
Dynamic knee valgus kinematics and their relationship to pain in women with patellofemoral pain compared to women with chronic hip joint pain
2019-09-25 07:51:54EricSchmidtMarcieHarrisHayesGretchenSalsich
Eric Schmidt,Marcie Harris-Hayes,Gretchen B.Salsich*
a Program in Physical Therapy,Washington University School of Medicine,St.Louis,MO 63108,USA
b Program in Physical Therapy,Department of Physical Therapy and Athletic Training,Saint Louis University,St.Louis,MO 63104,USA
c Department of Orthopaedic Surgery,Washington University School of Medicine,St.Louis,MO 63108,USA
Abstract Background:Dynamic knee valgus(DKV)is an abnormal movement pattern visually characterized by excessive medial movement of the lower extremity during weight bearing.Differences in hip and knee kinematic components of DKV may explain the emergence of different pain problems in people who exhibit the same observed movement impairment. Using a secondary analysis of exiting data sets, we sought to determine whether hip and knee frontal and transverse plane angles during a functional task differed between women with patellofemoral pain and women with chronic hip joint pain and the relationship between joint-specific kinematics and pain in these 2 pain populations.Methods:In the original studies,3-dimensional hip and knee kinematics during a single-limb squat were obtained in 20 women with patellofemoral pain and 14 women with chronic hip joint pain who demonstrated visually classified DKV.Pain intensity during the squat was assessed in both groups.For the secondary analysis,kinematic data were compared between pain groups using their respective control groups as a reference.Within each pain group,correlation coefficients were used to determine the relationship between kinematics and pain during the squat.Results:Hip adduction and contralateral pelvic drop were greater in those with chronic hip joint pain compared to those with patellofemoral pain(effect sizes ≥0.40). Greater knee external rotation(r=0.47,p=0.04) was correlated with greater knee pain in those with patellofemoral pain,while greater hip adduction(r=0.53,p=0.05)and greater hip internal rotation(r=0.55,p=0.04)were correlated with greater hip pain in those with chronic hip joint pain.Conclusion:Hip frontal plane motion was greater in those with chronic hip joint pain compared to those with patellofemoral pain.In both groups,greater abnormal movement at the respective joint(e.g.,knee external rotation in the patellofemoral pain group and hip adduction and internal rotation in the chronic hip joint pain group)was associated with greater pain at that joint during a single-limb squat.2095-2546/© 2019 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Anterior knee pain syndrome;Femoroacetabular impingement;Hip joint;Kinematics;Knee joint;Single-limb squat
1. Introduction
One in 4 people over the age of 18 report chronic joint pain.1This condition can lead to significant functional limitation2and economic burden.2Two prevalent sources of chronic joint pain are patellofemoral pain and chronic hip joint pain.Patellofemoral pain is pain located at the patellofemoral articulation and is characterized by retropatellar or peripatellar pain with activities involving lower limb loading.3Chronic hip joint pain4presents as deep hip joint or groin pain often associated with the diagnoses of femoroacetabular impingement,4structural instability,4acetabular labral tears,5and chondral lesions.6The best treatment approach for patellofemoral pain and chronic hip joint pain remains elusive. A better understanding of the factors associated with these pain conditions is needed to optimize future treatment strategies.
Abnormal movement patterns demonstrated during functional tasks is one factor that may contribute to chronic musculoskeletal pain.7,8Dynamic knee valgus(DKV)is an abnormal lower extremity movement pattern visually characterized by excessive medial movement of the lower extremity during weight bearing activity (Fig. 1). This excessive medial lower extremity movement is a multi-joint, multiplane pattern comprised of varying degrees of increased 3-dimensional (3D)joint kinematics that include hip adduction and internal rotation,and knee abduction and external rotation.9
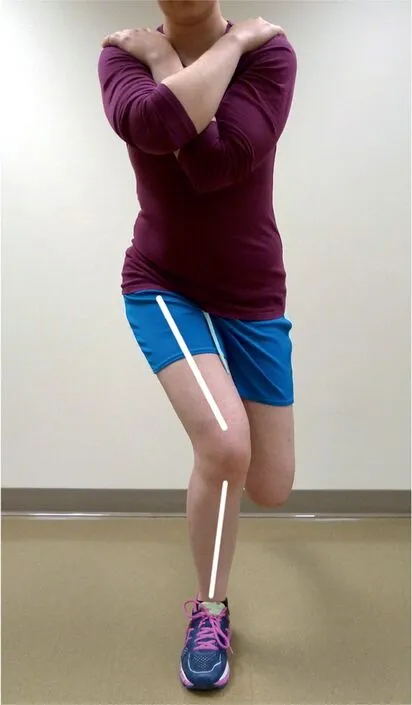
Fig.1. Dynamic knee valgus: excessive medial movement of the lower extremity as evidenced by an apparent increased frontal plane knee angle.
