patients by meta-analysis.These can provide a reference for further clinical study of the empowerment education intervention for hemodialysis patients.
2. Design and methods
2.1. Inclusion and exclusion criteria
2.1.1. Study type
Randomized controlled trials (RCTs) or class experiments in both Chinese and English were eligible for inclusion in this meta-analysis.
2.1.2. Study objective
The inclusion criteria were as follows: ① Conduct regular hemodialysis for at least 3 months; ② have communication abilities and be able to understand and cooperate with; ③ volunteers to participate in the study;and ④ age ≥18 years. People with mental illness and mental handicap were excluded.
2.1.3. Study intervention
Empowerment education was provided to hemodialysis patients in the experimental group. Empowerment education contained contents such as related knowledge about hemodialysis; diet management, such as the importance and principles of diet, exercise; appropriate use of medicines; and management of negative emotions. The traditional education was adopted in the control group.
2.1.4. Outcome measures
The outcome measures were self-efficacy [the Chronic Disease Management Self-Efficacy Scale and Strategies Used by People to Promote Health (SUPPH)],depression [Self-Rating Depression Scale (SDS)], and blood biochemical indicators [Hb, Alb, serum creatinine(Scr), blood urea nitrogen (BUN), empowerment level,and Empowerment Scale (ES)].
2.2. Search strategy
We used computer to search some databases such as Cochrane Library, Web of Science, PubMed, Chinese Biomedical Literature Database (CBM), Chinese Academic Journals Full-text Database (CNKI), VIP Database (VIP) and Wanfang Data Knowledge Service Platform. The retrieval time was from the establishment of the database to November, 2017. English search terms were empower*, empowerment theory, empowerment education, renal dialysis, renal dialyses, hemodialysis, hemodialyses, haemodialysis, haemodialyses,extracorporeal dialyses, extracorporeal dialysis, and hemodiaf i ltrat*; Chinese search terms were empowerment theory, empowerment education; hemodialysis hemodialysis, hemodiaf i ltration, hemof i ltration, plasma exchange, and blood perfusion. MeSH subject terms,free words, and Boolean operators were used to combine word combinations; corresponding search-based search literatures were formulated based on different databases; and references included in original documents and related reviews were referred to determine other relevant literature.
2.3. Data extraction
Two researchers independently selected the literature according to the inclusion and exclusion criteria, crosschecked after extracting the literature data, and if there were any objections, they were resolved through arbitration by the third researcher. According to the content of the literature, a data extraction form was prepared.The extracted contents included the included literature,publication time, sample size, interventions, intervention time, and data extraction time and outcome indicators.
2.4. Risk of bias assessment
Two investigators evaluated the quality of the included literature according to the Cochrane Handbook Quality Standards 2011. The evaluation items included random sequence generation, allocation concealment, blinding of study subjects and implementers, blinding of outcome measurers, completeness of result data, selective reporting of study results, and other sources of bias.According to the above criteria, each article included was evaluated one by one using “low risk of bias”, “high risk of bias”, or “unclear”. Literature quality was divided into three levels: A, B, and C. The characteristics of “Grade A” were low biased and fully satisfying the above quality standards, “Grade B” were moderately biased and partially satisfying the above quality standards, and “Grade C” were highly biased and completely dissatisf i ed with the abovementioned quality standards; such documents were excluded. After independently evaluating the quality of the literature, two researchers discussed the quality of each study based on the above evaluation criteria and reached a consensus to form the fi nal evaluation of the quality of the literature. If there were differences, the third researcher arbitrated.
2.5. Statistical analysis
RevMan 5.3 software was used for meta-analysis. Measured data were expressed as the weighted mean difference (MD) or standardized mean difference (SMD) and its 95% conf i dence interval (CI). Count data used relative risk (RR) or odds ratio (OR) and 95% CI. The heterogeneity between the results of the included studies was determined using the Q test, and the effectivity values were analyzed for heterogeneity. If there was no statistically signif i cant heterogeneity between studies (P > 0.1,I2< 50%), a fi xed-effects model was used. If there was statistical heterogeneity (P < 0.1, I2≥ 50%), these factors, which may lead to heterogeneity, were analyzed in subgroups. If there was a statistical difference and no clinical heterogeneity between the two groups, or difference was not statistically signif i cant, a random effects model was used to combine the effect sizes. If the heterogeneity was too obvious and the source could not be judged, a descriptive analysis was performed.
