
A meta-analysis of randomized controlled trials of combined treatment with DGSN and western medicine on diabetic peripheral neuropathy
2019-04-23 07:30:44XiaokeFengLiqunXie
Clinical Research Communications 2019年1期
Xiaoke Feng,Liqun Xie
1Department of Traditional Chinese Medicine, The First Affiliated Hospital of Nanjing Medical University,Nanjing,China. 2Graduate Institute of Integrated Medical of Nanjing Medicine University
Introduction
Diabetic peripheral neuropathy (DPN) is one of the chronic complications of diabetes, with strong secretiveness, slow morbidity, gradually aggravated symptoms and difficult reversibility. According to the national DPN screening conducted by Chinese Society of Diabetes,the prevalence of DPN in China is 52.97%[1]. Its specific pathogenesis remains unclear. It is believed that the occurrence of DPN is related with metabolic disorders, oxidative stress, vascular injury,neural ischemic lesion, and autoimmune disorder,resulted from long-term hyperglycemia[2].At present,treatments with western medicine (WM) mainly include controlling of blood glucose, blood pressure and blood lipid, nourishing nerves, dilating blood vessels, and reducing peripheral nerve damages through blocking polyol pathway by antioxidant.However, the clinical effects are not ideal and there is no treatment to reverse the DPN progression.
In recent years, more and more researches focus on the application of traditional Chinese medicine (TCM)in the treatment of DNP. DNP is divided into four syndromes, including deficiency of Qi and blood, Yin deficiency, Yan-deficiency of spleen and kidney and blood stasis in TCM [3]. To further clarify the clinical effect of DGSN in the treatment of DNP,we use metaanalysis to systemly reviewed articles about the application of combined treatment of DNP with DGSN and western medicine in recent 5 years. We concluded that, on the basis of western medicine, combined treatment with DGSN can improve the efficacy of DNP, providing requisition basis for guiding the clinical application of drugs.
1 Materials and methods
1.1 Search strategy and selection criteria
Seven databases, including Chinese National Knowledge Infrastructure (CNKI), Chinese Biomedical Database (CBM), Wanfang full-text database,Weipu database (VIP), MEDLINE, PubMed,and Embase, were retrieved with computer; The retrieval period was from January 2012 to December 2017. Related grey literatures, including master's and doctor’s dissertation, were also searched according to the selected articles. The retrieval was performed with combination with keywords and free words. The basic search terms in English and China were DGSN, type 2 diabetes mellitus, and diabetic peripheral neuropathy,and secondary retrieval was performed with"syndrome", "traditional Chinese medicine", and"traditional Chinese and western medicine" as keywords. Independent two-person and two-machine retrieval was used until the number of retrieved literatures was consistent.
1.2 Inclusion and exclusion criteria
1.2.1 Inclusion criteria
(1) Study type: randomized controlled trial (RCT)was required to be included in the study.(2)Study subjects: annual patients with type 2 diabetic peripheral neuropathy were included. The diagnostic criteria were consistent with the diagnosis and treatment consensus of diabetic peripheral neuropathy developed by the Chinese Medical Association in 2013. (3) Intervention measures: the experimental group was given DGSN combined with western medicine treatment including mecobalamine taken orally or intravenous drip, octanoic acid intravenous taken orally or drip, or Vitamin B12 intramuscular injection; the control group was given western medicine treatment alone.The basic treatment was oral drugs combined with or without insulin treatment.The patients’blood glucose levels were controlled in a stable range, with no limitations in drug dosage, combination with other drugs, and course of treatment. (4) Outcome indexes: Main outcome indexes were total effective rate of clinical efficacy (The efficacy evaluation criteria of the total effective rate were all made by referring to the efficacy criteria of diabetic peripheral neuropathy in
1.2.2 Exclusion criteria
Literatures that do not meet the inclusion criteria were excluded according to the literature exclusion criteria. The literature exclusion criteria were: (1) literatures are non-randomized controlled trials; (2) literatures are animal experiments or literature review; (3) diagnostic criteria are not clear or no diagnostic criteria; (4)control group was not pure western medicine treatment.