The increased motion of DKV may cause excessive stresses at the knee or hip joint and over time lead to patellofemoral pain or chronic hip joint pain. For example, increases in hip adduction, hip internal rotation, and knee external rotation may increase the dynamic quadriceps angle,9thereby increasing laterally directed stresses10on the patella and peripatellar tissues implicated in patellofemoral pain. Similarly, exaggerated hip adduction and internal rotation may increase hip joint stresses by increasing the abutment of the femur, pelvis, and intra articular structures on one another.11Over time, these excessive stresses may lead to chronic hip joint pain.11
Altered hip and knee kinematics associated with DKV have been reported in women with patellofemoral pain,12-16and although less studied, altered hip kinematics have been observed in women with chronic hip joint pain,7,17which suggests that women with DKV may represent a phenotype of patients among those who have patellofemoral or hip joint pain. Despite appearing to have the same visual movement impairment, however, those with patellofemoral pain may demonstrate different 3D kinematic components (e.g.,hip adduction, hip internal rotation, knee abduction, and knee external rotation) of DKV compared to those with chronic hip joint pain. This kinematic variation may create relatively greater stresses in either the knee or hip joints and may help explain why one population develops knee pain,and the other hip pain, despite a very similar looking abnormal movement pattern.
We were interested in determining whether subgroups of women with observed DKV (patellofemoral pain and chronic hip joint pain) differ in the 3D kinematic components of DKV and whether there is a relationship between joint-specific movement and pain experienced during a functional task.As an initial exploration of these questions,we performed a secondary analysis of existing data sets. We hypothesized that women with patellofemoral pain would have greater knee abduction and relative knee external rotation, and less hip adduction and hip internal rotation, during a single-limb squat compared to women with chronic hip joint pain. Secondly, based on our previously published work demonstrating relationships between patellofemoral pain and knee kinematics, but not hip kinematics,18we hypothesized that greater hip adduction and internal rotation would be associated with greater hip pain in the people with chronic hip joint pain, whereas knee kinematics and pain would not be related in this group. Determining the joint-specific kinematic differences and the relationships between joint-specific movement and pain is important as it may help clinicians develop more targeted movement based treatments to address the specific movement impairments that may be contributing to their patients'patellofemoral pain or chronic hip joint pain.
2. Methods
2.1. Experimental design
Kinematic, pain, and participant characteristic data were originally captured as part of 2 independent cross-sectional studies,conducted in separate laboratories.The first study analyzed the kinematics of those with patellofemoral pain,18and the second study analyzed those with chronic hip joint pain.19The original studies were approved by the Institutional Review Board at Saint Louis University and the Human Research Protection Office at Washington University. Before participation in the original studies,all participants signed an informed consent statement.All rights of the participants were protected.
2.2. Participants
2.2.1. Recruitment
Participants in the pain groups from the original studies were all women between 18 and 40 years of age, who had at least a 3 out of 10 average pain level over the past week and whose symptoms were at least 2 months in duration. Participants from the patellofemoral pain group were recruited between the years of 2009 and 2011 from the Saint Louis metropolitan area; from the campuses of Saint Louis University and Washington University; through word of mouth referrals from physician contacts and physical therapist colleagues;and through flyers posted in the surrounding community. Participants from the chronic hip joint pain group were recruited between the years of 2011 and 2013 from the Washington University orthopedic, physical medicine and rehabilitation, and physical therapy clinics; Washington University's research volunteer database;and public announcements.
