
Melanotic Xp11-associated tumor of the sigmoid colon:A case report
2019-04-20 02:03:58GangWangGangGangLiShengMaoZhuBaoJiaCaiPengJieYuChengWuZhang
World Journal of Clinical Cases 2019年5期
Gang Wang,Gang-Gang Li,Sheng-Mao Zhu,Bao-Jia Cai,Peng-Jie Yu,Cheng-Wu Zhang
Abstract
Key words: Melanotic Xp11-associated tumor; Perivascular epithelioid cell tumor; Melan-A; Sigmoid colon; Case report
INTRODUCTION
Melanotic Xp11-associated tumors are rare mesenchymal-derived tumors.In 2009,Arganiet al[1]reported the clinicopathological features of a distinctive renal cell cancer(RCC) termed “melanotic Xp11 translocation renal cancer”.In 2012,LeGalloet al[2]reported the first case of primary melanotic Xp11-associated tumor in the ovary,for which the immunohistochemical markers were very similar to those of RCC.Melanotic Xp11-associated tumors can occur at all ages; children and young adults are particularly prone whereas it is rare in middle-aged and elderly individuals.The common pathological features are:(1) the pigments are visible; (2) the tumor cells are nested,have highly developed capillary vessels,are rich in cytoplasm,and can coexpress melanocyte markers HMB45 and Melan-A but not epithelial markers; and(3) there areTFE3gene rearrangement and Xp11 translocation.So far,most primary melanotic Xp11-associated tumors have been reported in the kidney,and reports of this tumor in the gastrointestinal tract are rare.Therefore,data regarding the clinical features and biologic behavior of melanotic Xp11-associated tumors are limited.Here we report the clinicopathologic features of a sigmoid colon tumor in a 25-year-old woman showing morphologic,immunohistochemical,and molecular genetic features identical to those of melanotic Xp11 translocation renal cancer,and performed a review of the published literature.
CASE PRESENTATION
Chief complaints
A 25-year-old woman presented with a 4-d history of abdominal pain,melena,and nausea that were aggravated 1 d prior to admission.She had diarrhea approximately four times a day.
History of present illness
The patient presented to a local Chinese Medicine Hospital and was diagnosed with hemorrhoids.Her condition did not improve after the medical treatment,so she presented to our hospital for further evaluation.
History of past illness
There was no obvious abnormality in the past illness.
Personal and family history
She denied any family history of related diseases.
Physical examination upon admission
No obvious positive signs were found in the abdomen.
Laboratory examinations
The laboratory findings revealed normal routine blood parameters,coagulation function,tumor markers,and biochemistry results.Blood pressure was 90/70mmHg,heart rate was 90 beats/min,and the heart rhythm was normal.Immunohistochemically,the tumor cells were strongly positive for HMB45,CD34 (vascular+),CD117,CD163,CD68,and Melan-A and negative for CK,Vimentin,S100,CK7,CK20,CD10,Dog-1,Des,CgA,SYN,LCA,EMA,smooth muscle actin (SMA),and SOX-10.Mitotic figures were approximately ≥ 2/5 per high power field,Ki-67 labeling index was approximately 2%,and there was a partially invasive boundary.The initial diagnosis was a gastrointestinal tract malignancy with perivascular epithelioid cell tumor (PEComa).However,we excluded primary melanoma and primary clear-cell sarcoma of the gastrointestinal tract.The patient was advised to have a genetic test or pathological consultation.Pathological consultation and a fluorescencein situhybridization (FISH) test were subsequently performed at Xijing Hospital,Fourth Military Medical University; immunohisto-chemistry showed that the tumor cells expressed a melanin marker and TFE3,accompanied byTFE3gene translocation(Figure 1).FISH forTFE3rearrangement showed that theTFE3gene was fractured(Figure 1).The tumor showed an abnormal signal pattern consistent with rearrangement of theTFE3locus in 52% of the cells.Taking into account all these immunohistochemistry and FISH tests,the final diagnosis was a melanotic Xp11-associated tumor.There was no intraoperative evidence of metastasis or involvement of other abdominal organs.Moreover,subsequent staging studies showed no evidence of metastatic disease.