1.3 Data extraction
Two researchers independently screened the literatures,extracted data and evaluated the methodology quality of studies selected according to the inclusion and exclusion criteria.If there is a disagreement,discussion will be performed to settle.The extracted data contents mainly include:(1)researcher and publication time;(2)research design type; (3) sample size, sex ratio and average age of patients in the experimental group and control group; (4) intervention measures; (5) outcome indicators. The outcome indicators included clinical symptoms, TCSS score, TCM syndrome score, nerve conduction velocity and so on. Then, RCT bias risk assessment tools recommended by the Cochrane System Evaluator Manual 5.1.0 [4] were used to evaluate bias risk of study included.
The established Jadad scale was used to evaluate the quality of included RCTs. Items included randomization, concealment of allocation, double blinding, withdrawals, and dropouts. 0 to 3 points indicated poor or low-quality trials, and 4 to 7 points indicated high-quality trials. The inconsistencies with quality assessment were discussed until consensus was reached.
1.4 Data analysis
Meta-analysis of studies included according to the inclusion criteria was performed using Rev Man 5.3 software provided by Cochrane Collaboration.Measurement data used weighted mean as the effect size.Enumeration data used relative risk or ratio as the effect size. Study and the overall confidence interval adopted 95% confidence interval. Chi-square test was used for heterogeneity analysis of included literatures.P>0.1,I2≤50%was considered as small heterogeneity or no heterogeneity. Meta-analysis was carried out using a fixed-effect model. P < 0.1,I2>50% was considered to be heterogeneous. If so, the reason of heterogeneity was analyzed and then a random-effect model was applied. For literatures with oversize heterogeneity, perceptual analysis was performed to explore the source of heterogeneity. Ultimately,descriptive analysis was performed using forest diagram,and bias analysis was performed using funnel diagram.
2 Results
2.1 Literature retrieval results
Figure 1 showed the process of study selection. 18 articles (17 studies) including a total of 1530 patients with diabetic peripheral neuropathy published since 2012 were included according to the inclusion criteria[4-21]. The clinical total effective rates of combined treatment of diabetic peripheral neuropathy with DGSN and WM were observed in each paper. 9 articles observed the changes in TCSS scores. 10 articles observed the changes in sensory conduction velocity of nervus peroneus communis before and after treatment. 8 articles observed the changes in motor conduction velocity of nervus peroneus communis before and after treatment. 3 articles observed changes in scores of TCM syndrome. For the treatment of the control group,8 articles adopted oral administration of mecobalamin, 1 article used static drops of mecobalamin, 2 articles used oral administration of octanoic acid, 2 articles used static drops of octanoic acid, 1 article used epastar capsules, 1 article used intramuscular injection of vitamin B12,and 3 articles did not use any control western medicine.Details were shown in Table.1.
2.2 Basic characteristics and quality evaluation of the studies included
17 study articles were included in this study.Sample capacity ranged from 20 to 210,with 1690 patients. Basic features of included literatures were shown in Table 1. This included the number of participants, sex ratio, mean age, interventions,and course of treatment, outcome measures, and adverse events indicators. The results of quality evaluation of included literatures were shown in Table 2. Most of the literatures clearly described the random methods and double-blind analysis.