Both laboratories also recruited control participants(women between 18 and 40 years of age) over the same time periods using word of mouth referrals and flyers posted in the community.For the purposes of the current analysis,data from the control groups were included to provide a reference for comparing kinematics between the pain groups whose data were collected in different laboratories.
2.2.2. Inclusion criteria
The symptoms in the patellofemoral pain group(pain located behind or around the patella)had to be elicited by at least 2 of 3 provocation tests (resisted isometric knee extension, step down,and single-limb squat).18The symptoms in the chronic hip joint pain group(deep joint or anterior hip pain)had to be elicited by the hip flexion, adduction, and internal rotation test.20To be included in this analysis,participants in both pain groups also had to demonstrate an observable DKV during a single-limb squat test. Observable DKV was defined as a≥10° frontal plane knee angle increase, as determined by visual observation, during the descent phase of the majority of the observed squat trials. This visual classification has been demonstrated to have a high level of agreement with a 2-dimensional knee frontal plane projection angle obtained during a single-limb squat.21The 20 patellofemoral pain participants from the original study met this criterion and were included in this analysis. Only 4 of the 31 screened potential participants (13%) who met the pain criteria were excluded because they did not have DKV.Seven additional participants were excluded for other reasons.Women with patellofemoral pain and DKV were similar to those without DKV(noDKV)with respect to age(DKV vs.noDKV:22.4±4.3 years vs.23.3±2.4 years),body mass(62.5±7.6 kg vs.63.5±8.8kg),height (167.2±6.5 cm vs. 165.1±4.8cm), and average pain in the past week (4.0±1.3 vs. 3.7±1.4). From the original chronic hip joint pain study, 16 of 30 (53%) were excluded from the current analysis because they did not meet the DKV criterion. As such, the 14 remaining chronic hip joint pain participants were included in the current analysis.Women with chronic hip joint pain and DKV were similar to those without DKV with respect to age(DKV vs.noDKV:27.2±5.3 years vs.25.6±4.5 years), body mass (66.4±11.9 kg vs. 65.1±7.8kg), height(166.9±8.0 cm vs.167.6±5.1cm),and average pain in the past week(3.9±2.2 vs.3.6±1.7).
For the patellofemoral pain study,DKV was determined by the principal investigator,a physical therapist with 24 years of experience,who observed the patient performing the squats in real time.For the chronic hip joint pain study,DKV was determined by the principal investigator, a physical therapist with 16 years of experience, who observed video recordings of the squat trials.While the video recordings could be viewed multiple times,they were played at normal speed and the same criteria were used to determine DKV as in the patellofemoral pain study.In addition,the 2 principal investigators have demonstrated excellent agreement with each other in their visual classification of DKV.21
The inclusion criterion for the control participants was pain-free status of the knee joint (knee control) or hip joint(hip control).
2.2.3. Exclusion criteria
Participants in all groups were excluded if their body mass index was greater than 30kg/m2, or had a neurologic involvement that would influence coordination or balance during movement testing. Participants in the patellofemoral pain group were excluded if they had a history (or current report) of knee ligament, tendon, or cartilage injury; traumatic patellar dislocation;patellar instability; prior knee surgery; or hip or ankle pain that limited their mobility. Participants in the chronic hip joint pain group were excluded if they had a history of hip fracture or hip surgery or knee or low back pain that limited their mobility.
Control participants were excluded if they had current or prior history of patellofemoral pain (knee control) or hip joint pain(hip control).An additional exclusion criterion of the original patellofemoral pain study was the presence of observable DKV. Of the 52 potential knee control participants who were screened and met all other criteria, 29 (56%) were excluded because they demonstrated DKV. Three additional participants did not complete the study procedures, yielding 20 knee control participants for the current analysis. To provide a similar comparison group, the hip control participants were excluded from the current analysis if they demonstrated observable DKV.From the original chronic hip joint pain study, 17 of 30 (57%)participants were excluded because they demonstrated DKV,yielding 13 control participants for the current analysis.
2.3. Data collection and processing
2.3.1. Motion capture procedures
Three-dimensional (3D) kinematic data were collected in the original studies using an 8-camera, 3D motion analysis system(Vicon;OMG plc,Oxford,UK)sampling at 120Hz.The patellofemoral pain participants wore running shoes during data collection, while the chronic hip joint pain participants were barefoot.Prior to the collection of the squat trials,a static standing trial,during which participants were instructed to stand facing straight ahead with feet hip width apart,was performed in order to build the skeletal model and align the segment coordinate axes.
