
Immune checkpoint inhibitor-induced colitis:A comprehensive review
2019-04-16 08:23AniruddhSomRohanMandaliyaDanaAlsaadiMahamFarshidpourAlineCharabatyNidhiMalhotraMarkMattar
World Journal of Clinical Cases 2019年4期
Aniruddh Som,Rohan Mandaliya,Dana Alsaadi,Maham Farshidpour,Aline Charabaty,Nidhi Malhotra,Mark C Mattar
Abstract
Key words: Immune checkpoint inhibitors;Immune-related adverse events;Cytotoxic Tlymphocyte-associated antigen 4;Programmed cell death protein 1;Programmed deathligand 1;Immune-mediated colitis
INTRODUCTION
Scientists have long experimented with the idea that the immune system holds the potential to fight not only infections but also malignancy.In the early 19thcentury,Busch and Fehleisen,both noted that infecting tumors with erysipelas resulted in tumor regression[1,2].Towards the late 1800s,sarcoma regression was seen after injecting tumors with heat-inactivated bacteria known as “Coley's Toxins”[3].The pivotal change in the history of immune checkpoint inhibitors(ICIs)began with the discovery of the T-cell receptor by Allison et al[4]in the early 1980s.This discovery was soon followed by the first ever reported human tumor antigen recognized by T-cells[5].A study on tumors in animal models provided proof of concept that an antibody was successful in blocking the cytotoxic T-lymphocyte antigen 4(CTLA-4)[6].Such seminal work culminated with the Food and Drug Administration(FDA)approving the first ICI for use in metastatic melanoma in 2011[7].To date there are 7 approved checkpoint inhibitors that target 3 main checkpoints,including cytotoxic T-lymphocyte associated protein 4(CTLA-4;ipilimumab and tremelimumab),programmed cell death receptor 1(PD-1;pembrolizumab and nivolumab),and programmed death ligand 1(PD-L1;atezolizumab,avelumab,and durvalumab).Indeed,ICIs have become the standard of care for a number of cancers and resulted in the awarding of the 2018 Nobel Prize in Physiology or Medicine to Allison and Honjo in recognition of their contribution to the discovery of ICIs[8].While representing a remarkable breakthrough in the treatment of several advanced malignancies,several ICI-related adverse events that affect multiple body systems(Table1)[9-14]have been recognized,including immunemediated colitis(IMC)and enteritis[9-16].The incidence of IMC ranges from 0.3% to 7%and may be associated with other immune-related adverse events(irAEs)[17].As a result,addressing GI irAEs has become a major clinical issue for physicians and patients alike.This review summarizes the current clinical information of IMC,its postulated mechanism of injury,endoscopic features,and the management strategies that are currently advocated.
Mechanism of action
The immune system has an important role in recognizing and eliminating tumors.Transformed tumor cells express tumor-associated antigens(TAAs)that are not seen on normal cells[18].These TAAs are recognized by the immune system,and T cells can be stimulated in response to cellular presentation of TAAs[19].TAAs are presented along with the major histocompatibility complex(MHC)I or II by specialized antigen-presenting cells(APCs)that bind with T-cell receptors(TCRs).Activation of T cells requires a co-stimulatory signal which includes the interaction of TCR with MHC along with the interaction of CD-28(stimulatory checkpoint expressed on T cells)with B7(CD-80)present on APCs.This leads to T-cell proliferation,cytokine secretion,changes in gene expression and metabolism[20].