Imaging examinations
Colonoscopy revealed a large mucosal bulge in the sigmoid colon,approximately 32cm inside the anus.The surface was rough with local erosion.The tumor was brittle on biopsy and bled easily.Computed tomography revealed thickening of the rectal wall with edema.Gastroenterography revealed a filling defect at the junction of the sigmoid and the descending colon.Sputum passed through,the local wall was stiff,and the mucosal destruction was interrupted.Barium sulfate passed through,the local wall was stiff,and the mucosal destruction was interrupted.A malignant tumor was suspected after we completed the relevant examinations.Laparoscopic-assisted resection of the large sigmoid colon mass (about 10 cm × 2.1 cm) was performed.Postoperative pathology indicated the likelihood of a PEComa.
FINAL DIAGNOSIS
Melanotic Xp11-associated tumor of the sigmoid colon.
TREATMENT
Laparoscopic-assisted resection of the large sigmoid colon.
OUTCOME AND FOLLOW-UP
She was followed by imaging studies of the chest,abdomen,and pelvis as well as colonoscopy every 3 mo.At 6 mo after the initial diagnosis,she was disease-free.
DISCUSSION
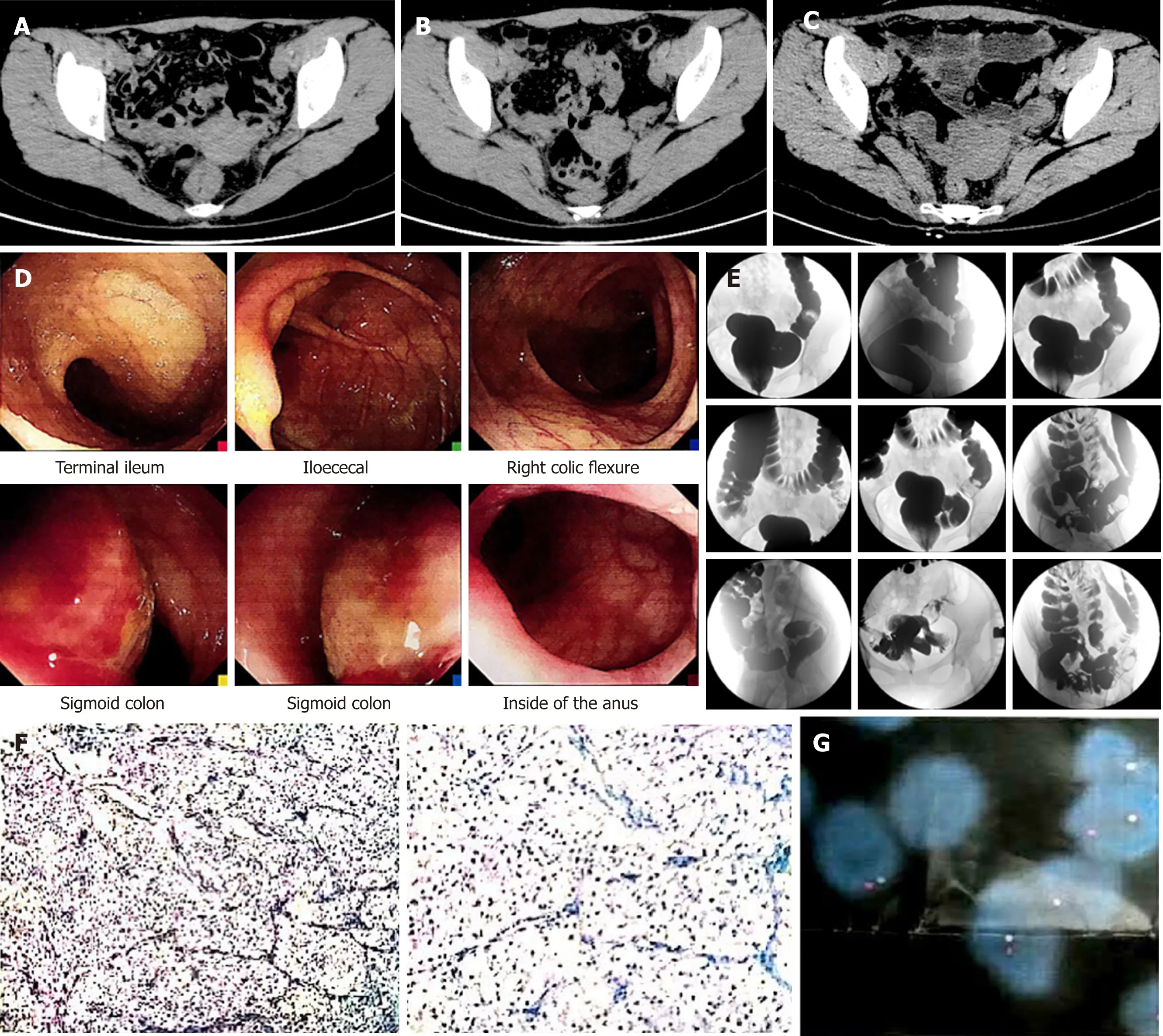
Figure 1 The examination results of the patient.