Participants performed trials of a single-limb squat as follows.From a standing position,participants were instructed to shift their bodyweight onto their involved limb and flex their uninvolved knee, positioning their foot behind them. Next,they were instructed to squat as deep as they could go while still maintaining balance and then return to an upright stance.A full squat cycle was defined as the start of knee flexion, to full knee extension. Three trials in which subjects squatted to at least 60°of knee flexion(visually estimated)and returned to standing without losing their balance were recorded.
2.3.2. Pain assessment
Pain during the squat task for the patellofemoral pain group was assessed using a 100-mm visual analog scale,22with 0=no pain and 100=worst pain possible; and for the chronic hip joint group, using a verbal numeric pain rating scale,22with 0=no pain and 10=worst pain possible. The patellofemoral pain participants were asked to mark a point on a 100-mm line that corresponded to the average pain during the squat trials, whereas the chronic hip joint pain participants verbally rated their perceived pain after each trial, and the average of the pain measurements was computed.
2.3.3. Kinematic analysis
For the purposes of the current analysis,the kinematic data from both laboratories were re-processed using the same kinematic model and marker set to allow kinematic comparisons between groups. Body segments and coordinate axes were defined as in the original patellofemoral pain study18with the exception of the pelvis segment(described below).Using Visual3D software(C-Motion,Inc.,Germantown,MD,USA),the marker trajectories were low-pass filtered using a fourth order Butterworth filter with a 6-Hz cutoff frequency.A 6 degrees of freedom model incorporated the pelvis, thigh, and shank. For the pelvis, the Codamotion model (Charnwood Dynamics Ltd., Leicestershire, UK) was used. The frontal plane for the thigh was defined by the hip joint center23and the 2 femoral epicondyle markers. The frontal plane for the shank was defined by the 2 femoral epicondyle markers and the midpoint of the malleolus markers. For each segment, the local coordinate system was located at the proximal endpoint. The frontal plane was defined by the orientation of the x axis(flexion and extension). The z axis (internal and external rotation) passed through each segment's proximal and distal end points. The y axis (abduction and adduction) was oriented orthogonal to both the x axis and z axis.
Three-dimensional hip and knee joint angles were calculated and expressed in the reference frame of the proximal segment. To determine the pelvis contribution to the hip adduction angle, the pelvis frontal plane angle was calculated relative to the laboratory coordinate system. Positive values represented hip and knee flexion, adduction, internal rotation,and contralateral pelvic drop. The Cardan sequence of rotations was x,y,z for all joint and segment angles except the pelvis,which was z,y,x.24For each trial,hip and knee frontal and transverse plane angles and pelvis frontal plane angle were obtained at the time of peak knee flexion. The time of peak knee flexion was chosen as it was consistent with time of peak knee extensor moment, a point of peak patellofemoral joint stress,25and because it closely corresponded to peak hip flexion. Peak hip flexion may represent maximal stresses in the hip,as hip flexion,combined with internal rotation and adduction, will maximize the chances of femoral acetabular abutment.11Angles were averaged over 3 trials. Test-retest reliability of the kinematic measures, obtained at least 2 days apart,26was determined previously in both laboratories. Intraclass correlation coefficients ICC (3, 3) ranged from 0.54 to 0.87 and standard errors of measurement ranged from 1.59°to 3.54°(Supplementary Table 1).
2.3.4. Additional subject characterization
Self-reported measures of pain and activity level were obtained in the original studies and are reported in the current analysis to characterize the samples.Average pain severity the week prior to the study was collected using an 11-point numerical scale (0 representing no pain and 10 representing severe pain), for both the patellofemoral pain and chronic hip joint pain groups.In addition,participants reported duration of pain in months. Activity level was collected using the Baecke Habitual Activity Questionnaire.