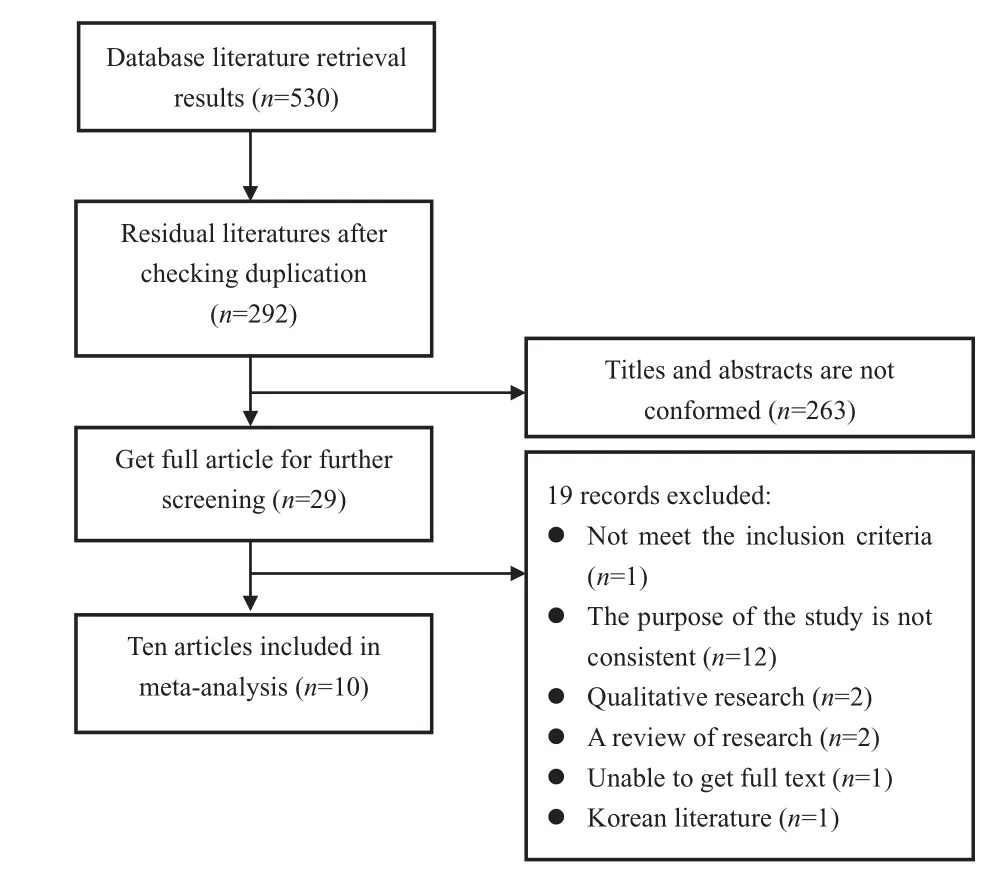
Figure 1. Flow chart of the study selection procedure.
3. Results
3.1. Study selection
A total of 530 reports in literature were retrieved, including 106 Chinese studies and 424 English studies. After removing duplicate literature with NoteExpress, there were 292 studies, including 41 in Chinese and 251 in English; after reading the title, abstract, and full text,the studies that did not meet the inclusion criteria were deleted, and fi nally, 10 studies were identif i ed. See Figure 1 for details.
3.2. Methodological quality
For the 10 studies included, the total sample size was 817; the basic characteristics of the included studies are given in Table 1. The quality of the 10 studies included was evaluated by the Cochrane Systematic Review Manual 5.1.0. Some of the studies were lost to follow-up, but all were explained. Among the 10 studies included in the results, one had a quality rating of A and the others had a quality rating of B. See Table 2 for details.
3.3. Primary outcomes
3.3.1. Effect of empowerment education intervention on self-ef fi cacy
Eight studies9,10,12-14,16-18used the Chronic Disease Management Self-Efficacy Scale or Strategies Used by People to Promote Health (SUPPH) to measure the impact of empowerment education intervention on the self- efficacy of hemodialysis patients. Efficacy scales have good reliability and validity. The combined results showed that there was statistical heterogeneity among the studies (P < 0.1, I2= 81%), so the random effects model was used for meta-analysis. The results showed that the self-efficacy score of the empowerment education group was higher than that of the control group, and the difference was statistically signif i cant [MD = 1.10,95% CI (0.71, 1.48), P < 0.01]. That is, empowerment education intervention can improve the self-efficacy of hemodialysis patients. Taking into account the greater heterogeneity, the included studies were grouped into subgroup analyses by data collection time. The results showed that measured for 6 weeks in hemodialysis patients, empowerment education intervention can improve the self-efficacy of hemodialysis patients[MD = 8.83, 95% CI (5.49, 12.17), P < 0.01] and measured for 3 months in hemodialysis patients, education intervention can improve self-efficacy [MD = 0.62, 95% CI(0.43, 0.81), P < 0.01]; 6-month self-efficacy of hemodialysis patients can also be improved in empowerment education interventions [MD = 1.39, 95% CI (1.17, 1.61),P < 0.01] (see Figures 2-4).