2.3 Results of meta-analysis
2.3.1 Total clinical efficiency
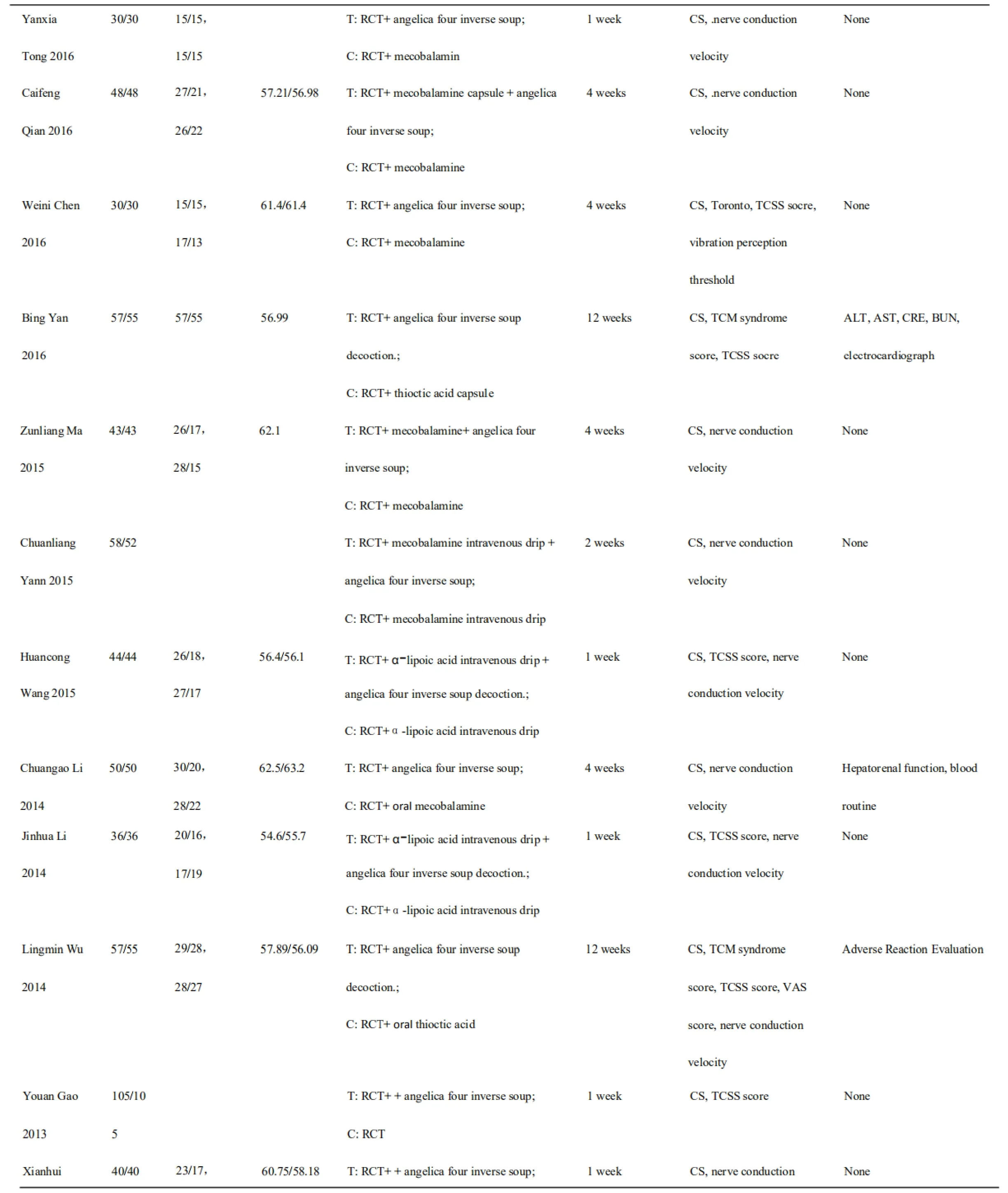
Total clinical efficiency was used to describe the clinical efficiency in all of the 17 articles.Heterogeneity test results showed that I2=0%,P=0.93, so fixed effect model was used for Metaanalysis. The results showed that the estimated median survival time effect was 4.36,P<0.00001,indicating that the median survival time of the TCM treatment group was 4.36 times than that of control group, and the difference was statistically significant. The results of Meta-analysis forest diagram showed that, after treatment with DGSN,the total clinical efficiency of experimental group was significantly higher than that of control group.(Figure.2-3).