2.3.5. Statistical methods
Independent t tests were used to compare participant characteristics between the patellofemoral pain group and the chronic hip joint pain group. Due to methodological differences between laboratories and the exploratory nature of this analysis, effect sizes27rather than p values were computed to compare kinematics between groups. Effect sizes of 0.40 and above were considered moderate effects. Within each laboratory, effect sizes were generated for between-group(pain-control) differences. Across laboratories, the differences of the between-group (within laboratory) differences were calculated.The relationships between hip joint,knee joint,and pelvis segment angles and pain during the single-limb squat were determined within each group using Pearson correlation coefficients for the patellofemoral pain group (interval data)and Spearman correlation coefficients for the chronic hip joint pain group(ordinal data).Data were analyzed using SPSS Version 22.0 (IBM Corp., Armonk, NY, USA) with the threshold for significance set at p ≤0.05.
3. Results
With the exception of age,participants with patellofemoral pain and those with chronic hip joint pain were similar with respect to height,weight,activity level,average pain intensity in the past week, and pain duration (Table 1). Kinematic values are displayed in Table 2. Both the patellofemoral pain group and the chronic hip joint pain group had greater relative knee external rotation (less knee internal rotation) and greater hip internal rotation compared to their control groups (effect sizes ≥0.40).Both pain groups also had greater hip adduction and contralateral pelvic drop compared to their control groups,however the hip group differences were greater than the knee group differences(effect sizes ≥0.40).Hip flexion was less in the chronic hip joint pain group compared to hip control group(effect size = 0.42). Effect sizes for all other kinematic comparisons were below 0.40.
For those with patellofemoral pain, reprocessing the data with the newly defined pelvic segment did not change the previously published relationships.18Greater knee external rotation was associated with greater knee pain during the singlelimb squat (Table 3). For those with chronic hip joint pain,greater hip adduction and hip internal rotation were associated with greater hip pain during the single-limb squat.In addition,in those with patellofemoral pain, hip angles were not associated with knee pain. Similarly, in those with chronic hip joint pain,knee angles were not associated with hip pain(Table 3).
4. Discussion
To better understand the relationship between joint-specific movement impairments and pain we performed a secondaryanalysis of data collected from 2 different musculoskeletal pain populations whose members demonstrated the same visually classified abnormal movement pattern (DKV). We compared hip, knee, and pelvis kinematics between the patellofemoral pain group and the chronic hip joint pain group using their respective control groups as a reference to account for methodological differences between laboratories. Inaddition, within each pain group we determined the correlations between hip and knee joint angles and pelvis segment angles and joint pain during a single-limb squat.
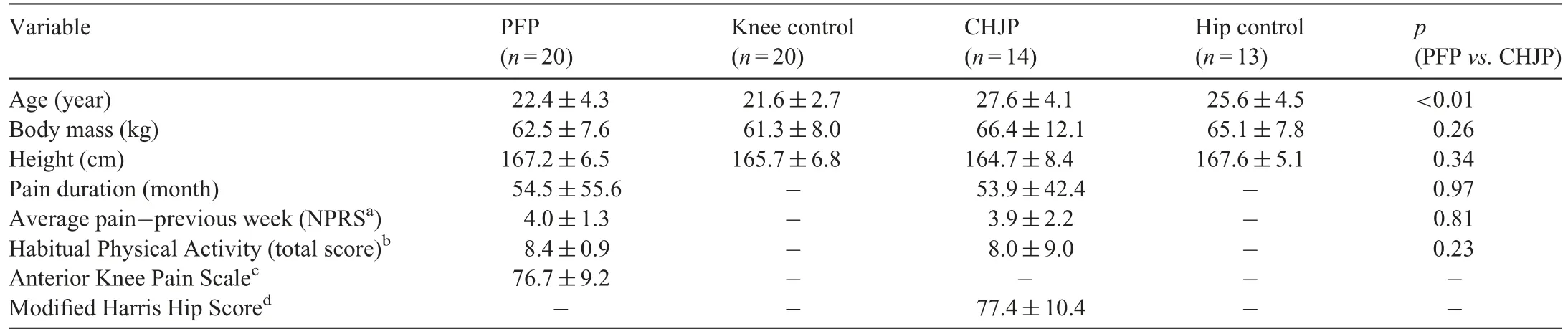
Table 1 Participant characteristics(mean±SD).