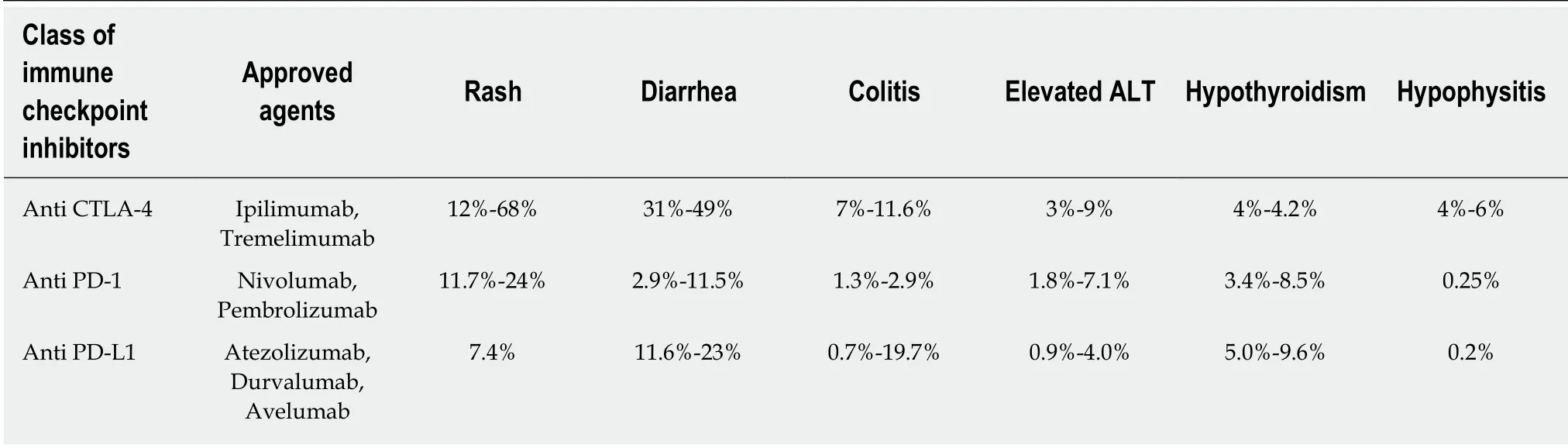
Table1 Percentage ranges of all grade immune-related common adverse events by checkpoint inhibitor class
Tumors may use immune-checkpoint pathways as a mechanism of immune resistance,principally against T cells that are specific for TAAs[21].Two well-studied immune-checkpoint receptors are CTLA-4(CD152)and programmed cell death protein 1(PD-1 or CD279).CLTA-4 is a negative regulator of T-cell-mediated antitumor responses.Expression of CTLA-4 is up-regulated upon TCR stimulation.This molecule competes with CD28 for binding to B7 on APCs,avoiding the costimulatory signal and blunting T-cell activation and proliferation[22].PD-1 is also expressed on the surface of activated T cells.The interaction between PD-1 and programmed death ligand(PD-L1 and PD-L2),expressed on APCs,leads to T-cell inactivation.Additionally,PD-1 plays an important role to limit the activity of T cells in peripheral tissues through inflammatory response to infection and to limit autoimmunity[23].
Checkpoint inhibitors are monoclonal antibodies that block these pathways.Ipilimumab was the first checkpoint inhibitor immunotherapy approved by the FDA,in March 2011,for the treatment of melanoma.Ipilimumab is a fully humanized monoclonal antibody that competitively binds to CTLA-4 more efficiently when compared to B7 while preserving CD28 signaling[24].Blockade of CTLA-4 signaling extends T-cell activation and reestablishes T-cell proliferation[25].As CTLA-4 plays a crucial role in regulating tolerance to self-antigens,CTLA-4 blockade may lead to autoimmune damage to various organ systems,resulting in irAEs[26].CTLA-4 blockade can initiate dysregulation of GI mucosal immunity which results in irAEs that comprise the esophagus,duodenum,stomach,ileum and colon[27].The various types of ICIs are described in Table1.
Mechanism of irAEs
Mechanisms of IMC and other irAEs are not fully understood;however,CTLA-4 blockade removes CTLA4-mediated protection from autoimmunity and is responsible for a large spectrum of autoimmune-side effects[28].Immune-related toxicities are mostly associated with the inflammatory reaction produced by immune system responses against specific organs and tissues[29].Immune-related T-cell activation leads to the secretion of high levels of CD4 T-helper cell cytokines and cytolytic CD8 T-cell tissue infiltration[21].Another potential mechanism for generating colitis following anti-CTLA4 antibody involves CD25+CD4+ regulatory T cells(Treg).These immunosuppressive regulatory cells constitutively express high levels of CTLA-4 and data show increased autoimmune diseases in mice lacking Treg cells[30,31].Consequently,it has been hypothesized that an antibody to CTLA4 might diminish Treg cells and induce autoimmunity[32].
The enterocolitis related to ipilimumab has features similar to graft-versus-host disease.It has been proposed that a contributing factor to enterocolitis in this setting may be intestinal microflora and bacterial antigens,representing an area of future research for prophylaxis of enterocolitis in patients treated with ipilimumab[33,34].