2.3.2 TCSS scores
A total of 9 articles used TCSS scores to evaluate the improvement of clinical symptoms of patients before and after treatment. TCSS scores of two groups were decreased after treatment. However,the TCSS scores in the experimental groups were decreased significantly. It is prompted that the treatment method is better than that in control group. 8 articles showed differences with statistical significance.Heterogeneity test results showed that I2=88%, P<0.0001, so random effect model was used for Meta-analysis.The results showed that the median survival time effect was estimated to be 1.11,P=0.0010,indicating that the median survival time of the TCM treatment group was 1.11 times than that of control group, and the difference was statistically significant.(Figure.4-5).

Fig.1 Processes and results of literature selection
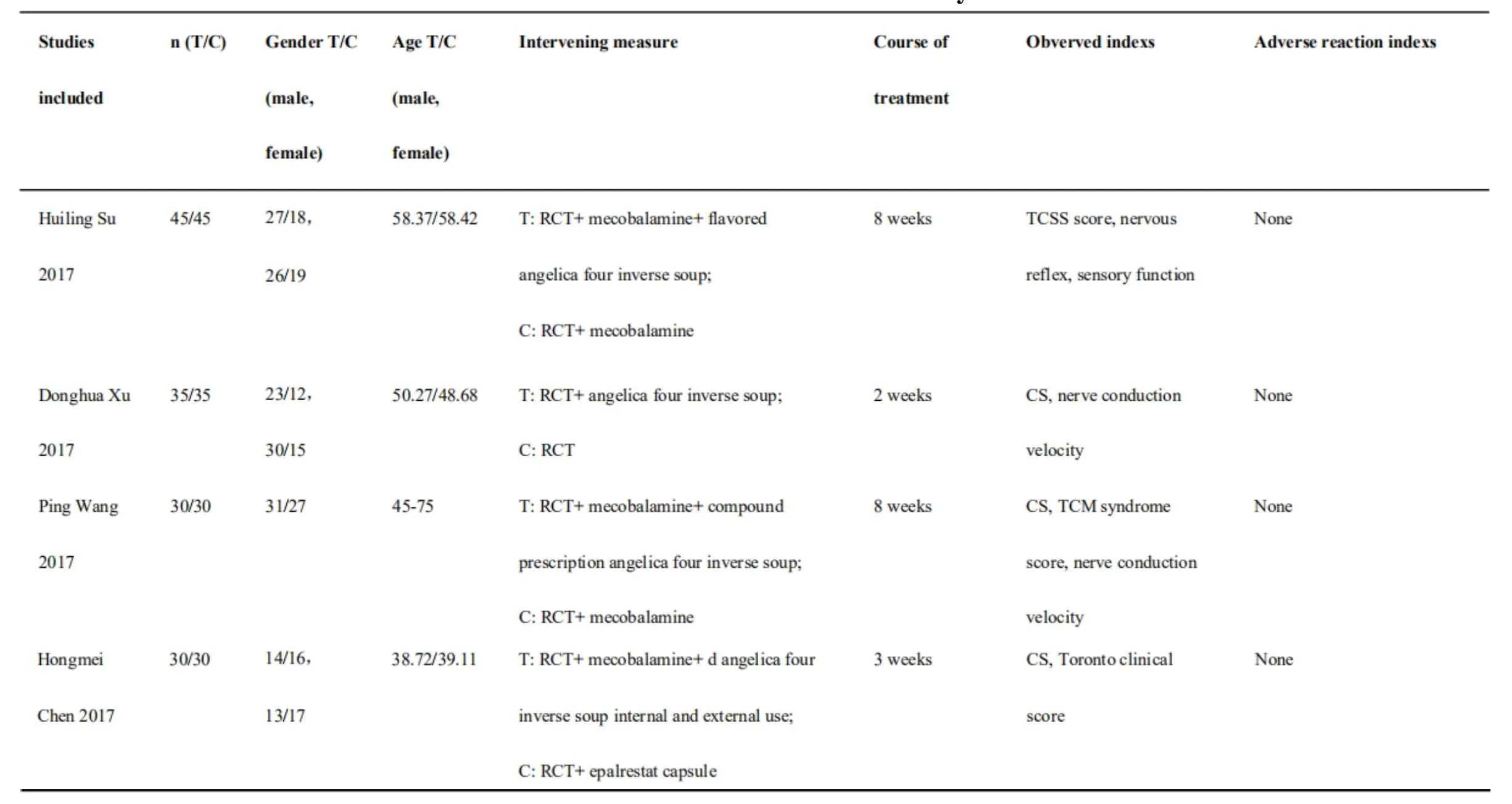
Table 1 Basic features of selected study
?