Since Arganet al[1]first reported Xp11 translocation RCC in 2009,increasing numbers of melanotic tumors have been reported.In 2012,LeGalloet al[2]first reported melanotic Xp11-associated tumor originating in the ovary.The common pathological feature are that the tumor cells are nested,have highly developed capillary vessels,and are rich in cytoplasm,and the pigments are visible,which makes it very similar to PEComa,and tumor cells can coexpress melanocyte markers HMB45 and Melan-A[3,4].Melanotic Xp11-associated tumors originating in the digestive system are rare.Therefore,most previous reports on this disease misdiagnosed it as a PEComa.So far,no relevant clinical data can predict the prognosis of these rare postoperative melanotic Xp11-associated tumors[2].Due to the fact that melanotic Xp11-associated tumors are extremely rare and their histologic features vary,a differential diagnosis to exclude other tumors is important.The differential diagnosis of melanotic Xp11-associated tumors includes various types of epithelial and mesenchymal tumors,including PEComa,malignant melanoma,clear-cell sarcoma,gastrointestinal stromal tumor (GIST),metastatic RCC,and epithelioid leiomyosarcoma.It is well known that the morphology and immunohistochemical features of these unique melanotic Xp11-associated tumors overlap with the morphologic and immunohistochemical features of PEComa.Although the distinction of melanotic Xp11-associated tumors from PEComas is difficult,we believe that the overall morphologic features of the current tumor,particularly the presence of large amounts of melanin,the absence of SMA expression,the lack of the tuberous sclerosis complex gene mutation,and the presence ofSFPQ/TFE3fusion[3,5-8],encouraged us to interpret this lesion as a melanotic Xp11-associated tumor (Table 1),thereby making it less difficult to differentiate.The detailed differences are shown in Table 1.FISH is the most commonly used method for gene detection[9].Malignant melanoma and clear-cell sarcoma have a high positive rate of S100 protein andTFE3recombination but a lack of expression of myogenic markers[10,11].Therefore,the melanin and myogenic immune markers can be used for identification.GIST is the most common tumor of the gastrointestinal mesenchymal tissue,which has a morphology very similar to that of gastrointestinal PEComa,and can also coexpress the CD117 tumor marker,which increases the difficulty in differentiation of this disease.However,GIST does not have the characteristic of expressing the melanin marker; hence,we can use the melanin marker to distinguish it[12-15].
CONCLUSION
In summary,we report the clinicopathological features of a primary tumor that is extremely rare in the sigmoid colon and review the clinicopathological characteristics of melanotic Xp11-associated tumors,compatible with the very rare tumor termed“melanotic Xp11 translocation renal cancer” in all aspects.Xp11 melanoma should be considered in the differential diagnosis of abnormal melanomas,particularly in cases involving PEComas or unusual primary melanoma tumors.Melanotic Xp11-associated tumors are a special type of tumor with a low incidence,especially for tumors originating in the gastrointestinal tract.The etiology,pathogenesis,and related biological behaviors of this disease remain unclear.Postoperative management,including adjuvant chemotherapy,has not been established yet.A further study of these particularly rare tumors is necessary to understand their biological behavior and pathogenesis.Therefore,patients with postoperative melanotic Xp11-associated tumors should be carefully followed.