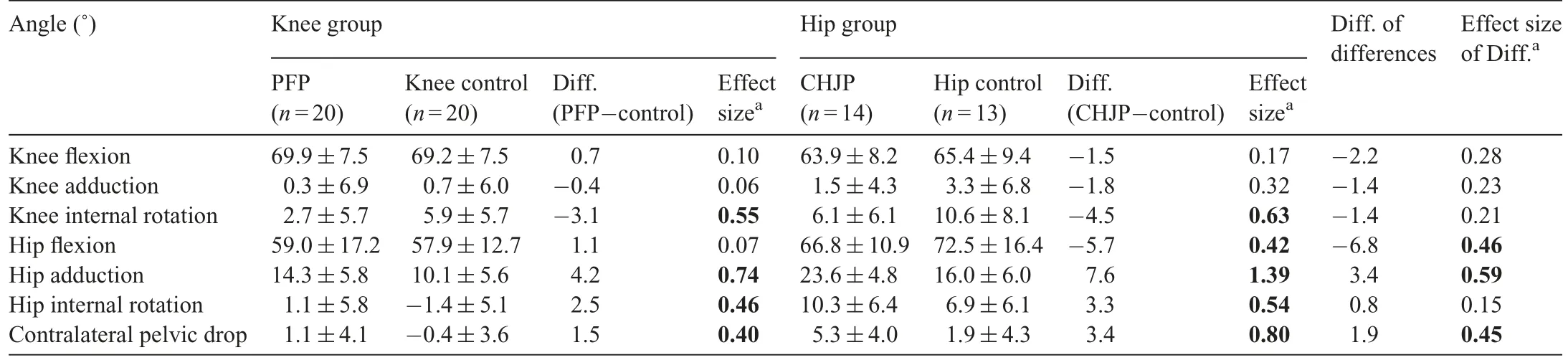
Table 2 Three-dimensional joint angles at peak knee flexion during single-limb squat(mean±SD).
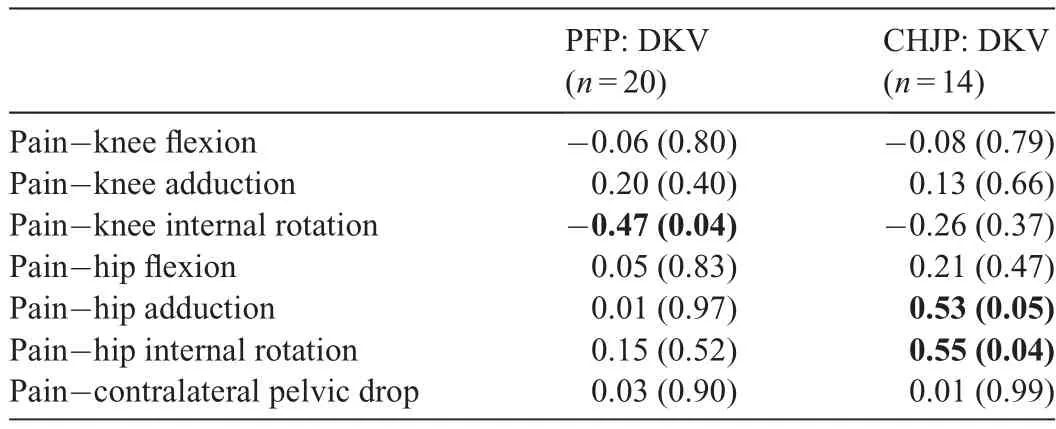
Table3 Correlation between knee and hip kinematics at peak knee flexion and pain during the single-limb squat.
As hypothesized, participants in the patellofemoral pain group had greater relative external knee rotation compared to the chronic hip joint pain group; however, this difference appears to be explained by methodological differences across studies, as the within-laboratory differences (pain vs. control group) were very similar in the 2 laboratories. Nonetheless,greater knee external rotation was associated with greater knee pain in the people with patellofemoral pain,as noted in the original study,18and not associated with greater hip pain in the people with chronic hip joint pain, which lends support for the mechanism of excessive external rotation contributing to a patellofemoral pain problem.This finding builds on those of previous studies that have reported greater relative knee external rotation in those with patellofemoral pain compared to healthy controls during single-limb squats,15,28single-limb jumps,15and running,15by substantiating a mechanical link between knee external rotation and pain during a movement task.