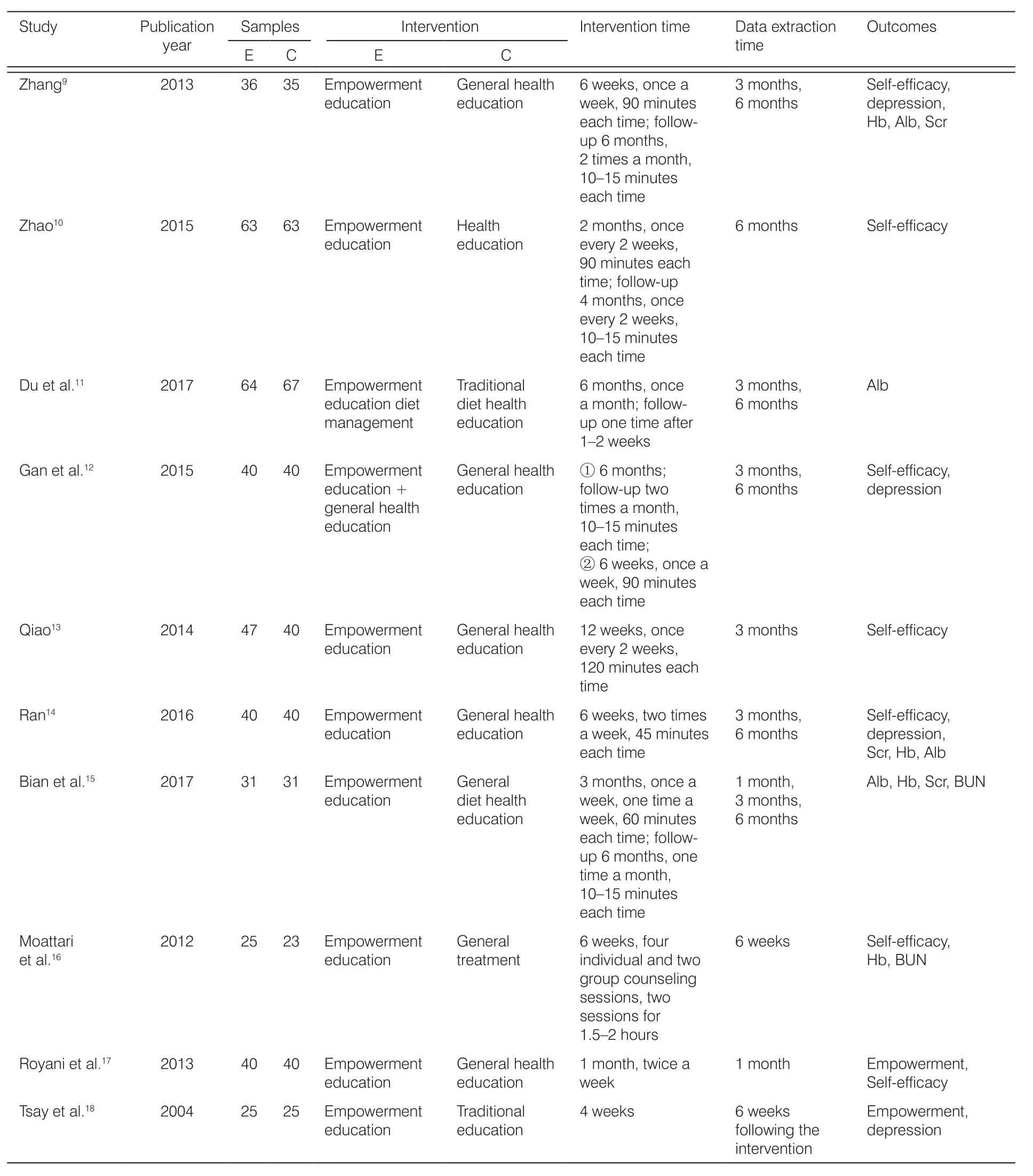
Table 1. Basic characteristics of the included studies.
3.3.2. Effect of empowerment education intervention on depression level
All three studies9,12,14used depression self-rating scales to measure the level of depression in hemodialysis patients. The combined results showed that there was no statistical heterogeneity between the studies(P = 0.17, I2= 35%), so a fi xed-effect model was used for meta-analysis. The results showed that the level of depression in the empowerment education intervention group was lower than that in the control group and the difference was statistically signif i cant [MD = -6.94, 95%CI (-8.53, -5.34), P < 0.01], namely, empowerment education can alleviate depression in hemodialysis patients. Because the intervention time was 3 months
and 6 months, a subgroup analysis was conducted to investigate the effects of interventions at different times on the level of depression in hemodialysis patients.The results showed that 3 months and 6 months of empowerment education intervention could alleviate the depression of hemodialysis patients [3 months:MD = -4.62, 95% CI (-6.90, -2.33), P < 0.01; 6 months:MD = -9.14, 95% CI (-11.36, -6.91), P < 0.01] (see Figure 5).
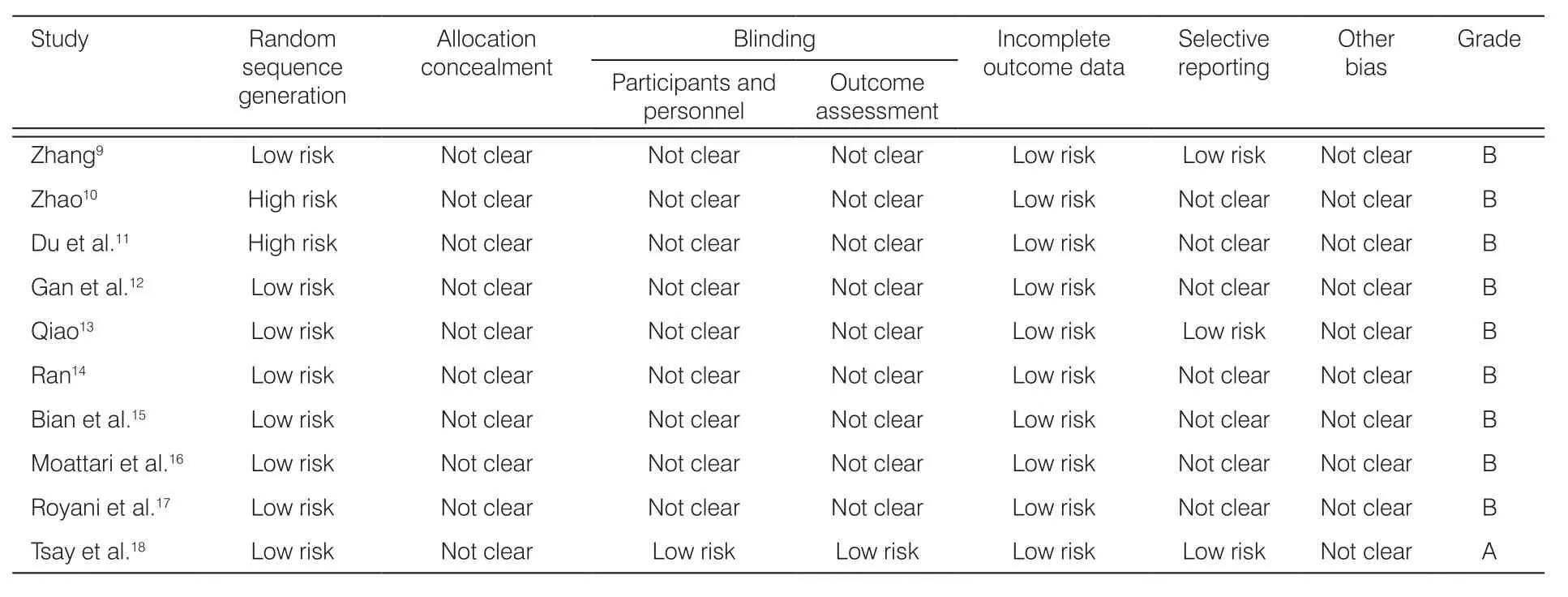
Table 2. Methodological quality assessment of included studies.