Note:RCT:Routine Complex Treatment;CS:Clinical symptom

Table 2Quality evaluation of methodology of selected articles
2.3.3.Nerve conduction velocity
A total of 10 articles compared the nerve conduction velocity before and after treatment in the experimental group combinedly treated with DGSN and in control group treated with western medicine alone. However,the selected nerves were not exactly the same,including nervus peroneus communis, nervus tibialis,and nervus medianus.There were some literatures detecting MNCV and SNCV of selected nervus at the same time, while some other literatures detecting one item of them only.Thus MNCV and SNCV of nervus peroneus communis used in most researches were used as the indicators of analysis.The analysis results showed that conduction velocities of motor nerve and sensory nerve of nervus peroneus communis were significantly higher after combined treatment with DGSN than those in control group. In the analysis of MNCV of nervus peroneus communis, the heterogeneity test results showed that I2= 99%, P < 0.00001, so random effect model was used for Meta-analysis.The results showed that the estimated median survival time effect was 4.2, P < 0.00001, indicating that the median survival time of the TCM treatment group was 4.2 times higher than that of control group,and the difference was statistically significant. In the analysis of SNCV of nervus peroneus communis, the heterogeneity test results showed that I2= 99%, P <0.00001, so random effect model was used for Metaanalysis.The results showed that the estimated median survival time effect was 4.74, P < 0.00001, indicating that the median survival time of the TCM treatment group was 4.74 times higher than that of control group, and the difference was statistically significant.(Figure.6-9).
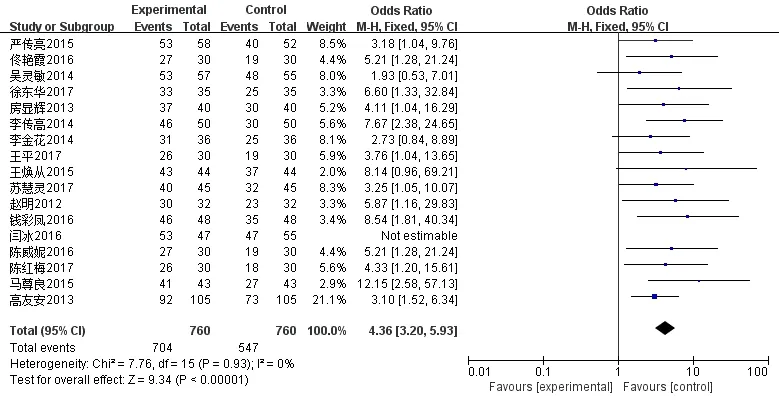
Fig.2 Meta-analysis forest diagram of total clinical efficiency
Fig.3 Meta-analysis funnel diagram of total clinical efficiency
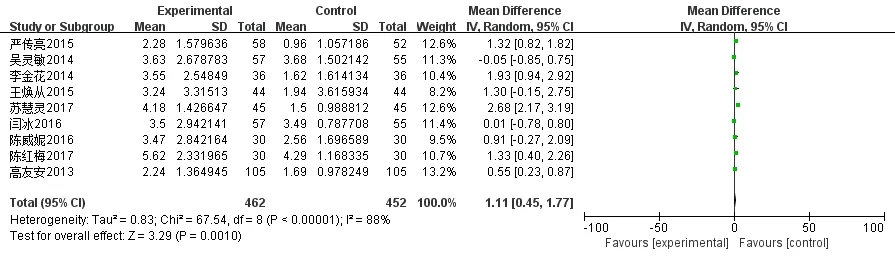
Fig.4 Meta-analysis forest diagram of TCSS scores
2.3.4 TCM syndrome scores
A total of 3 literatures reported that the TCM syndrome scores of experimental group were significantly lower than those of control group.

