
Epidemiology and immunodiagnostics of Strongyloides stercoralis infections among migrant workers in Malaysia
2019-07-13 01:45:24NorhidayuSahiminYvonneLimRahmahNoordinMuhammadHafiznurYunusNorsyahidaArifinJerzyMarianBehnkeSitiNursheenaMohdZain
Norhidayu Sahimin, Yvonne A.L. Lim, Rahmah Noordin, Muhammad Hafiznur Yunus,Norsyahida Arifin, Jerzy Marian Behnke, Siti Nursheena Mohd Zain
1Tropical Infectious Diseases Research and Education Centre (TIDREC), University of Malaya, 50603 Kuala Lumpur, Malaysia
2Department of Parasitology, Faculty of Medicine, University of Malaya, Kuala Lumpur. Malaysia
3Institute for Research in Molecular Medicine (INFORMM), Universiti Sains Malaysia, 11800 Pulau Pinang, Malaysia
4School of Life Sciences, University of Nottingham, University Park, Nottingham, NG7 2RD, UK
5Institute of Biological Science, Faculty of Science, University of Malaya, Kuala Lumpur, Malaysia
Keywords:Strongyloides stercoralis Migrant workers Microscopic examination Serological analysis PCR
ABSTRACT Objective: To investigate the status of Strongyloides(S.) stercoralis infections among migrant workers in Malaysia for the first time and identify risk factors.Methods: Four diagnostic methods were employed for the detection of S. stercoralis including microscopy, enzyme-linked immunosorbent assay (ELISA) using a commercial kit, ELISA using the rSs1a antigen and polymerase chain reaction (PCR). Low and semi-skilled workers from five working sectors (i.e. manufacturing, food service, agriculture and plantation,construction and domestic service) were tested on a voluntary basis.Results: The overall seroprevalence of S. stercoralis from 483 workers employing the ELISA commercial kit for IgG was 35.8% (n=173; 95% CI: 31.5%-40.1%) whereas seroprevalence using the rSs1a-ELISA was 13.0% (n=63; 95% CI: 10.0%-16.0%). Cross tabulation between the ELISA commercial kit and rSs1a-ELISA showed that only 6.4% (n=31; 95% CI: 4.2%-8.6%) of the samples were positive in both tests. Microscopic examination of all 388 fecal samples were negative; however subsequent testing by a nested PCR against DNA from the same samples successfully amplified DNA from three male subjects (0.8%; 3/388). Male workers, India and Myanmar nationality, food service occupation and those living in the hostel were statistically significant with seroprevalence (P<0.005).Conclusion: This is the first report on the epidemiology of S. stercoralis infections among the migrant workers in Malaysia. Our results highlight the importance of using appropriate diagnostic tools for detection. The presence of anti-S. stercoralis antibodies in the study population calls for improvements in personal hygiene and sanitation standards among migrant workers in Malaysia through control strategies including health education campaigns and programs aimed at increasing awareness and healthy behaviors.
1. Introduction
Strongyloides (S.) stercoralis is one of the four soil-transmitted helminths (STH) that cause infections categorized as neglected tropical diseases (NTD) infecting an estimated 30-100 million
How to cite this article: Sahimin N, Lim YAL, R Noordin, Yunus MH, Arifin N, Behnke JM, et al. Epidemiology and immunodiagnostics of Strongyloides stercoralis infections among migrant workers in Malaysia. Asian Pac J Trop Med 2019; 12(6): 250-257.people worldwide annually[1]. Infection is initiated by the infective larvae penetrating through intact skin followed by autoinfection,inflicting a persistent low-level infection that may last for many years. Clinical symptoms arise due to the host immune response and magnitude of the larval burden, however, the majority of low intensity level infections remain undetected. Symptoms may include diarrhea, pneumonia, gastrointestinal bleeding and hemorrhagic pneumonitis[2,3], while in immunocompromised patients,autoinfection may cause exacerbation and dissemination of the parasite burdens, resulting in a highly fatal hyper infection[4].