Clinical presentation
Diarrhea and enterocolitis lie along a clinical spectrum where diarrhea is defined as increased stool frequency,and enterocolitis is defined as abdominal pain,rectal bleeding or the presence of mucus in stools with either clinical or radiologic objective evidence of entero-colonic inflammation,as defined by the American Society of Clinical Oncology(ASCO)[35].The presence of enterocolitis increases the risk of other complications,including ileus,colonic distension,and toxic megacolon,intestinal perforation,or even death.The clinical severity of both diarrhea and colitis is graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events(Table2).Mild diarrhea(grade 1)is defined as less than 4 stools per day above baseline.Grade 2 diarrhea is defined as 4 to 6 stools per day above baseline,while grade 2 colitis is characterized by abdominal pain or blood or mucus in the stool.Severe diarrhea(grade 3)is defined as ≥ 7 stools per day above baseline,and grade 3 colitis is defined by the presence of peritoneal signs with ileus and fever consistent with bowel perforation.A grade 4 designation is distinct from grade 3,reflecting increased severity and the life-threatening nature of symptoms.
While irAEs can affect any portion of the GI tract,the lower GI tract is most commonly involved.Less commonly,the upper GI tract can be affected,manifesting as aphthous ulcers,esophagitis,and gastritis.IMC and diarrhea typically occur 5 wk-10 wk after the 2ndor 3rddoses of treatment,but they have also been documented to occur as late as 4 mo after the last dose and may even recur one to two years after discontinuation of treatment[13,36-38].
EPIDEMIOLOGY
More than two-thirds of patients who receive anti-CTLA-4 therapy develop an irAE,and one-third of patients who are treated with anti-CTLA-4 therapy experience irAEs of the gastrointestinal tract,such as aphthous ulcers,esophagitis,gastritis,and enterocolitis,which usually presents as diarrhea[39,40].The incidence of diarrhea is higher in patients receiving anti-CTLA-4 agents,such as ipilimumab,compared to patients receiving anti-PD-1/PD-L1 agents,such as nivolumab or pembrolizumab[41],with grade 3/4 diarrhea seen in 10%vs1%-2% of patients,respectively[42].
Becket al[33]showed that enterocolitis,defined by the presence of grade 3 or 4 symptoms and/or proven by biopsy,was the most common irAE associated with ipilimumab use,occurring in 21% of treated melanoma patients.Kwonet al[43]reported a 5% incidence of grade 3/4 colitis among patients with prostate cancer who were treated with ipilimumab at the dose of 10 mg/kg.Slovinet al[44]demonstrated that the incidence of grade 3/4 colitis increased from 13% to 16% with an increase in the dose of ipilimumab from 5 mg/kg to 10 mg/kg in patients with prostate cancer.Similarly,the incidence of enterocolitis in patients with renal cell carcinoma receiving higher doses of ipilimumab was 35% compared to 14% in patients receiving lower doses[33].
Overall,the risk of severe grade adverse events increased from 7% to 25% with an increase in the dose of ipilimumab from 3 mg/kg to 10 mg/kg[43].Most of the increase in adverse effects was due to an increase in the episodes of diarrhea.However,the toxicity profile would not increase if the dosage of nivolumab or pembrolizumab were increased from FDA approved doses(2 mg/kg every 3 wk)to higher doses(10 mg/kg every 2 wk or 3 wk).It may be argued that toxicities due to anti-CTLA-4 antibodies are dose-dependent whereas toxicities with anti-PD-1/anti-PD-L1 antibodies are perhaps independent of a dose-related effect[45].
Combination therapy and risk of enterocolitis
Combination therapies have so far only been approved for metastatic melanoma.Use of combined anti-CTLA4 and anti PD-1 agents results in increased frequency and severity of diarrhea and colitis than with the use of either agent alone[46-48].They can also cause rarer forms of toxicities like pancreatitis and small bowel enteritis which warrants discontinuation of ICI treatment and initiation of immunosuppressive therapy.
Risk factors for ICI enterocolitis
Gut microbiome:Baseline microbiota composition may predict ipilimumab-induced colitis.In one prospective study of 34 patients whose pre-treatment fecal composition was analyzed,an increased baseline presence ofBacteroidetesspecies was found in patients who remained free of colitis after ipilimumab treatment[49].Another study of 26 patients with metastatic melanoma treated with ipilimumab again showed that nocolitis related phylotypes were assigned to Bacteroidetes;most of the baseline colitisassociated phylotypes were related toFirmicutes[50].Compared with those whose baseline microbiota was driven by Bacteroides,patients with a baseline microbiota enriched with Faecalibacterium and Firmicutes had longer progression-free survival and overall survival.