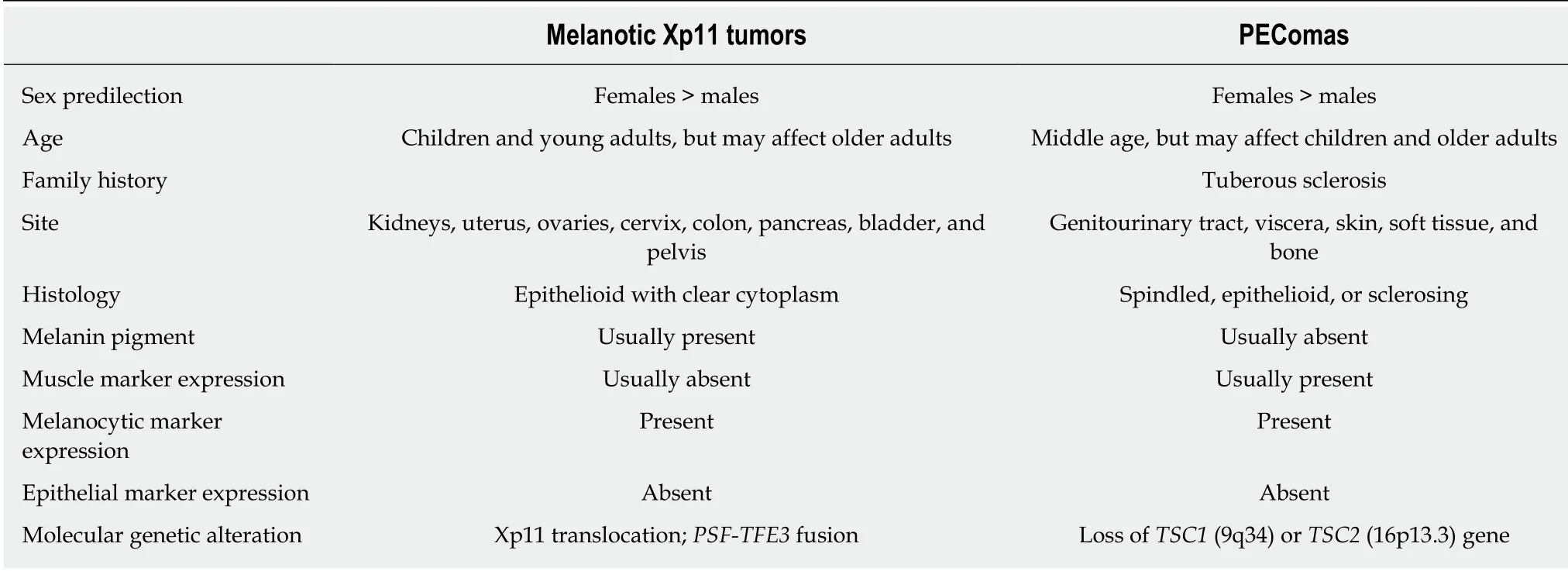
Table 1 Comparative features of melanotic Xp11 tumors and perivascular epithelioid cell tumors
 World Journal of Clinical Cases2019年5期
World Journal of Clinical Cases2019年5期
- World Journal of Clinical Cases的其它文章
- Intrauterine cystic adenomyosis:Report of two cases
- Use of tunnel endoscopy for diagnosis of obscure submucosal esophageal adenocarcinoma:A case report and review of the literature with emphasis on causes of esophageal stenosis
- Rare empty sella syndrome found after postoperative hypotension and respiratory failure:A case report
- Concomitant paraganglioma and thyroid carcinoma:A case report
- Application of computer-assisted navigation in treating congenital maxillomandibular syngnathia:A case report
- Perioperative topical ascorbic acid for the prevention of phacoemulsification-related corneal endothelial damage:Two case reports and review of literature