
Curcumin in The Treatment of in Animals Myocardial ischemia reperfusion: A Systematic review and Meta-analysis
2019-07-16 04:36:08QianHeBinMengHongYunHuGaoJianZhuangQunTangXuZhu
Medical Data Mining 2019年2期
关键词:姜黄
Qian He, Bin Meng, Hong-Yun Hu, Gao-Jian Zhuang, Qun Tang, Xu Zhu*
Hunan University of Chinese Medicine, Changsha, 410208, China.
Abstract Objective:The protective effects of curcumin on myocardial ischemia-reperfusion were systematically evaluated by analyzing the related literatures of curcumin and myocardial ischemia-reperfusion.Methods:The computer was searched for Wanfang, VIP, China National Knowledge Infrastructure(CNKI), SinoMed, and Pubmed database to find animal experiments on curcumin treatment of myocardial ischemia-reperfusion.The retrieval time is from the establishment of the database to November 2018. Two researchers independently screened the literature based on inclusion and exclusion criteria, extracted the data, and assessed the risk of bias in the included studies. Meta analysis was performed using RevMan 5.3 software.Results:Finally, 9 studies were included for analysis. Meta-analysis showed that the curcumin group can reduce LD and MDA levels compared with the ischemiarreperfusion group (LD: SMD=-4.75, 95% CI [-6.56, -2.94], P < 0.01, MDA: SMD=-2.27, 95% CI[-3.07, -1.47], P < 0.01), the difference was statistically significant (P<0.01). In the subgroup analysis of different doses of curcumin, different doses of curcumin (0.8, 10, 12.5, 20, 25,30, 50 mg) were able to reduce LD content compared with the ischemia-reperfusion group, and the differences were statistically significant. Different doses of curcumin(5,10,20,30,40mg) can reduce MDA content, and the difference is statistically significant;curcumin (0.8mg) group has no statistically significant effect on MDA content (SMD = -0.54,95% CI [-1.35, 0.28], P = 0.20). The relationship between the content of MDA and the dose of curcumin showed that compared with the curcumin (20 mg) group, the curcumin (40 mg)group could better reduce the MDA content, and the difference was statistically significant(P=0.03).Conclusion:Curcumin can reduce the content of LD and MDA in myocardial ischemia-reperfusion, and has a protective effect on myocardium. Moreover, the ability to reduce the damage is related to the dose of curcumin. owever, the sample of the included studies is limited, and this conclusion requires more high-quality experiments to verify.
Keywords:curcumin; myocardial ischemia-reperfusion; meta-analysis; animal experiment;systematic review
Background
In recent years, with the increase of cardiovascular diseases, especially coronary heart disease, it has seriously endangered human health. Coronary artery occlusion is prone to lead to ischemia and myocardial infarction. The recovery of ischemic myocardium after perfusion causes further damage to the morphology,function and metabolism of myocardial cells, which is called myocardial ischemia-reperfusion injury. In myocardial ischemia-reperfusion injury, ischemia and hypoxia produce a large number of oxygen free radicals, which can further aggravate tissue damage and eventually lead to irreversible damage to cardiac myocytes[1]. At present, the drug studies to prevent the injury caused by myocardial ischemiareperfusion mainly play a role in reducing the oxidative damage of myocardial cells and calcium overload of myocardial cells. Curcumin is a yellow phenolic compound extracted from Curcuma tuber, which has anti-inflammatory, anti-oxidative and anti-apoptotic effects. The anti-oxidative effect is mainly related to scavenging oxygen free radicals and increasing oxidase activity, and has a good protective effect on cells[2].At present, there are some basic researches, but there is still a lack of systematic evaluation. In this paper,we systematically evaluated the experimental study of curcumin on myocardial ischemia-reperfusion by using Meta-analysis method, and provided references and suggestions for optimizing animal experimental design and improving research quality.
1 Materials and methods
1.1 Inclusion and exclusion criteria
1.1.1 Research Types Randomized controlled animal experiment
1.1.2 Research object
Rats, not limited in strain, not limited in male and female
1.1.3 Interventions
Intervention with different doses of Curcumin.(Curcumin group)Mainly ischemia-reperfusion group. (Model group)
1.1.4 Outcome Indicators
The main outcome indicators were serum malondialdehyde (MDA) and lactate dehydrogenase(LDH).
1.1.5 Exclusion criteria
(1) Non-rat model of myocardial ischemia-reperfusion injury in the literature; (2) rat isolated heart reperfusion model; (3) duplicated papers and conference papers;(4) intervention measures of curcumin post-treatment;(5) review.