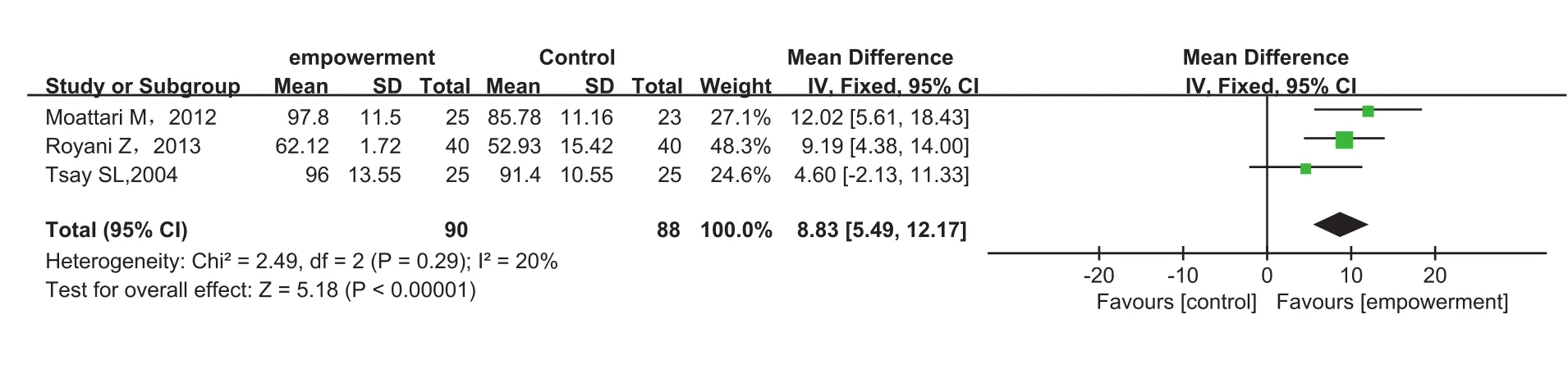
Figure 2. Comparison of 6-week self-eff i cacy between empowerment education intervention group and traditional education group.
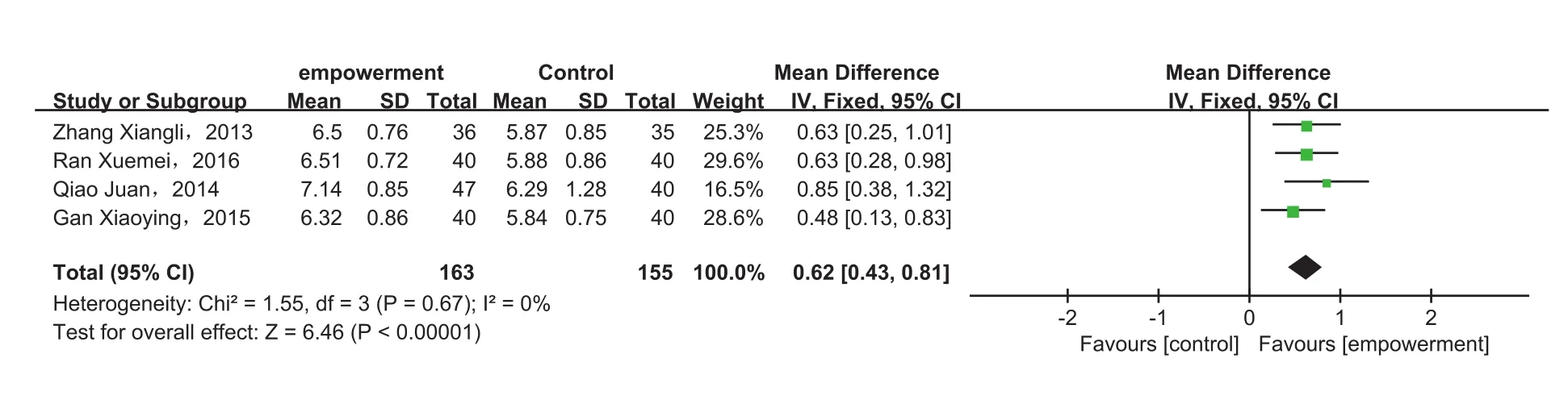
Figure 3. Comparison of 3-month self-eff i cacy between empowerment education intervention group and traditional education group.