Strongyloidiasis is prevalent in socioeconomically deprived communities where hygiene and sanitation are compromised. The limited studies to-date in Malaysia have focused largely on the Orang Asli communities[3,5]. Low (1.2%) prevalence has been reported among aboriginal children from 6 villages in Post Brooke,Kelantan following detection using the formal-ether concentration technique[5]. While, Ahmad et al.[3] reported the absence of S.stercoralis larvae from 54 stool samples, serological examination of the same individuals revealed a prevalence of 31.5% but subsequent nested PCR only confirmed 3 (5.6%) positive samples[3]. In contrast,a study in Sarawak among hospitalized patients with gastrointestinal symptoms recorded a high prevalence (62.3%, n=48/77) using the pentaplex-PCR[6].
Approximately 232 million workers migrate worldwide to major cities around the globe to join the expanding urban workforce[7]in search of a better life and to escape financial adversities such as poverty and high unemployment in their home countries. Due to the rapid economic development in the 1970's, Malaysia has attracted multinationals from the region (i.e., Indonesia, Bangladesh, Nepal,Myanmar, India and Vietnam) including from countries where endemic infections are prevalent, and these pose a significant risk of public health problems for the local community[8-11].
In Malaysia medical screening is mandatory prior to entering the workforce however, screening for parasitic infections other than malaria, including for S. stercoralis, is not carried out routinely. Recent studies have shown that parasitic infections are prevalent among migrant workers in Malaysia[12]. Therefore,immunodiagnostic methods and molecular characterization were employed to record for the first time the presence of S. stercoralis infections among this cohort of the population and to identify risk factors associated with this infection.
2. Materials and methods
2.1. Study population, questionnaire and ethical consideration
In Malaysia, low and semi-skilled migrant workers are employed in the manufacturing, food services, construction, domestic services,agriculture and plantation. This study took place between September 2014 and August 2015 among migrant workers recruited on a voluntary basis from all employment sectors. Questionnaires were distributed and followed with face-to-face interviews in order to substantiate socio-demography information on each subject. The interview process was conducted via an interpreter in the event of low fluency in either Malay or English. All participants were informed of the nature of the study for maximum co-operation and for the completion of the consent forms. Ethical clearance(Reference number: MECID NO: 20143-40) was obtained from the University Malaya Medical Centre (UMMC) ethics committee.
2.2. Sample collection
All volunteers were provided with a screw-capped plastic container marked with a specific identification number and instructions were given on the faecal size required. All received faecal samples were preserved in 2.5% potassium dichromate solution. In addition,approximately 5 mL of venous blood were drawn using sterile syringes and needles (without anticoagulant) into a plain tube by a trained medical assistant. Both samples (faecal and blood) were transported back to the Parasitology Lab, Institute of Biological Science, Faculty of Science, University of Malaya for further screening. Faecal samples were kept at 4 ℃ while blood samples were spun at 1 500 rpm for 10 min and the collected sera were stored in -20 ℃ until further use.
2.3. Detection of immunoglobulin G to S. stercoralis
Serum samples were screened using the ELISA commercial kit(Strongyloides serology microwell ELISA, Scimedx Corporation, NJ,USA) for detection of specific anti-Strongyloides immunoglobulin G(IgG) in accordance with the manufacturer's instructions. A serum dilution 1: 64 was prepared using a dilution buffer. A volume of 100 μL of diluted serum was added into the each well followed with the positive and negative controls supplied with the kit and incubated for 10 min at room temperature(RT). The coated wells with Strongyloides antigen were then washed three times with washing buffer. Two drops of enzyme conjugate were added to each well, and further incubated for 5 min at RT and washed a further three times. Two drops of chromogen tetramethylbenzidine substrate were added to each well and incubated in the dark for 5 min at RT. Finally, two drops of phosphoric acid (1 M) were added into each well to stop the reaction. The wells were read at 450/ 620-650 nm via an ELISA Reader. A seropositive reading was indicated when the absorbance was greater than or equal to 0.2 OD units.Absorbance of less than 0.2 OD units indicated a negative result.