1.2 Retrieval Strategy
We searched Wanfang, VIP, CNKI, SinoMed and Pubmed by computer, and collected animal experiments on curcumin for myocardial ischemia and reperfusion.The retrieval time is from the establishment of the database to November 2018. Chinese search terms:姜黄素、心肌缺血再灌注;English search words: curcumin, Myocardial ischemia reperfusion,Myocardial ischemia-reperfusion.
1.3 Literature screening and data extraction
Two researchers independently conducted literature screening and data extraction, conducted crosschecks, and consulted a third party for assistance in resolving differences. The basic characteristics of the study included: first author, year of publication, rat characteristics, modeling methods, groups and sample size, intervention measures, outcome indicators.
1.4 Quality Evaluation
According to the list of CAMARADES, the quality of the included studies was evaluated. There were 10 items: (1) Papers published after peer review; (2)instructions with temperature control; (3) randomly assigned to treatment group or control group; (4) blind method of researchers; (5) blind evaluation of results;(6) application of anesthetics without significant impact on outcome indicators; (7) animal model (myocardial ischemia-reperfusion model); (8) calculation of sample size; (9) compliance with animal protection laws and regulations; (10) Potential conflict of interest in the declaration.
Two researchers evaluate the quality of the literature separately, and then cross-examine the literature after the evaluation. If there are differences, consult a thirdparty researcher to resolve them..
1.5 Data extraction and merging
LDH and MDA data of curcumin group were merged according to formula [3] in literature, and the data with obvious errors were excluded. The formula assumes that there are m sub-groups, the sample size of sub-group I is ni, the mean value isthe standard deviation is SDi, the total mean value is XT, and the total standard deviation is SDT.

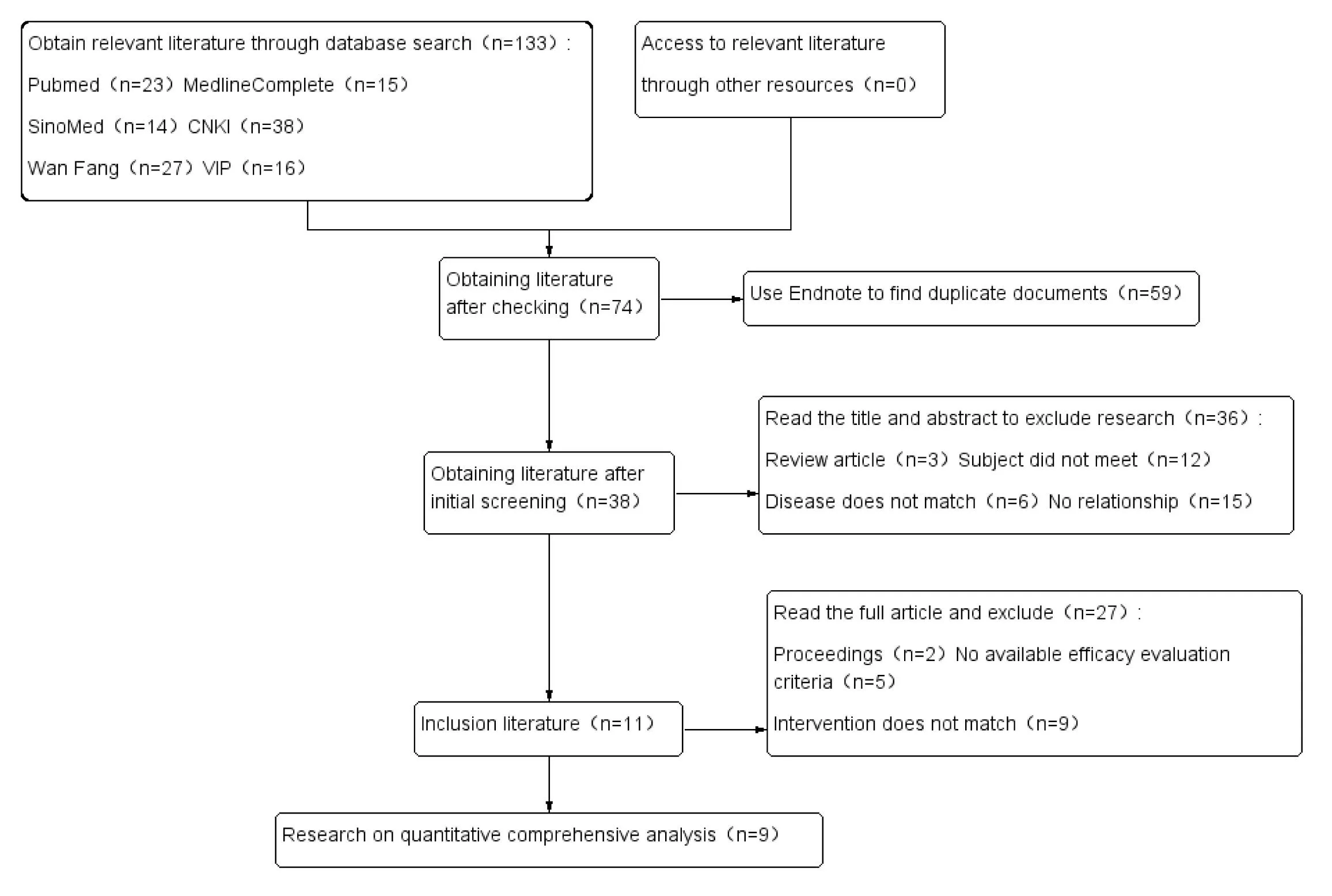
Figure 1. Literature screening process
1.6 Statistical methods
RevMan 5.3 software was used for meta-analysis.RevMan 5.3 statistical data were used. Mean difference(SMD) was used as the effect index, Cochrane Q test was used to analyze the heterogeneity among the studies, and I2was used to evaluate the heterogeneity. If I2> 50% indicates that there is obvious heterogeneity,the study can be subdivided according to curcumin dosage. When there is no significant heterogeneity, the results can be merged by fixed effect model, and the random effect model can be used instead.
2 Results
2.1 Literature screening process and results