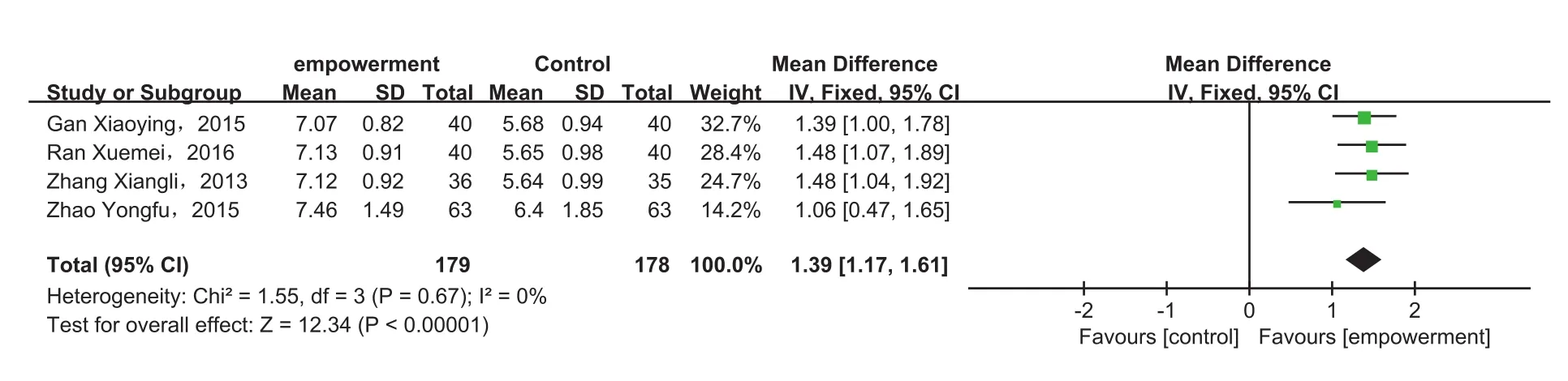
Figure 4. Comparison of 6-month self-eff i cacy between empowerment education intervention group and traditional education group.
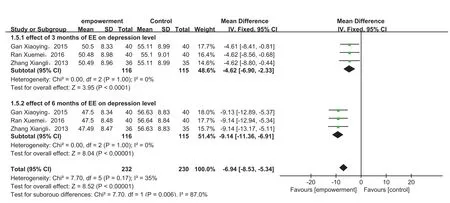
Figure 5. Comparison of depression levels between empowerment education intervention group and traditional education group.
3.3.3. Effect of empowerment education intervention on blood biochemical indexes
3.3.3.1. Effect of empowerment education intervention on Hb
Four studies9,14-16compared the effects of empowerment education intervention on Hb in hemodialysis patients. The combined results showed that there was statistical heterogeneity among the studies (P = 0.02,I2= 60%), so a random effect model was used for meta-analysis. The results showed that there was no statistically signif i cant difference between the empowerment education intervention group and the control group [MD = 3.03, 95% CI (-0.64, 6.70), P = 0.11]. Considering the greater heterogeneity, the included studies were divided into 1 month of Hb group, 3 months of Hb group, and 6 months of Hb group according to the time of data collection. The results showed that the combined effects were not statistically signif i cant[1 month: MD = 8.57, 95% CI (-12.07, 29.22), P = 0.42;3 months: MD = 2.69, 95% CI (-3.12, 8.51), P = 0.36;MD = 2.01, 95% CI (-2.03, 6.05), P = 0.33], namely,empowerment education intervention has no signif icant effect on improving Hb in hemodialysis patients(see Figure 6).
3.3.3.2. Effect of empowerment education intervention on Alb
Four studies9,11,14,15evaluated the effects of empowerment education on Alb in hemodialysis patients. The combined results showed that there was no statistical heterogeneity among the included studies (P = 0.009,I2= 60%), so a random effect model was used for metaanalysis. The results showed that there was a statistically signif i cant difference between the empowerment education group and the control group [MD = 2.93, 95% CI(2.00, 3.86), P < 0.01]. Considering the heterogeneity among the studies, a subgroup analysis was performed according to the data collection time. The results showed that there was no heterogeneity between the subgroups (3 months Alb: P = 0.21, I2= 33%; 6 months Alb: P = 0.15, I2= 44%); in addition, difference of each subgroup between the intervention group and the control group was statistically signif i cant [3 months: MD = 2.86,95% CI (1.99, 3.74), P < 0.01; 6 months: MD = 3.70,95% CI (2.81, 4.59), P < 0.01], that is empowerment education intervention can improve Alb index in hemodialysis patients. Since only one study was reported in the 6-week Alb subgroup, no subgroup analysis was performed (see Figure 7).
3.3.3.3. Effect of empowerment education intervention on serum creatinine
Three studies9,14,15reported the impact of empowerment education intervention on serum creatinine in hemodialysis patients. The combined results showed that there was statistical heterogeneity among the included studies (P < 0.1, I2= 74%), so a random effect model was used for meta-analysis. The results showed that there was a statistically signif i cant difference between the empowerment educational intervention group and the control group [MD = -116.46, 95% CI (-171.90, -61.03),P < 0.01]. Taking into account the heterogeneity between studies, the included studies were subgrouped according to the time of data collection. The results showed that there was a statistically signif i cant difference between the empowerment education intervention group and the control group among the subgroups[3 months: MD = -84.84, 95% CI (-143.89, -25.79),P < 0.01; 6 months: MD = -144.97, 95% CI (-258.72,-31.21), P < 0.01], that is, empowerment education intervention can improve the serum creatinine index in hemodialysis patients (see Figure 8).