Table2 Grading the severity of immune checkpoint inhibitor-induced colitis and diarrhea based on Common Terminology Criteria for Adverse Events grade
Autoimmune disorders:Patients with a history of autoimmune disease,are at risk for worsening of their autoimmune disease while on immune checkpoint blockade,but immune-mediated toxicities are often mild and manageable without discontinuation of treatment[51].Patients that have experienced irAEs with prior checkpoint inhibitor therapy are at risk of developing irAEs following treatment with a different class of ICI;irAE risk also increases with dual therapy[51,52].
Other risk factors:A recent series demonstrated that non-steroidal anti-inflammatory drug use was associated with an increased risk of ipilimumab-induced enterocolitis[53].Little data is available on the risk of immune-related colitis in patients with Crohn's disease and ulcerative colitis.
DIAGNOSIS
Infectious causes of diarrhea should be ruled out with the first presentation of diarrhea or abdominal pain in patients treated with ICI therapy.Stool should be sent for standard microbiological examinations,including stool ova and parasites,bacterial culture,andClostridium difficiletesting[40].ICI-induced colitis and infection can coexist,as demonstrated by two case reports of co-infection by CMV andSalmonellaspecies[54,55].Patients who are treated with antibiotics for infection may not experience complete resolution of symptoms,suggesting a concomitant ICI component to their colitis[56].
While infections are more common,gastrointestinal metastases should also be ruled out as a potential etiology of symptoms.Patients with clinical signs of peritonitis such as fever,severe abdominal tenderness,distention,and rigidity should be evaluated with abdominal CT to rule out colonic perforation,which is a rare but well-documented adverse event that can be fatal[57-59].
Endoscopic features
Colonoscopy,with an exam of the terminal ileum and biopsies of the colon and ileal mucosa,is the gold standard diagnostic test for ICI-mediated colitis in patients with persistent grade 2 or higher diarrhea.Patients with upper GI symptoms such as nausea or vomiting should also undergo EGD with biopsies.A normal appearance of the mucosa on endoscopic examination does not exclude enterocolitis,and mucosal biopsies must always be attained[33].
Some patients with immune-mediated diarrhea or colitis may demonstrate ulcerations,but others may demonstrate erosions,erythema,loss of vascular pattern,or even grossly normal appearing mucosa(Figure 1)[60].Ipilimumab-induced colitis most often involves lesions of the rectum and sigmoid,so flexible sigmoidoscopy is usually sufficient for diagnosis.A majority of patients,however,also have endoscopic lesions proximal to the sigmoid.In more extensive colitis,inflammation can be either patchy or continuous[53,61].Studies have shown no correlation between diarrheal grade or severity of abdominal pain and endoscopic appearance,but bloody stools have been correlated with higher endoscopic Mayo scores[56,62].
Histology
ICI colitis presents with an array of histologic findings ranging from focal active colitis with patchy crypt abscesses to diffuse mucosal inflammation[53,63].Biopsies most commonly demonstrate features of acute colitis such as increased cellularity of the lamina propria with mononuclear cells,intraepithelial neutrophilic infiltrates or crypt abscesses,and an increased number of apoptotic cells in crypts[56].

Figure1 Patient who experienced immune-mediated colitis 4 wk after ipilimumab therapy.
Histologic findings may precede the onset of diarrhea or colitis.One study of asymptomatic patients who underwent colonoscopy 1 wk-2 wk following ipilimumab induction demonstrated that inflammatory changes were already present prior to symptoms(which occurred 3 wk later in the majority of patients)[63].Biopsies most frequently showed focal neutrophilic cryptitis and neutrophilic infiltration in the lamina propria,and a subset of patients had excess plasma cells in the lamina propria and lymphocytic cryptitis.When a subset of these patients did eventually present with symptomatic diarrhea or colitis within 24 wk of induction,their biopsies showed more severe infiltration of the lamina propria with mixed inflammatory cells(neutrophils,lymphocytes,plasma cells,and eosinophils),neutrophilic cryptitis and crypt abscesses,as well as glandular destruction and mucosal erosions or ulcers.This study did not show a significant increase in the number of intraepithelial lymphocytes,apoptotic activity,or histologic evidence of chronicity,such as crypt architectural distortion,basal plasmacytosis,the presence of granulomas,Paneth cell metaplasia,or pyloric metaplasia.As several other studies have also shown a relative lack of chronic inflammation on histology,the pathogenesis of ICI-induced enterocolitis is generally considered distinct from that of IBD,although both diseases have similar clinical presentations.