2.4. Detection of immunoglobulin G4 to S. stercoralis
The detection of anti-Strongyloides IgG4 antibody was determined using ELISA rSs1a recombinant antigen[13]. Prior to performing the test, each well of a high-binding microtitre plate (Nalgene Nunc Int., Rochester, NY, USA) was coated with 100 μL of rSs1a antigen at 10 μg/mL diluted in 0.06 M carbonate buffer (pH 9.6),and incubated overnight at 4 ℃. Next day, the plate was incubated at 37 ℃ for 1 h and washed 5 times for 5 min each, with 200 μL of PBS-T (0.05%) and shaken at 700 rpm. After the fifth wash,the wells were blocked with 200 μL of 3% bovine serum albumin(BSA). After 1 h incubation at 37 ℃ and a washing step, 100 μL of each serum sample at 1:100 dilution were added into each well,and incubated at 37 ℃, for 2 h. After a washing step, anti-human IgG4-HRP (Invitrogen, Carlsbad, CA, USA) at 1:2 000 was then added (100 uL/well) and the plate was incubated at 37 ℃ for 30 min.After a final washing step, 100 μL/well of ABTS substrate (Roche Diagnostics GmbH, Germany) were added and incubated at 37 ℃for 30 min. The absorbance value was read with an ELISA Multiskan spectrophotometer (Thermo Scientific, Waltham, MA, US) at 405 nm(test filter) and 490 nm (reference filter). An OD value of 0.165 was used as the cut-off value (COV) to discriminate between positive and negative results.
2.5. Faecal sample screening
All the collected faecal samples were processed by the formalin ethyl acetate sedimentation technique prior to microscopic examination with Lugol's iodine for the presence of S. stercoralis larvae. Approximately 1 to 2 g of sample was mixed with 7 mL of formalin and 3 mL ethyl acetate, the suspension was centrifuged and the pellet was examined under light microscopy.
2.6. Molecular analysis of S. stercoralis from fecal samples by nested PCR
Genomic DNA was extracted from all 388 faecal samples using NucleoSpin® Soil kit (MACHEREY-NAGEL, Düren,Germany) according to the manufacturer's instructions. DNA of S. stercoralis from fecal samples was amplified by a nested PCR technique targeting the internal transcribed spacer 1 (ITS1)region of the ribosomal DNA gene. Two primer sets were used in two separate reactions. The primary reaction consisted of a forward primer SS-FO: 5'-ATCCTTCCAATCGCTGTTGT-3' and reverse primer SS-RO: 5'-TTTCGTGATGGGCTAATTCC-3'.The secondary reaction forward and reverse primers were SS-FI:5'-GTAACAAGGTTTTCGTAGGTGA -3' and SS-RI: 5'-ATTTAGTTTCTTTTCCTCCGCTT -3' respectively[14]. The nested PCR was performed using Maxime PCR PreMix Kit (i-Taq)(iNtRON Biotechnology, Inc.) in 20 μL volume reaction that contained i-TaqTM DNA Polymerase (5 U/μL) (2.5 U), 1 ˟ Reaction buffer (10˟), deoxynucleoside triphosphate (dNTPs) (2.5 mM each) and Gel loading buffer (1˟). Distilled water, primers (100 nM each) and DNA template (2 μL) were added to the premix. Cycling conditions of PCR consisted of an initial denaturation at 94 ℃ for 5 min and 35 cycles of 94 ℃ for 45 s, 58 ℃ for 1 min, 72 ℃ for 1 min and a final extension at 72 ℃ for 5 min. Subsequently, 2 μL of the primary PCR products were subjected to a secondary PCR performed at 94 ℃ for 2 min and 30 cycles of 94 ℃ for 45 sec,60 ℃ for 45 sec, 72 ℃ for 1 min and a final extension at 72 ℃ for 5 min. PCR products were subjected to electrophoresis through 2% (w/v) agarose and visualized in a UV transilluminator after staining with RedSafeTM Nucleic Acid Staining Solution (iNtRON Biotechnology, Inc, Korea).