133 studies were collected from different databases,59 duplicate articles were excluded, 36 articles were excluded from reading abstracts and titles, 27 articles were excluded from reading the full text, 11 articles met the criteria, and 9 studies were finally carried out quantitative analysis. The flow chart of literature screening is shown in Figure 1. Characteristic tables and quality scores included in the study are shown in Table 1.
2.2 Meta-analysis results
2.2.1 Content of LDH
LDH content was reported in seven studies[4-8, 10,12]. The data of LDH content in curcumin groups of different doses were combined and analyzed. Fixedeffect model showed that I2=94% between studies,because I2>50%, random-effect model was adopted.

Table 1. Features included in the experiment table

Figure 2. Meta-analysis forest map of LDH content in curcumin treatment group and ischemia-reperfusion
The results showed that curcumin could reduce LDH content, reduce myocardial injury and protect myocardium compared with model group, and the difference was statistically significant (SMD= -4.75, 95%CI [-6.56, -2.94], P<0.01). The analysis results were shown in Figure 2.
2.2.2 Analysis of the effect of curcumin treatment group on LDH content

Figure 3. LDH subgroup analysis of curcumin treatment group and model group
Seven studies [4-8, 10, 12] reported the content of LDH. Subgroup analysis was carried out according to different doses of curcumin. Fixed-effect model showed that I2was 95.7% between studies. Because I2was more than 50%, random-effect model was selected.The results showed that curcumin (10,20,40 mg) group could reduce the level of LDH, the difference was significant (SMD= -2.36, 95% CI [-4.01,-0.71], P <0.01; SMD= -9.42, 95% CI [-12.83,-6.00], P < 0.01;SMD= -7.81, 95% CI [-9.93,-5.70], P < 0.01); curcumin(12.5, 25, 50 mg) group could reduce the level of LDH,the difference was significant (SMD=-4.45, 95% CI[-6.22, -2.68], P < 0.01; SMD= -6.10, 95% CI [-8.38,-3.81], P < 0.01; SMD= -8.76, 95% CI [-11.91, -5.61],P < 0.01. In one study, compared with the ischemiareperfusion group, the randomized effect model Metaanalysis showed that curcumin (0.8mg) group could reduce the level of LDH (SMD=-1.21, 95% CI [-2.09,-0.32], P < 0.01). The results are shown in Figure 3.2.2.3 Content of MDA
Seven studies[4, 6, 8-12] reported MDA levels.Data from curcumin groups of different doses were combined and analyzed. Fixed-effect models showed that I2=84% between studies, because I2>50%, so random-effect models were used. The results showed that curcumin treatment group could reduce the content of MDA and the severity of tissue damage caused by oxygen free radicals compared with model group(SMD=-2.27, 95% CI [-3.07, -1.47], P < 0.01). The analysis results were shown in Figure 4.