However,the finding of chronic inflammation changes in some ICI-treated patients has caused speculation that their presence is consistent with the progression of acute inflammation or the development of IBD.More recent studies have shown that some patients do exhibit intraepithelial lymphocytes or basal lymphocytes and crypt architecture distortion,which is more consistent with findings in chronic colitis[62].One study found features of chronic colitis in three out of nine patients with endoscopic or histological inflammation on biopsies that were taken several months after the onset of enterocolitis[53].
Interestingly,one recent study demonstrated distinct immunological characteristics of colonic biopsies taken from patients with IMC and IBD that were analyzed by immunohistochemistry and flow cytometry.The lamina propria and epithelium of anti-PD-1-induced colitis was predominantly characterized by CD8+T-cells,whereas the lamina propria in anti-CTLA-4-induced colitis was predominantly characterized by CD4+T-cells and high mucosal TNFα concentrations.In IBD or anti-PD-1-induced colitis,Treg cells were predominant,whereas in anti-CTLA-4-induced colitis more conventional CD4+cells were found[63].
Similarities between IMC and IBD still persist though these differences are helpful.As histologic features may overlap,clinical factors must be utilized to differentiate these distinct clinical entities,including disease onset soon after initiation of ICI or other associated symptoms.IMC is one of the most common irAEs,but patients often exhibit other concomitant irAEs such as hepatitis,hypophysitis,and hypothyroidism;if any of these also coincide in a patient with diarrhea,ICI colitis is much more likely than IBD.
Stool or serologic markers of ICI colitis
Identification of serologic markers specific to IMC has been an important focus of research.Fecal calprotectin is a marker that has high sensitivity and specificity for intestinal inflammation.Calprotectin is a calcium-binding protein derived primarily from neutrophils and activated macrophages[64].While calprotectin can be used to distinguish inflammatory from noninflammatory diarrhea,it is not specific for ICIinduced colitis[65].Further,while fecal calprotectin can be elevated in patients receiving ipilimumab,indicating active bowel inflammation,it does not predict the onset of colitis.There are few reports regarding the use of new novel markers to diagnose IMC.In one report by Callahanat al[66]patients with melanoma treated with ipilimumab who developed colitis had higher on-treatment serum concentrations of interleukin 17 compared with those without colitis.Another study reported that an increase in the number of eosinophils from baseline after treatment was associated with the advent of irAEs[67].Whether these are predictors of who will develop colitis on treatment or just markers of active inflammation is still unclear.Plasma CRP and albumin may be helpful but again can be affected by other systemic inflammatory processes[68].ICI-induced enterocolitis is one of the most commonly occurring irAEs,but the differential diagnosis for diarrhea in ICI-treated patients should also include other irAEs that manifest as diarrhea,such as ICI-induced hyperthyroidism or celiac disease.
MANAGEMENT
Optimal management of immune-mediated enterocolitis requires early recognition and timely use of immunosuppressive agents which are chosen based on the severity of the colitis as determined by the CTCAE[69].For mild grade 1 diarrhea,defined as less than 4 stools per day above baseline,patients may continue ICI therapy with symptomatic treatment of diarrhea with loperamide and electrolyte repletion[70].For grade 2 diarrhea or colitis,defined as 4 to 6 stools per day above baseline,abdominal pain,or blood or mucus in the stool,infectious causes must be ruled out prior to initiation of immunosuppressive agents.Checkpoint inhibitor therapy should be withheld,and oral corticosteroids initiated at 0.5-1 mg/kg per day if symptoms persist for > 1 wk and tapered over 1 mo-2 mo[71].
For severe grade 3 or 4 toxicity,defined as ≥ 7 stools above baseline per day or the presence of peritoneal signs with an ileus and fever consistent with bowel perforation,checkpoint inhibitor therapy should be permanently discontinued.Patients with grade 3 or 4 toxicity are usually hospitalized for intravenous fluid resuscitation and expedited initial workup and treatment.Systemic corticosteroids are initiated at 1-2 mg/kg per day(prednisone or equivalent)once bowel perforation is excluded and Clostridium difficile infection is ruled out.