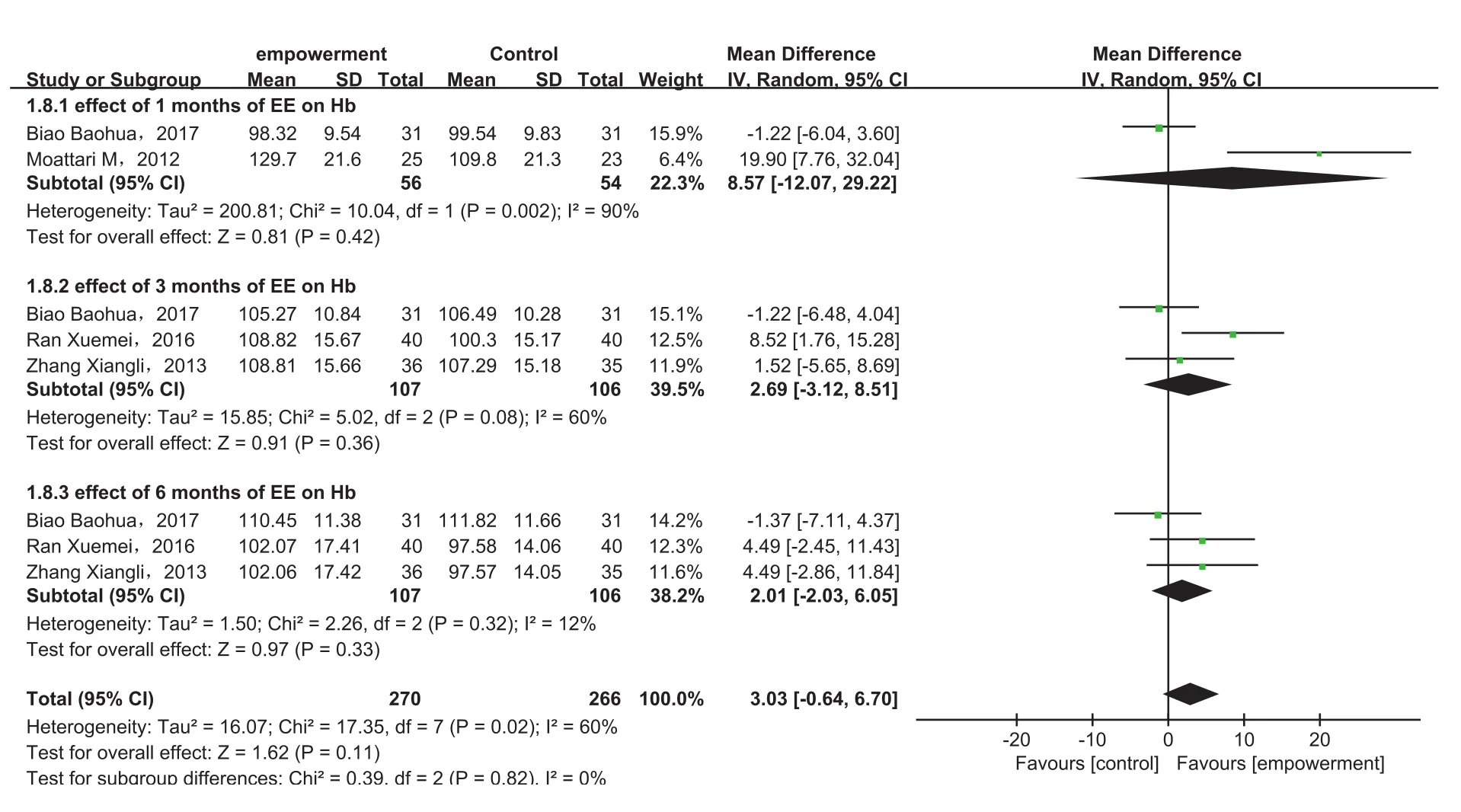
Figure 6. Comparison of hemoglobin between empowerment education intervention group and traditional education group.