2.7. Data analysis
Data were analyzed using bespoke software for prevalence and 95% confidence interval (95% CI)[15]. The prevalence data were then statistically analyzed with maximum likelihood techniques based on log linear analysis of contingency tables using SPSS software statistic program version 22.0. Infection was considered as a binary factor; presence/absence of parasites or presence/absence of anti-Strongyloides antibodies (immune status). Socio-demographic factors considered in the analysis included intrinsic [sex (males and females); age (<25, 25-34, 35-44, 45-54 and >54 years old) and nationality (Indonesia, Bangladesh, Myanmar, India and Nepal)] and extrinsic [employment sector (construction, manufacture, plantation,food service and domestic); years of residence in Malaysia (< than 1 year and > than 1 year); type of accommodation (own/rent house,work site and hostels) and education (primary school, secondary school, university and no formal schooling)] factors.
3. Results
3.1. Socio-demographic characteristics
A total of 610 participants were recruited of which, 483 (79.2%)provided blood and 388 (63.6%) faecal samples. Only 306 volunteers provided both blood and faecal samples (Figure 1).
All 483 blood donors originated from rural backgrounds in their respective countries of origins. The majority were Indonesians(n=246, 50.9%) and slightly more than three quarters were males(males: n=374, 77.4%; females: n=109, 22.6%). The sociodemographic breakdown of the workers is described in Table 1.
Slightly more than half who provided stool were Indonesian(n=167; 43.0%), followed by Nepal (n=81, 20.9%), Bangladesh(n=70, 18%), India (n=47, 12.1%) and Myanmar (n=23, 5.9%). The socio-demographic profile of this subset comprised predominantly 304 males (78.4%) and 84 females. Among the males, 37.4% were between 25 to 34 years old (n=145), 29.4% were younger than 25(n=114) and 23.2% older (n=90) for 35 to 44 years. The majority were involved in the domestic sector (n=105, 27.1%), followed closely by the service sector (n=104, 26.8%), while, only a small proportion were from among those working on plantations (n=71,18.3%), manufacturing (n=61, 15.7%) and construction (n=47,12.1%) sectors.

Figure 1. Biological sample collection and workflow process from five working sectors in Peninsular Malaysia.
3.2. Fecal samples collection and screening
A total of 388 feacal samples from the study cohort were successfully collected and fixed in formalin-ether. Microscopic screening of all samples failed to detect any presence of S. stercoralis larvae. However, other intestinal parasites were identified; Ascaris lumbricoides (43.3%), hookworms (13.1%), Entamoeba histolytica/dispar (11.6%), Giardia spp. (10.8%), Trichuris trichura (9.5%),Cryptosporidium spp. (3.1%), Hymenolepis nana (1.8%) and Enterobius vermicularis (0.5%)[12].
3.3. Seroprevalence using ELISA commercial kit and rSs1a-ELISA
The overall seroprevalence of S. stercoralis based on the ELISA commercial kit for immunoglobulin G (IgG) was 35.8% (n=173;95% CI: 31.5%-40.1%). Meanwhile, seroprevalence using the rSs1a-ELISA was 13.0% (n=63; 95% CI: 10.0%-16.0%). Cross tabulation between values using the ELISA commercial kit and rSs1a-ELISA showed that only 6.4% (n=31; 95% CI: 4.2%-8.6%) of the samples were positive in both tests (Table 2).
3.4. Intrinsic factors association to infection
Seroprevalence of S. stercoralis was analysed statistically in relation to intrinsic factors including host sex, age and nationality(Table 1). The results based on the rsS1a-ELISA identified two significant factors i.e. host sex and nationality (Table 1). There was a significantly higher seroprevalence among male workers compared with females (Χ21= 8.297, P = 0.004) and those originating from India and Myanmar compared with other countries (Χ24=23.073,P<0.001).