Overall,one-third to two-thirds of patients either do not respond to high-dose intravenous steroids,or have a relapse requiring an increase in the corticosteroid dosage during the course of steroid tapering[53].In a recent study of 92 patients who developed diarrhea/colitis on immunotherapy for melanoma or lung cancer,in 54(56%)episodes,patients had corticosteroid-refractory colitis[56].Recent studies suggest that the presence of colonic ulcers on endoscopic exam of patients with ipilimumabinduced colitis predict a steroid refractory course[56,61,62].One study of 92 patients with ICI-colitis requiring corticosteroid therapy found that ulcers,pancolitis,and high Mayo scores or high van der Heide scores,which assess the severity of colitis based on endoscopic features,predict the likelihood that patients may be steroid-refractory and need infliximab[56,72,73].Patients that require infliximab usually have an excellent response.If there is no improvement in symptoms within 3 d to 5 d of high-dose steroids,then immunosuppressive therapy with the anti-TNFα inhibitor infliximab is started at 5 mg/kg dosed every 2 wk until resolution of symptoms[74].There are few differences in the management guidelines established by the Society for Immunotherapy of Cancer(SITC),ASCO,and European Society of Medical Oncology(ESMO)(Table3)[10,36,75].
All of the clinical guidelines recommend permanently discontinuing ICIs for grade IV colitis.For grade III colitis,recommendations vary.SITC recommends resuming ICI once corticosteroid is tapered to ≤ 10 mg/d and the patient remains symptom-free.ASCO recommends considering permanent discontinuation of CTLA-4 agents,while PD-1 or PD-L1 agents may be restarted if the patient can recover to grade 1 or less.ESMO does not make any clear recommendations regarding resuming ICI in grade 3 diarrhea/colitis.All of the societies agree that resuming ICI may be considered in grade II diarrhea once improvement is noted.
While infliximab has been successfully used to achieve clinical resolution in many patients with ICI-induced colitis,its use may be limited in those who are refractory or those who have contraindications to anti-TNFα therapy,including patients with a history of latent tuberculosis or chronic carriers of hepatitis B virus[76-78].Historically infliximab use has notably been associated with skin cancers and with lymphomas(Hodgkin's,non-Hodgkin's,and hepatosplenic T-cell)in younger populations,butmore recent studies suggest that these associations are confounded by prior thiopurine use and by overall increased risk of malignancies in the IBD population whose use of infliximab is the most studied[79,80].One recent meta-analysis of 11702 patients with cancer history who were followed for 31258 person-years found that there was no increased risk of cancer recurrence in those exposed to anti-TNFα agents[81].For patients who do not respond to the first or second dose of infliximab,drug trough levels should be obtained to determine whether dose escalation would be beneficial such as in those who have low trough levels[82].Patients with adequate drug levels are likely primary non-responders and need to switch to a different drug class.

Table3 Management of immune checkpoint inhibitor-induced colitis and diarrhea based on Common Terminology Criteria for Adverse Events grade,as summarized by the Society for Immunotherapy of Cancer,American Society of Clinical Oncology,and EuropeanSociety of Medical Oncology

ICI:Immune checkpoint inhibitors;FBC:Full blood count;UEC:Urea,electrolytes,creatinine;LFTs:Liver function tests;CRP:C-reactive protein;TFTs:Thyroid function tests;PCR:Polymerase chain reaction;CTLA-4:Cytotoxic T-lymphocyte-associated antigen 4;PD-1:Programmed cell death protein 1;PD-L1:Programmed death-ligand 1;NYHA:New York Heart Association;CHF:Congestive heart failure.
Treatment algorithms do not currently suggest the use of any immunosuppressants other than anti-TNFα agents in the treatment of irAEs such as colitis.There are few published reports in the literature demonstrating the use of vedolizumab in the treatment of ICI-induced colitis[38,68,77,83].Vedolizumab,an antibody against the α4β7-integrin on the surface of CD4+ T cells,is approved for the treatment of inflammatory bowel diseases.Bergqvistet al[68]reported on 7 cases of steroid-dependent or steroidrefractory ICI-induced colitis successfully treated with vedolizumab,which has a uniquely gut-specific mechanism of action in that it prevents T cells from binding and homing into the inflamed bowel mucosa,which can explain its efficacy in ICImediated enterocolitis.Vedolizumab was administered with infusions of 300 mg at time-points 0 wk,2 wk,and 6 wk or until clinical and laboratory regression was observed[68].Vedolizumab's gut selectivity potentially allows minimization of the potential risk for cancer progression in patients known to have metastasis involving lymph nodes[83].Vedolizumab use is thought to mitigate the antitumor effect of ICIs to a lesser extent potentially and to have the additional benefit of not heightening the risk of secondary malignancies in an already vulnerable patient as is a potential with infliximab use.Further studies are needed to establish the role of vedolizumab in the therapeutic algorithm for ICI-induced enterocolitis.