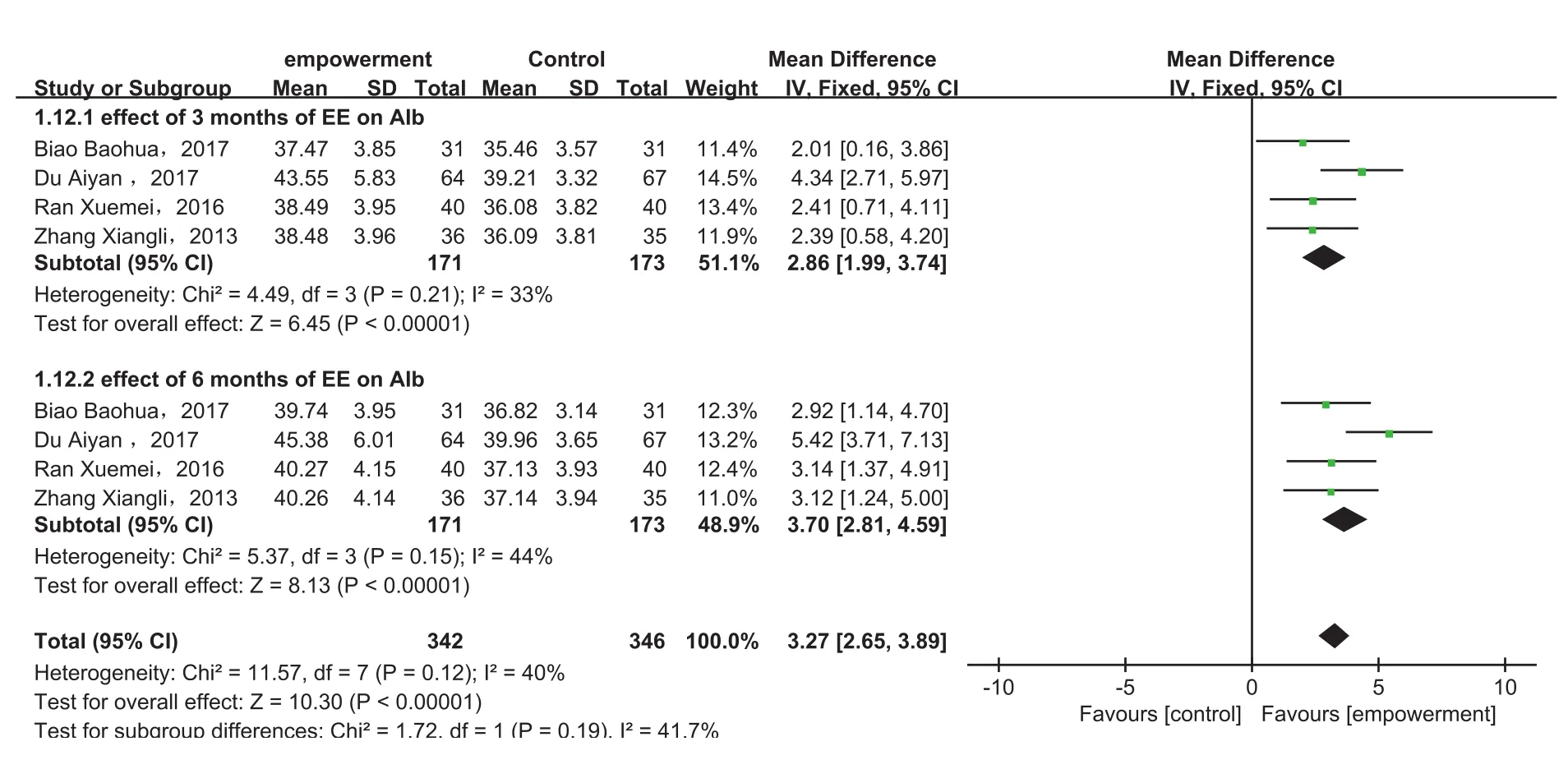
Figure 7. Comparison of albumin between empowerment education intervention group and traditional education group.
3.3.3.4. Effect of empowerment education intervention on BUN
Two studies15-16evaluated the impact of empowerment education intervention on BUN indexes in hemodialysis patients. The combined results showed that there was no statistical heterogeneity between studies (P = 0.35,I2= 0%), so a fi xed-effects model was used to perform a meta-analysis. The results showed that empowerment education intervention can improve the urea nitrogen index in hemodialysis patients [MD = -0.95, 95% CI(-1.89, -0.01), P=0.05].
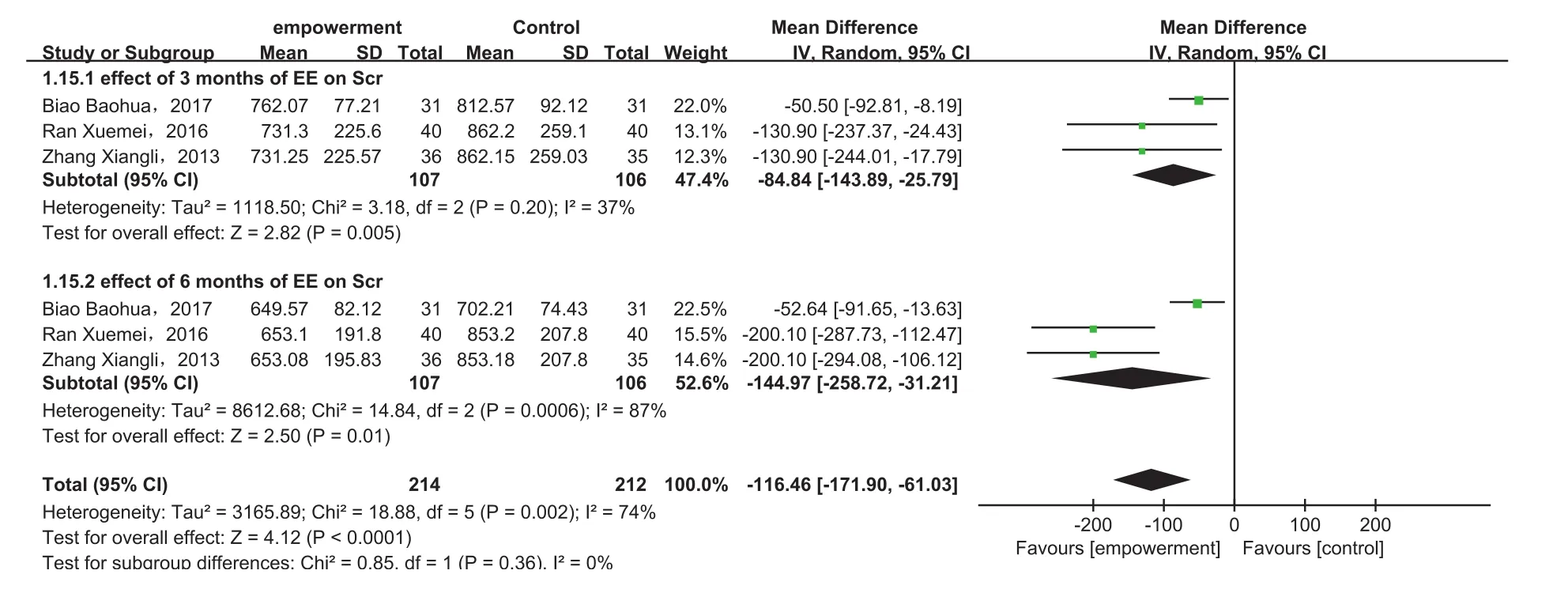
Figure 8. Comparison of serum creatinine between empowerment education intervention group and traditional education group.