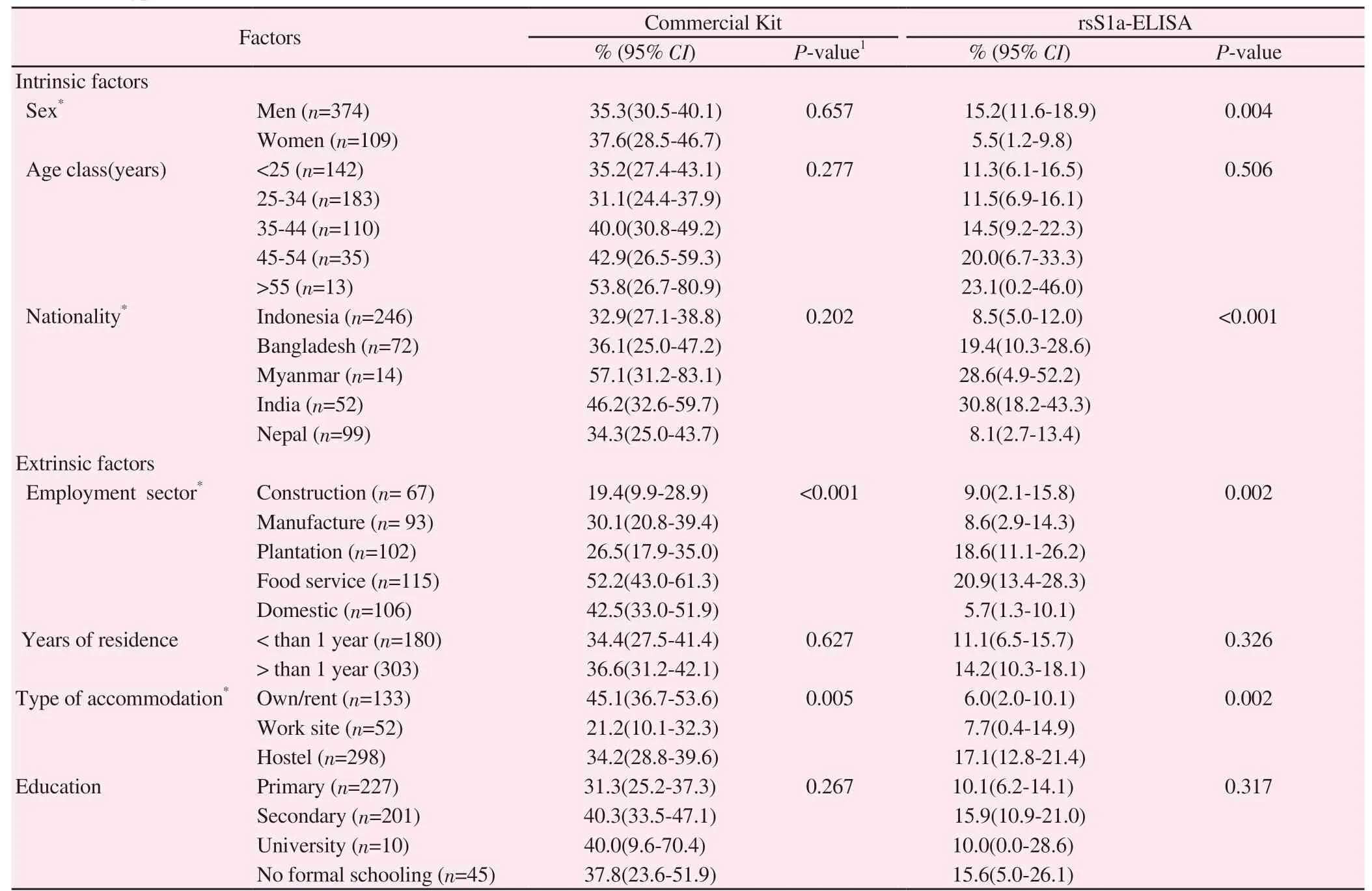
Table 1. Seroprevalence of Strongyloides stercoralis infections among migrant workers in Malaysia according to sex, age, nationality, employment sector, years of residence, type of accommodation and education level.