Fig.5 Meta-analysis funnel diagram of TCSS scores
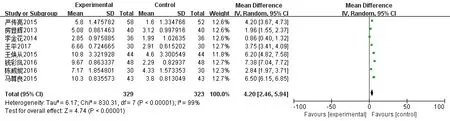
Fig.6 Meta-analysis forest diagram of MNCV of nervus peroneus communis
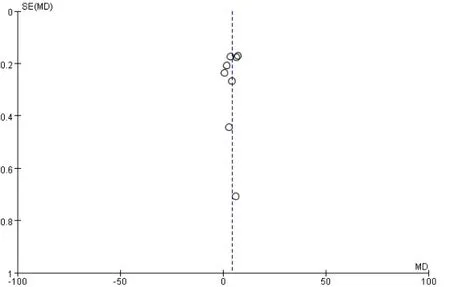
Fig.7 Meta-analysis funnel diagram of MNCV of nervus peroneus communis
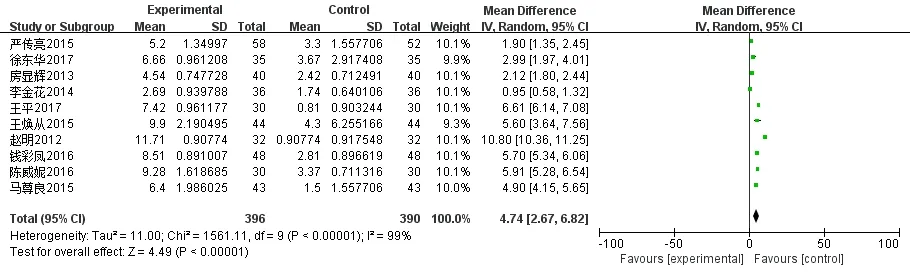
Fig.8 Meta-analysis forest diagram of SNCV of nervus peroneus communis
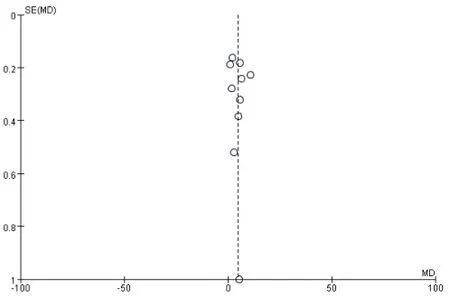
Fig.9 Meta-analysis funnel diagram of SNCV of nervus peroneus communis
2.3.5 Adverse effects
Only 3 literatures in this study used liver and kidney functions,blood routine and other indicators to observe the adverse effects in the treatment process. Other studies did not involve this part.
3 Discussion
Diabetes belongs to the category of "consumptive thirst" in TCM. There is no clear name for diabetes peripheral neuropathy in TCM, but there is description of symptoms,such as"extremities numbness"and"leg knee is fine", etc., long after collateral in TCM literatures.Thus, it can be classified as certification of"Bi syndrome", "weak" or "blood", etc., according to the symptoms. So analysis of diabetes peripheral neuropathy syndromes mainly included Yinjin loss after long illness, Yin-loss to Yang, Jin-less, body fluid-deficiency and blood-loss, tendon and vessel malnutrition, systemic vein stasis, Qi and blood notfree, and then extremities numbness and not-warm,then even extremities cold, and so on. “Deficiency”and “stasis” are the key links in pathogenesis changes of DNP. DGSN, which has effects of warming channel to remove coldness, nourishing blood and fluxing pulse, is a traditional Chinese medicine prescription from treatise on Shang Han Za Bing Lun by Zhongjing Zhang. In this prescription, Dang gui has the effect of invigorating circulation of blood and nourishing blood,and is adept in relieving pain.Radix paeoniae alba has the effect of nourishing blood and jointing venture,slowing and relieving pain. It also benefits to blooding effect of Dang gui. Asarum and cassia twig can invigorate pulse-beat. Evodia rutaecarpa can Wen Zhonghang gas,relieve pain and pursue cold.Tong cao can dredge blood vessels.Prepared Liquorice Root and jujube together can replenish Qi and strengthen the middle warmer. The full prescription can warm yang and dispell cold, nourish blood and unclog arteries,remove cold evil from meridians and repair camp blood. It is warm but not dry, complementary but not stasis.It is suitable to treat diabetic neuropathy of blood deficiency and haemorrheological nature.