3.3.3.5. Effect of empowerment education intervention on empowerment level
Two studies17,18evaluated the impact of empowerment education intervention on the empowerment of hemodialysis patients. The combined results showed statistical heterogeneity among studies (P = 0.31, I2= 3%), so a fi xed-effects model was used. The analysis results show that the level of empowerment level between the empowerment education group and the traditional education group has statistical signif i cance, namely, empowerment education intervention can improve the empowerment level of hemodialysis patients [MD = 5.76, 95% CI(4.18, 7.34), P < 0.01].
4. Discussion
4.1. Methodological quality
A total of 10 studies were included in this study. One study had a quality rating of A. The rest had a quality rating of B. The overall quality was moderate and may be related to the stringency of the randomized interventions included in the literature. The included studies used a randomization method, but most studies did not describe the specif i c randomization method, and the included studies did not specif i cally describe the allocation concealment and blinding methods, so there may be a certain offset, and therefore, we should pay attention to the concealment and endgame blindness when we make some related researches.
4.2. Effect of empowerment education intervention in hemodialysis patients
Empowerment education is an education model in which patients are the whole body and they can participate in decision-making. In fact, educators and patients become friends and cooperate with each other to formulate nursing plans together.19Its intervention is mainly carried out through fi ve steps,20namely, clarifying problems, expressing emotions, setting goals, setting plans,and evaluating results. Each step is crucial. In addition,attention should be paid to clarifying the issues and expressing emotions, always insisting on people centeredness, and paying attention to the patient's own wishes, emotions, and needs.21In this study, metaanalysis was used to evaluate the impact of empowerment education intervention on hemodialysis patients'self-efficacy, depression, and serum, creatinine, Alb,and other biochemical indicators. The results showed that empowerment education can improve self-efficacy,relieve depression, and improve related indicators. The reason may be that hemodialysis patients can vent their bad feelings, face their own health problems correctly,and make correct choices and positive changes.
In assessing the role of empowerment education interventions in the self-efficacy of hemodialysis patients, subgroup analyses were performed considering the heterogeneity. In the 6-week intervention selfefficacy subgroup, self-efficacy was evaluated using the self-efficacy (SUPPH) scale and the remaining subgroups were all managed using the Chronic Disease Management Self-Efficacy Scale. In addition, the study10on empowerment education interventions for depression indicators in hemodialysis patients, using the Hospital Anxiety and Depression Scale. Blood biochemical indicators are important indicators for evaluating the nutritional status of hemodialysis patients.Attention should be paid to the conversion of each unit when data are extracted, and data analysis can only be performed when the units are consistent. In this study,serum creatinine, Alb, Hb, BUN, and other biochemical indicators are commonly used in domestic units, which are μmol/L, g/L, g/L, and mmol/L, respectively. The meta-analysis showed that empowerment education had a certain improvement on serum creatinine, urea nitrogen, and Alb, probably because empowerment education was based on the individualized implementation plan of the patients. The patients' own problems were clearer. However, there was no statistically signif i cant difference in Hb between the empowerment education group and the control group. The analysis of the causes may be related to the treatment with erythropoietin, and it also may be different investigator or intervention program.
5. Conclusions
This study shows that empowerment education intervention can improve the self-efficacy, relieve the depressed mood, and improve the laboratory indicators such as serum creatinine, Alb, and urea nitrogen in hemodialysis patients, but there is no obvious improvement in the Hb index. In addition, the contents of empowerment education intervention and the intervention time for hemodialysis patients have not yet been concluded. Therefore,more large-scale, high-quality studies are needed to further evaluate the effects of empowerment education intervention on the self-efficacy, depression, and laboratory indicators of hemodialysis patients.
Limitations
This study only searched publicly published Chinese and English literature. The lack of systematic search of literature in less frequently used languages may cause a certain bias in the results. Some indicators have heterogeneity due to different assessment tools and cannot extract data for meta-analysis; thus, these limited the scale of meta-analysis. In addition, the random sequence generation and allocation concealment of multiple studies have not been specif i cally described and may have a certain impact on the reliability of the results.
Ethics approval
Not declared.
Conf l ict of interest
The authors declare that they have no conf l icts of interest.
- Frontiers of Nursing的其它文章
- Inf l uence of physical self and mindfulness on the academic possible selves of freshman nursing students
- Research status and hotspots of economic evaluation in nursing by co-word clustering analysis
- Analysis of the application and practice of PDCA cycle in management of the naked medicine dispensing—the quality and safety of the drug
- Investigation and analysis of attitudes and knowledge of aging among students in different majors
- Effectiveness of integrated nursing interventions for fatigue in patients with advanced cancer: a systematic review of randomized controlled trials
- The eligibility criteria, training content, and scope of practice for prescriptive authority for midwives: a modif i ed Delphi study†