3.5. Extrinsic factor association to infection
Of the four extrinsic factors considered (Table 1), only two significantly affected seroprevalence i.e. employment sector and type of accommodation. Based on the ELISA commercial kit, prevalence was significantly higher among workers in the food service sector(Χ24= 28.838, P < 0.001) and those living on their own and in hostels (Χ22= 10.463, P = 0.005) (Table 1). Similarly, the results of the rSs1a-ELISA revealed that infection was significantly associated with workers in the food service sector (Χ24= 17.101, P = 0.002)and those living in the hostels (Χ22= 12.576, P = 0.002).
3.6. Molecular analysis
Subsequent confirmation using a nested PCR against DNA from all stool samples showed successful DNA amplification, with a target amplicon of approximately 680 bp, from three samples (0.8%;95% CI: 0.2%-2.2%). All three positive amplifications were from males (1.0%; 95% CI: 0.2%-2.9%) with residence in this country of more than a year (1.2%; 95% CI: 0.2%-3.4). Two samples were from subjects originating from India (4.3%; 95% CI: 0.5%-14.5%)and one from Indonesia (0.6%; 95% CI: 0.0%-3.3%). Both Indian workers were employed in the food service sector (1.9%; 95%CI: 0.2%-6.8%) and were also found to be infected with Ascaris lumbricoides. Meanwhile the worker from Indonesia was employed in the domestic sector (1.0%; 95% CI: 0.0%-5.2%). These three positive subjects were aged between 35 to 54 years old (2.5%;95% CI: 0.5%-7.2%) and were also seropositive using the ELISA commercial kit for IgG. All the negative samples were also subjected to molecular analysis and ELISA screening, and were all confirmed as negative.
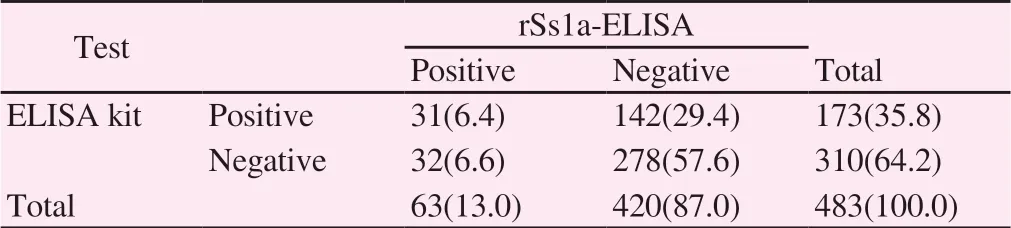
Table 2. Crosstabulation of ELISA commercial kit and rSs1a-ELISA[n(%)].
4. Discussion
To-date studies on strongyloidiasis among the population of Malaysia have been of only minor concern and limited to the Orang Asli communities[3,5]. However, the strong economic presence in early 1970's drew many workers to the cities of Malaysia particularly from low socio-economic neighbouring countries where many parasitic infections including S. stercoralis are still endemic and responsible for disease among the inhabitants. This infection is not included presently in the list of mandatory illnesses screened for prior to employment in this country, hence this is the first attempt to record the presence of S. stercoralis infection and its extent among migrant workers in Malaysia.
The majority of workers originated from rural areas in their respective countries where parasitic infections are still very much prevalent. Over a third of the workers screened for Strongyloides infection with the commercial kit were seropositive and this is in agreement with global values which have been recorded as generally between 10% and 40% in endemic countries in tropical and subtropical regions[16]. In the Southeast Asia region, prevalence of S. stercoralis infection has been found to vary between countries[Cambodia (2.6%-44.7%), Thailand (0.1%-57.0%), Indonesia (0.8%-5.4%), China (0.04%-17.9%), Lao PDR (1.4%-41.0%) and Vietnam(0.1%)][17].