Contrary to our hypothesis,knee abduction was not greater in the patellofemoral pain group compared to the chronic hip joint pain group. In addition, knee abduction angles were similar between the patellofemoral pain group and the knee control group, which suggests that the 3D frontal plane knee angle is not a major component of the overall dynamic valgus movement pattern during a single-limb squat29and may not be a major contributor to patellofemoral joint pain. That said, increased knee abduction moments (i.e., loading), which may occur in the absence of increased knee abduction angles, have been associated with the development of patellofemoral pain.30
Consistent with our hypothesis, participants with chronic hip joint pain demonstrated greater hip adduction compared to those with patellofemoral pain,which suggests that hip frontal plane motion had a greater contribution to DKV in this population than in the women with patellofemoral pain. They also had greater contralateral pelvic drop, which suggests that in participants with chronic hip joint pain, increased pelvis motion was a key contributor to increased hip adduction.Importantly,the hip and pelvis kinematic differences between groups were detected irrespective of the methodological differences between laboratories. Regarding the kinematic and pain relationships, we found a positive correlation between hip adduction and internal rotation and hip pain during a singlelimb squat. We hypothesized this relationship would exist as the combined motion of increased hip adduction and internal rotation, which has been shown to lead to greater bony abutment of the femur against the acetabulum.11This increased bony abutment is proposed to lead to chronic hip joint pain and its associated conditions, including femoroacetabular impingement,11labral tears,31and chondral lesions.11
Our findings in the chronic hip joint pain group are in line with other movement analysis studies that have analyzed lower extremity kinematics in those with chronic hip joint pain.Kumar et al.17found relatively greater hip adduction during maximal squat depths in those with femoroacetabular impingement compared to healthy controls.Similarly,Kennedy et al.32found that during gait,compared to controls,those with femoroacetabular impingement were in a relatively more adducted position just after toe off.In contrast,other studies have found no difference in hip adduction17or have found decreased hip adduction33during functional tasks in those with chronic hip joint pain.It may be that this reduced hip movement is a strategy to decrease hip pain.
While we observed greater hip internal rotation in the hip pain group compared to the patellofemoral pain group,the difference appears to be explained by methodological differences across studies, as the within-laboratory differences (pain vs.control group) were very similar in the 2 laboratories. Nonetheless, we found a direct relationship between increased hip internal rotation and hip pain during a single-limb squat, a finding that is in line with Austin et al.,7who found a relationship between hip internal rotation and chronic hip joint pain in a subject with an acetabular labral tear and anterior medial groin pain during running, drop jump, and step down tasks.Austin et al.7demonstrated that reducing hip internal rotation and adduction with the use of a lower extremity brace in this subject reduced the subject's anterior medial groin pain in each task.Combined,our study and the study of Austin et al.7suggest that excessive hip internal rotation may be associated with increased pain in those with chronic hip joint pain.
Although not part of our purpose, we analyzed sagittal plane hip and knee angles to get a more complete picture of the movement patterns used by the 2 pain groups during the single-limb squat. Knee flexion was similar in both pain groups and between the pain and control groups within each laboratory. However, the chronic hip joint pain group had greater hip flexion than the patellofemoral pain group but less hip flexion than the hip control group. While methodological differences across laboratories could explain the hip flexion differences between the pain groups,given the similar hip flexion values between the patellofemoral pain group and the knee control group,the finding of less hip flexion in the chronic hip joint pain group compared to the hip control group suggests that participants with chronic hip joint pain may have been reducing hip motion in the sagittal plane to compensate for increased motion in the frontal and transverse planes.
Collectively, our data suggest that people with patellofemoral pain and chronic hip joint pain,who also demonstrate a visually classified DKV, may use different joint-specific movement strategies to complete a single-limb squat task,even when given similar instruction.In addition,in both populations, greater movement impairments at the respective joint may contribute to the intensity of pain experienced at that joint during a functional task.These results provide insight into possible pain mechanisms and could help direct clinical examination tests and rehabilitation interventions in these 2 pain populations. For example, in people with patellofemoral pain,reducing relative knee external rotation(via distal or proximal movement training or muscle strengthening approaches)might be an effective target for rehabilitation,whereas in people with chronic hip joint pain,targeting optimal pelvis,and hip motion during functional tasks might be indicated.