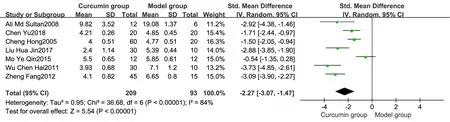
Figure 4. Meta-analysis forest map of MDA content in curcumin treatment group and ischemia-reperfusion
2.2.4 Analysis of the effect of curcumin treatment group on MDA content
Subgroup analysis was carried out according to different doses of curcumin. Fixed-effect model showed that I2=89.5% between studies, so randomeffect model was adopted. The results showed that curcumin (10,20,40 mg) group could reduce the level of MDA, with significant difference (SMD=-3.41, 95%CI [-5.23,-1.59], P < 0.01; SMD=-2.95, 95% CI [-4.19,-1.71], P < 0.01; SMD=-3.78, 95% CI [-5.84,-1.73],P < 0.01). Meta-analysis of randomized effect model showed that curcumin (0.8mg) group had no significant effect on MDA level (SMD=-0.54, 95% CI [-1.35,0.28], P=0.20). In one study, compared with the model group, the randomized effect model Meta-analysis showed that curcumin (5 mg) group could reduce the level of MDA, with significant difference (SMD=-4.85,95% CI [-7.47, -2.23], P < 0.01). A randomized effect model Meta-analysis showed that curcumin (30mg)group could reduce the level of MDA (SMD=-12.96,95% CI [-17.53, -8.39], P < 0.01). The analysis results were shown in Figure 5.
2.2.5 Relationship between curcumin and MDA content in different doses
Four studies [6, 8, 11, 12] reported the effects of 20 mg vs 10 mg on MDA, three studies [6, 8, 11]reported the effects of 40 mg vs 10 mg on MDA, and three studies[6, 8, 11] reported the effects of 40 mg vs 20mg on MDA (The analysis results were shown in Figure 6, Figure 7, Figure 8, The summary results are shown in Table 2). The results showed that compared with curcumin (10mg), curcumin (20mg) group had no significant difference in reducing MDA content(P=0.29), curcumin (40mg) group could better reduce MDA content (P=0.01), and curcumin (40mg) group could better reduce MDA content compared with curcumin (20mg) group, the difference was statistically significant (P=0.03).
2.2.6 Publication bias
According to the funnel diagram of the effect of curcumin treatment group and model group on LDH and MDA content, as shown in figure 9. The results show that the distribution of each study is asymmetric on both sides of the funnel map, indicating that there is publication bias.

Figure 5. Analysis of MDA subgroup in curcumin treatment group and model group
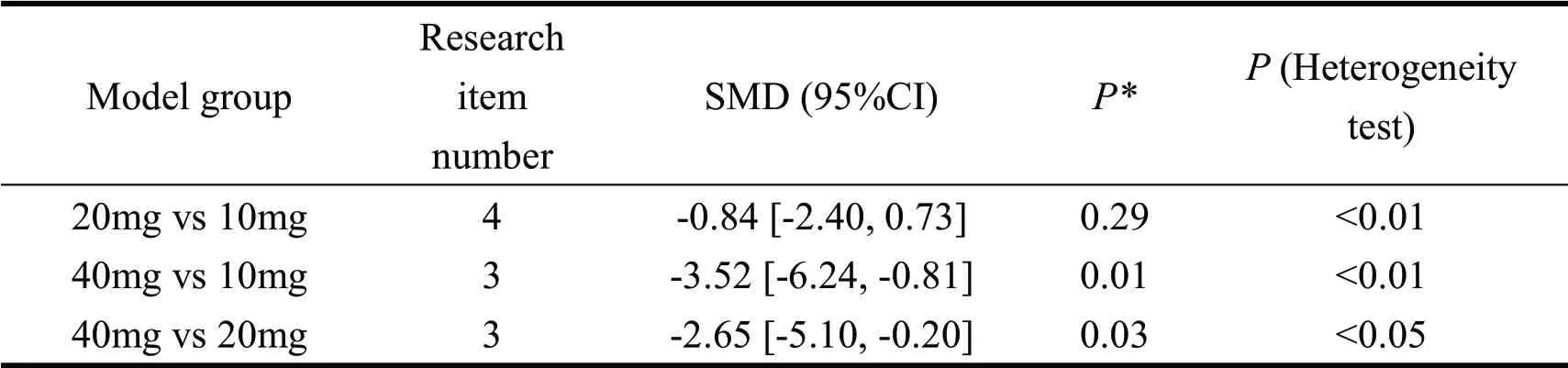
Table 2. Results of curcumin and MDA contents in different doses

Figure 6. Meta-analysis forest map of MDA content in 20 mg vs 10 mg group

Figure 7. Meta-analysis forest map of MDA content in 40 mg vs 20 mg group

Figure 8. Meta-analysis forest map of MDA content in 40 mg vs 10 mg group
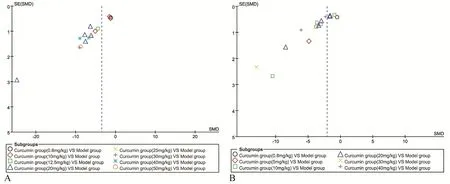
Figure 9. Funnel diagram for analysis of the effect of curcumin treatment group and model group (A: LDH B: MDA)
3 Discussion
In this paper, the protective effect of curcumin on myocardial ischemia-reperfusion was verified by systematic analysis of previous articles, so as to provide theoretical guidance for scientific prevention and treatment of myocardial ischemia-reperfusion caused by coronary heart disease. LDH, a marker of myocardial injury, is an indicator of the severity of myocardial injury [13]. MDA, a metabolite of lipid
peroxidation, can indirectly reflect the severity of tissue damage caused by oxygen free radicals. Therefore,according to the changes of LDH and MDA in serum,the therapeutic effect of curcumin on myocardial ischemia-reperfusion model can be judged. Sun Meng et al [14] found that curcumin may protect cardiac myocytes by promoting SIRT3 expression and antioxidative stress injury in the model of ischemiareperfusion injury of cardiac myocytes pretreated with curcumin.