This study reviewed relevant clinical researches in recent 5 years. Analysis results indicate that proper use of DGSN combined with western medicine to treat diabetic peripheral neuropathy according to traditional Chinese medicine clinical angelica in clinic, is more effective in improving patients’symptoms, such as limbs numb, cold and pain than treatment with western medicine alone.Major performance is that the clinical total effective rate was significantly increased, TCSS scores were reduced, and nerve conduction velocity was improved significantly, thus improving the quality of patients’ life. Moreover,there is no significant adverse reaction in studies included, which is superior to treatment with western medicine alone.
Comprehensive analysis of research methods involved in this study shows the deficiencies of experiments about the curative effects of DGSN in treatment with DPN in many clinical studies,which is worthy of further discussion. The following aspects are involved: first,inhomogeneity of patients included,including age,sex ratio, foundation treatment, leading to the incomparability between clinical studies. Only the improved symptoms and objective indexes of nerve conduction velocity of patients in this study were compared before and after treatment.Second,the duration of study differs significantly.Observation time involved in articles ranges from 1 weeks to 12 weeks. No-treatment time may result in different curative effect. It cannot be sure whether it is one of the reasons leading to different results. Third, the observation indicators used by some researches are too simple, and do not have objective indicators to fully reflect the improvement of nerve conduction. Forth, the indicators of adverse reactions are not comprehensive.
In conclusion, the current combined treatment of diabetic peripheral neuropathy with DGSN and western medicine according to syndrome differentiation in clinic is superior to treatment with western medicine alone.However,multi-center clinical trials with larger sample, more comprehensive observing indexes and more rigorous research conditions are needed to further prove its validity.And its mechanism is worth further discussion and exploration.
1. Zhigang Zhao. Clinical screening study of diabetic peripheral neuropathy. Chinese Medical Association, Chinese Diabetes Society. The 16th National Academic Conference Proceedings of the Chinese Diabetes Society. Beijing: Chinese Medical Association,2012:2.
2. You Lu,Yingli Lu.Advance in the pathogenesis of diabetic peripheral neuropathy.Journal of Shanghai Jiaotong University (medical version), 2017, 37:1441-1445.
3. Hongjing Tong. Treatment based on syndrome differentiation in Chinese medicine of diabetes peripheral neuropathy. Jilin Chinese Medicine,2017,37:1200-1202.
4. Bing Yan, Lingmin Wu, Liying Wang, et al.Clinical Observation of Lipoic Acid and Dangguisini Decoction on the Treatment With Diabetic Peripheral Neuropathy. Chinese Health Standards Management,2016,7,21:129-132.
5. Chuanliang Yan. The effect analysis of combined Chinese traditional medicine and western medicine in the treatment of diabetic peripheral neuropathy.Practical Combination of Traditional Chinese and Western Medicine Clinical,2015,6,15:60-67.
6. Youan Gao. The clinical effect observation of flavored angelica four inverse soup combined mecobalamine and insulin strengthen therapy in the treatment of diabetes peripheral neuropathy.Clinical Journal of Chinese Medicine, 2013, 5, 2:16-17.
7. Donghua Xu. Analisis of the effects of angelica four inverse soup on improving nerve conduction velocity and curative effect in treatment of coldcoagulation blood-stasis-type diabetes peripheral neuropathy. Modern Diagnosis & Treatment, 2017,1,28:228-230.