There were several limitations in our study. Because this secondary analysis was not initially planned during the development of the 2 original studies, some procedures were not standardized across the laboratories.Mainly,those in the patellofemoral pain group wore shoes during the movement capture trials, which may have systematically influenced the kinematics. However, if footwear were the primary contributor to the kinematic differences, we would have expected the patellofemoral pain group to have demonstrated less relative knee external rotation compared to the chronic hip joint pain group,which was not the case. Despite the difference in footwear,many other methods were consistent across the 2 laboratories.For instance, we used the same marker placement, squatting instructions, and kinematic processing procedures in the 2 studies.Additionally,the reliability for the hip and pelvis kinematic variables in the patellofemoral pain group was moderate.While we were able to detect a fairly large within-laboratory difference in hip adduction that was greater than the standard error of the measure, the within-laboratory differences for hip internal rotation and contralateral pelvic drop were less than the standard error of the measure, and thus should be interpreted with caution.It should also be noted that the kinematic differences we detected between painful groups and controls were influenced by our pre-defined inclusion and exclusion criteria for observed movement patterns.Finally,the associations we detected were correlational in nature,and as such,we cannot establish a causal relationship between kinematics and pain. To help establish mechanisms of musculoskeletal pain,future research should prospectively investigate the contribution of joint specific movement to pain across a variety of musculoskeletal pain conditions. Better understanding of these relationships may help clinicians develop more specific movement based treatments to address the specific movement impairments which may be contributing to their patients'patellofemoral pain or chronic hip joint pain.
5. Conclusion
In women who demonstrate visually classified DKV, hip adduction and contralateral pelvic drop were greater in those with chronic hip joint pain compared to those with patellofemoral pain.In both groups,greater abnormal movement at the respective joint (e.g., knee external rotation in the patellofemoral pain group and hip adduction and internal rotation in the chronic hip joint pain group)was associated with greater pain at that joint during a single-limb squat.
Acknowledgments
The authors would like to thank Randy Richter for his input on statistical analysis procedures. This work was supported by the Washington University Institute of Clinical and Translational Sciences (No. UL1 TR000448) (Schmidt); from the National Center for Advancing Translational Sciences (No. TL1 TR000449) (Schmidt); from the National Center for Medical Rehabilitation Research, National Institute of Child Health and Human Development, and National Institute of Neurological Disorders and Stroke (No. K23 HD067343, K12 HD055931)(Harris-Hayes);and from the National Center for Medical Rehabilitation Research, National Institute of Child Health and Human Development (No. R15HD059080) (Salsich). The funding organizations had no role in the collection of data,their analysis and interpretation, or in the right to approve or disapprove publication of the finished manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Authors'contributions
ES carried out secondary kinematic data processing and analysis of the previously collected samples to ensure uniformity of data as well as the statistical analysis to compare groups,drafted the manuscript;MHH was responsible for all aspects of the original chronic hip joint pain study, which included study design,participant recruitment, data collection, analysis, and dissemination;GBS was responsible for all aspects of the original patellofemoral pain study, including study design, participant recruitment, data collection, analysis and dissemination; both MHH and GBS assisted and mentored ES in all steps of the secondary analysis and manuscript development as part of 1 yearlong pre-doctoral clinical research training program. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary data to this article can be found online at doi:10.1016/j.jshs.2017.08.001.
 Journal of Sport and Health Science2019年5期
Journal of Sport and Health Science2019年5期
- Journal of Sport and Health Science的其它文章
- Biomechanics of ankle giving way:A case report of accidental ankle giving way during the drop landing test
- Influences of load carriage and physical activity history on tibia bone strain
- Effects of intermittent sprint and plyometric training on endurance running performance
- The relationship between transport-to-school habits and physical activity in a sample of New Zealand adolescents
- Cardiorespiratory fitness and cancer in women:A prospective pilot study
- Heat dissipating upper body compression garment:Thermoregulatory,cardiovascular,and perceptual responses