From the forest plots of LDH and MDA in this paper, we can see that curcumin treatment group has certain effect on reducing myocardial injury. (LDH:SMD=-4.75, 95% CI [-6.56, -2.94], P < 0.01, MDA:SMD=-2.27, 95% CI [-3.07, -1.47], P < 0.01). This is consistent with the existing research results. The results of the relationship between curcumin and MDA content in different doses showed that with the increase of curcumin dosage, the more significant the effect of reducing myocardial injury was, and the effect of curcumin (40mg) group on reducing MDA content was better. In the process of literature collection and screening, it was found that all the included studies were published articles, which were reviewed by peers,but neither blind method nor sample size calculation was mentioned. Some studies lacked description of experimental conditions. Only three studies[5,6,9]described temperature control and random grouping completely. Quality assessment of the included studies based on the list of CAMARADES, the average score is 5.11, the highest score is 6, and the lowest score is 4. The overall quality of the included research is acceptable, but the lack of some experimental data may lead to errors in the comparison between the studies.Experimental researchers should standardize the grouping and allocation of experiments and describe them in detail in order to improve the quality of research reports[15].
The system evaluation still has some limitations:(1) This study mainly includes Chinese and English studies with a small number, lacking of effective grey literature, which may lead to bias by omitting negative results. If the negative results are not published, the study will be incomplete, and the combined effects will be overestimated. (2) There are differences in the establishment of animal models, and there is no uniform time for myocardial ischemia and reperfusion.(3) The results of random effects model processing may weaken the quality of evidence.
In conclusion, the available evidence shows that curcumin can reduce the levels of MDA and LDH in myocardial ischemia-reperfusion model, reduce the injury caused by myocardial ischemia-reperfusion,and has a certain relationship with the dose. With the further study on the pharmacological mechanism of curcumin, its efficacy will continue to improve.Influenced by the quantity and quality of the included studies, large sample studies with rigorous design and methods should be carried out to determine the efficacy and safety of curcumin therapy so as to better serve the clinic.
猜你喜欢
Digital Chinese Medicine(2022年2期)2022-07-02 07:46:20
九江学院学报(自然科学版)(2022年2期)2022-07-02 02:34:24
文萃报·周五版(2018年25期)2018-08-13 01:41:44
中成药(2018年2期)2018-05-09 07:19:43
中成药(2018年3期)2018-05-07 13:34:37
中国运动医学杂志(2016年3期)2016-07-10 12:07:23
中国塑料(2015年3期)2015-11-27 03:42:16
中国生化药物杂志(2015年4期)2015-07-07 12:05:59
西南军医(2015年1期)2015-01-22 09:08:25
中国神经精神疾病杂志(2014年1期)2014-03-01 03:23:23
- Medical Data Mining的其它文章
- Postulation of a Priod of an unexplored manuscript
—— Kashyapa Samhita - Efficacy of empowerment education in self-management with Type 2 Diabetes Mellitus: A systematic review and meta-analysis
- The application effect of swaddling bath in neonates: A meta-analysis
- Bibliometric Analysis of the Elderly’s Frailty in China