For patients that develop a colonic perforation,with or without intra-abdominal abscess,either initially or during the course of medical treatment,emergency colectomy is indicated.A subtotal colectomy may be recommended because colonic lesions are generally extensive and segmental colonic resection is generally followed by severe inflammation of the remaining colon in the postoperative phase[53].
Colitis relapse risk associated with ICI resumption
In one recent study,four out of six patients who had an additional infusion of ipilimumab after going into enterocolitis remission relapsed[53].Among them,three patients required a new steroid course,including one patient who had a severe steroid-refractory relapse requiring infliximab infusion.Reintroduction of anti-CTLA4 in patients,who had previously experienced enterocolitis,poses a high risk of relapse and should be discussed on an individual basis.
Prevention
To date,there have been no studies that demonstrate effective measures to prevent ICI-induced colitis.One randomized,double-blind,placebo-controlled study of 115 patients receiving ipilimumab investigated the efficacy of concomitant budesonide as prophylaxis against colitis.The authors found that prophylactic steroids did not show a benefit in the tolerability of ipilimumab and did not alter the frequency of grade ≥ 2 diarrhea compared to placebo[65,84].
While rare,bowel perforation is an irAE with fatal consequences.Smithet al[85]noted that in a cohort of 22 patients treated with ipilimumab followed by high-dose IL-2 therapy,3 patients experienced perforation and subsequently required emergency laparotomy.This was found to be more significant compared to 8 perforations among 1797 patients treated with IL-2 alone and compared to 4 perforations among 198 patients treated with ipilimumab alone[85].To reduce the risk of this complication,the authors recommended that patients who have received prior anti-CTLA4 therapy,and who plan to receive treatment with IL-2,undergo diagnostic colonoscopy before initiating IL-2 to rule out chronic active colitis even in the absence of symptoms[85].
Prognosis of cancer in patients with IMC
Current theories suggest that increased irAEs predict improved response to checkpoint inhibitors and improved overall survival[62].One study of 117 patients treated with ICIs who experienced diarrhea found that diarrhea is an independent predictor of improved survival regardless of treatment requirement,and that immunosuppressive treatment for diarrhea did not significantly affect overall survival[13].
CONCLUSION
IMC is one of the most common adverse effects associated with checkpoint inhibitors.Those who experience persistent grade 2 or above diarrhea or abdominal pain should undergo infectious work up and colonoscopy with biopsies.Endoscopic features of IMC range from normal appearing mucosa to erosions,erythema,and loss of vascular pattern,to ulcerations.Symptom severity does not correspond with endoscopic appearance.While IMC shares some clinical characteristics with inflammatory bowel disease.IMC biopsies typically demonstrate findings of acute colitis such as increased cellularity of the lamina propria,intraepithelial neutrophilic infiltrates,and crypt abscesses rather than characteristics of chronic colitis such as intraepithelial or basal lymphocytes and crypt architecture distortion.Most patients with IMC respond to corticosteroids.Patients refractory to steroids are treated with short-term biologic therapy including infliximab or the gut-specific vedolizumab.Immunotherapy may be resumed in patients with IMC who respond to treatment except for those with grade 4 colitis.Multidisciplinary collaboration among gastroenterologists,oncologists and pathologists is necessary to better characterize this immune-mediated adverse event and improve upon current standard management algorithms.
 World Journal of Clinical Cases2019年4期
World Journal of Clinical Cases2019年4期
- World Journal of Clinical Cases的其它文章
- Formalin fixation on HER-2 and PD-L1 expression in gastric cancer:A pilot analysis using the same surgical specimens with different fixation times
- Nested case-control study of multiple serological indexes and Brighton pediatric early warming score in predicting death of children with sepsis
- Intestinal endometriosis:Diagnostic ambiguities and surgical outcomes
- Efficacy of 1.2 L polyethylene glycol plus ascorbic acid for bowel preparations
- Congenital analbuminemia in a patient affected by hypercholesterolemia:A case report
- Primary leiomyosarcoma of the thyroid gland with prior malignancy and radiotherapy:A case report and review of literature