8. Chuangao Li. The clinical effect observation of angelica four inverse soup in the treatment of diabetes peripheral neuropathy. Clinical Journal of Traditional Chinese Medicine,2014,26,1:44-45.
9. Hongmei Chen, Jianfang Wu, Huanan Tan. The clinical effect observation of angelica four inverse soup in the treatment of diabetes peripheral neuropathy.Journal of New Chinese Medicine,2017,3,49:56-57.
10. Yanxia Tong.The clinical effect observation of angelica four inverse soup in the treatment of diabetes peripheral neuropathy. Journal of cardiovascular disease with combination of TCM and Western Medicine,2016,9,4:67-68.
11. Ming Zhao. The clinical effect observation of angelica four inverse soup in the treatment of diabetes peripheral neuropathy. Chinese Manipulation & Rehabilition Medicine, 2012,8,3:180-181.
12. Caifeng Qian. The clinical effect observation of angelica four inverse soup in the treatment of diabetes peripheral neuropathy. Chinese Medical Information,2016,8:33.
13. Huiling Su. 45 cases of flavored angelica four inverse soup combined with western medicine in the treatment of diabetes peripheral neuropathy. Traditional Chinese Medicinal Research,2017,3,30:27-28.
14. Zunliang Ma. The effect observation of flavored angelica four inverse soup combined mecobalamine in the treatment of diabetes peripheral neuropathy. Journal of Modern Chinese and Western Medicine, 2015, 10, 24:3846-3847.
15. Jinhua Li, Hengxia Zhao, Huilin Li, et al. The effect observation of angelica four inverse soup combined with α-lipoic acid in the treatment of diabetes peripheral neuropathy.Integration of Traditional Chinese and Western Medicine Research,2014,2,6:28-29.
16. Huancong Wang, Junqiang Zhao. The effect observation of angelica four inverse soup combined with α-lipoic acid in the treatment of diabetes peripheral neuropathy. Journal of Modern Chinese and Western Medicine, 2015,8,24:2575-2577.
17. Lingmin Wu.The clinical effect observation of angelica four inverse soup decoction in the treatment of cold-coagulation blood-stasis-type diabetes peripheral neuropathy. Postgraduate Dissertation of Fujian University of Traditional Chinese Medicine,2017.05.
18. Weimi Chen, Zhilong Liu, Sujing Duan, et al.The effect of angelica four inverse soup on vibration perceptionthreshold of patients with diabetes peripheral neuropathy. Shaanxi Journal of Traditional Chinese Medicine,2016,37,6:660-661.
19. Weimi Chen, Zhilong Liu, Sujing Duan, et al.The effect of angelica four inverse soup on nerve conduction velocity and ankle brachial index of patients with diabetes peripheral neuropathy. Journal of Hunan University of Chinese Medicine,2016,7,36:62-64.
20. Xianhui Fang,Richu Liang,Peng Zhou.The effects of angelica four inverse soup on RBC-AR and Na+-K+-ATPase in the treatment of diabetes peripheral neuropathy. Guangming Journal of Chinese Medicine,2013,1,28:77-78.
21. Ping Wang,Peng Cui,Yangyang Hong.The clinical effect observation of angelica four inverse soup in the treatment of cold-coagulation blood-stasis-type diabetes peripheral neuropathy. Chinese Journal of Traditional Chinese Medicine,2017,3,3:661-664.
 Clinical Research Communications2019年1期
Clinical Research Communications2019年1期
- Clinical Research Communications的其它文章
- Clinical observation on TCM fumigation and washing for treatment of diabetic peripheral neuropathy by self-made water-washing footbath
- Xiaoaiping injection combined with cisplatin and gemcitabine for non-small cell lung cancer:a meta-analysis
- A case report of acupuncture of dysphagia caused by herpes zoster virus infection
- 18F-FDG PET/CT for Detecting Vulnerable Carotid Plaque:A Systematic Review of Literatures