Diagnosis of latent infections is difficult due to the limitations of current methods i.e parasitological and serological. The varying prevalence values recorded herein resulted from differences in the sensitivity of the various techniques that were used. This study employed four screening techniques with the microscopic technique for larval detection in faecal samples[3,5,18] being found to be the least sensitive method. This method was limited to only a one time stool sampling and failed to detect any positive samples. Meanwhile,the commercial IgG-ELISA results recorded a relatively high seropositivity in the targeted population but it is important to stress that this assay reflects previous history of infection, and does not confirm current active infection since the detected antibodies may be persisting from a past infection or chronic autoinfection[3,19].Nevertheless, the ELISA method has advantages over microscopy as it allows large-scale automated screening and the assay is easy to perform with no technical skills required for identification and diagnosis[3,19,20].
The low concordances (6.4%) in the cross tabulation results between both ELISA tests were probably due to differences in the antigens and secondary antibodies that were used. The commercial kit uses crude Strongyloides antigen, in combination with IgG as the secondary antibody, while rSs1a-ELISA uses a recombinant antigen of S. stercoralis, with IgG4 as the secondary antibody. Previously,significant cross-reactions with other helminthic infections (filariasis,ascariasis, and schistosomiasis) have been observed in assays utilizing crude Strongyloides parasite antigens[21]. Therefore, much attention has focused on the development of a recombinant antigen to improve serological assays for strongyloidiasis. As such, the newly reported S. stercoralis recombinant antigen (rSs1a) as revealed by Arifin et al.[13] showed high sensitivity (96%) and specificity (93%), and is potentially useful for serodiagnosis of strongyloidiasis.
Despite being the most abundant circulating antibody in 95% of patients[22], the major disadvantage of assays for anti-Strongyloides IgG is their cross-reaction with filarial antigens[21]. On the other hand, the assay for anti-Strongyloides IgG4, a major component of total IgG, has been shown to be far more specific in the detection of human strongyloidiasis in subjects that also harbour concurrent infections with other helminths[23,24]. Anti-Strongyloides IgG4 has also been shown to play a prominent role in chronically infected patients with Strongyloides[25-27]. As none of the subjects from this study appeared to be symptomatic, they were assumed to be asymptomatic, although as shown above many were also co-infected with other parasites. These two factors may have contributed to some of the discrepancies between the results from the two immunoassays in this study.
Of the four techniques employed in this study, nested PCR proved to be the most sensitive diagnostic tool for confirmation of active current infection, with DNA from three stool samples being successful amplified. Based on the rSs1a-ELISA and nested PCR results, infections were primarily recorded in male workers. A recent review recognized host-sex as one of the risk factors for S. stercoralis infection in Southeast Asia[17]. In rural Lao PDR, Conlan et al.[28]showed that the risk of infection was higher in male compared with female subjects (OR=2.76). Similar findings were also recorded in Cambodia with OR of 1.4 for males (P = 0.001)[29] and among males in all age groups(OR: 1.7; P < 0.001)[30]. In Thailand, infections in boys (35.2%) were significantly higher than in girls (16.8%) (P = 0.003)[31] and in Northern Ghana, a significantly higher prevalence (12.7%) was recorded in males compared to females (10.6%)[32], as was also the case in Okinawa, Japan (males: 14.0%; females: 6.8%)[33].
Host-sex plays a significant role due to the higher occupational involvement of males in the agricultural and plantation sectors[3].Frequent contact with contaminated soil and/or water is likely to predispose more males to S. stercoralis infection. In South Eastern provinces of China[34] and the Yunnan province in the South of China[35], high S. stercoralis infections have been detected among farmers. While in Europe and in the United States, infections have been found predominantly among the miners and plantation workers[16]. Despite no significant association with occupation, this latter study detected a higher prevalence among workers in the food services sector, which is mainly dominated by workers from India.The results of the present study have important public health implications as transmission of S. stercoralis is fundamentally due to poor sanitation and poor personal hygiene practice, in addition to inappropriate methods for sewage disposal[16]. A community based survey of the urban slum community in Bangladesh showed high prevalence of infection (29.8%)[36] which was also recorded in Nepal (22.8%)[37]. However, India[38,39] and Indonesia[40] recorded lower prevalence of 6.6% and 7.6%, respectively. A study in rural Cambodia recorded a significant reduction of 39% in strongyloidiasis cases in households with properly functioning latrines[41]. A high prevalence of up to 60% can be expected in resource-poor countries linked to ecological and socioeconomic factors. Meanwhile in urban and developed countries, very low prevalences of infection have been reported, except for in slum areas in the big cities[16].
Other known risk factors such as behavioral patterns are known to also play a role in transmission with most infections acquired during childhood and sustained through auto-infection into later life[16]. Several studies have reported individuals who have sustained continuous infection with S. stercoralis for more than 75 years[42-44]. These are possibly explained by the parasite's capacity for reproduction within a human host (endogenous autoinfection) hence resulting in persisting worm burdens.
Most soil-transmitted helminths studies in Malaysia have omitted screening for S. stercoralis, while others have adopted the low sensitivity conventional technique based on microscopy[45].A worldwide review has highlighted the low sensitivity of the diagnostic methods applied in many community-based studies with concerns also about their specificity[16]. The asymptomatic nature of many helminth infections, coupled with difficulties in accurate diagnosis, often leads to under-diagnosis. The latest developed tools for the diagnosis of Strogyloidiasis i.e. the ELISA-rSs1a and nested PCR have enabled some of these issues to be overcome, as shown in this study. Therefore, it is recommended that both of the techniques(ELISA rSs1a based on serum and hence reflecting previous history of infection and the nested PCR based on current presence of parasite antigens in host faeces and hence reflecting current presence of the parasite) should be applied in tandem in future studies assessing the extent and importance of human strongyloidiasis in affected communities.
Our current results have provided baseline information on the epidemiology of S. stercoralis infections among migrant workers in Malaysia and have highlighted the importance of using appropriate diagnostic tools in detection of this infection. In addition to the use of better diagnostic tools, workers should be exposed to health education campaigns and programs aimed at increasing awareness of the importance of personal hygiene, good sanitation and healthy behaviors in controlling S. stercoralis infection.
Conflict of interest statement
RN and NA are named as inventors in a patent titled “Strongyloides stercoralis protein and/or corresponding DNA and RNA sequences for application in diagnosis” filed in Malaysia (PI 2015002836) and at PCT [PCT/MY 2016/050053].
Acknowledgements
The authors are very grateful to the Ministry of Health, Malaysia and all collaborators from companies and agencies in Malaysia for their support to this study. Special thanks also go to all medical staff and nurses from University Malaya Medical Centre (UMMC)and Hospital Universiti Kebangsaan Malaysia (HUKM) for their technical assistance. Most importantly, the authors would like to thank all the respondents who have voluntarily participated in this study.
Foundation project
This research work was funded by University of Malaya, PPP grant(PG040-2014A), Fundamental Research Grant Scheme (FRGS)from Ministry of Higher Education (FP015-2014B), UM/MoHE High Impact Research Grant (UM.C/625/1/HIR/MOHE/MED/23)and Universiti Sains Malaysia, Malaysian Ministry of Higher Education grant (HICoE 311/CIPPM/4401005).
 Asian Pacific Journal of Tropical Medicine2019年6期
Asian Pacific Journal of Tropical Medicine2019年6期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Community-acquired pneumonia with Acinetobacter radioresistens bacteremia in an immunocompetent host: A case report
- Optimized combinations of statins and azoles against Acanthamoeba trophozoites and cysts in vitro
- Anticancer activity of Mahonia leschenaultii methanolic root extract and berberine on Dalton’s ascitic lymphoma in mice
- Symptoms of dengue at the acute and post-infection stage in the Western Province, Sri Lanka: A cross-sectional study
- Laboratory diagnosis of schistosomiasis mansoni: Current status and future trends