
PD-L1 expression and its effect on clinical outcomes of EGFR-mutant NSCLC patients treated with EGFR-TKIs
2018-12-07 06:21:40YuchenBaiXiaoxiaChenLikunHouJunQianTaoJiangCaicunZhouMaciejCiebiadaDepartmentofGeneralandOncologicalPulmonologyUniversityClinicalHospitalNorbertBarlickiMedicalUniversityofLodzLodzPolandDepartmentofUrologyShanghaiGeneralH
Cancer Biology & Medicine 2018年4期
Yuchen Bai, Xiaoxia Chen, Likun Hou, Jun Qian, Tao Jiang, Caicun Zhou, Maciej CiebiadaDepartment of General and Oncological Pulmonology, University Clinical Hospital Norbert Barlicki, Medical University of Lodz, Lodz 0, Poland; Department of Urology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 000, China; Department of Medical Oncology; Department of Pathology, Shanghai Pulmonary Hospital & Thoracic Cancer Institute, Tongji University School of Medicine, Shanghai 00, China; Department of Medical Oncology, Suzhou Cancer Center, the Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou 1000, China
ABSTRACT Objective: Epidermal growth factor receptor (EGFR) activation was reported to upregulate programmed death-ligand 1 (PD-L1)expression in lung cancer cells and subsequently contribute to immune escape, indicating its critical role in EGFR-driven lung tumors. This study characterized PD-L1 expression in patients with surgically resected EGFR-mutant non-small cell lung cancer(NSCLC). The effect of PD-L1 expression on clinical outcomes was also investigated in advanced EGFR-mutant NSCLC treated with EGFR-tyrosine kinase inhibitors (TKIs).Methods: In total, 73 patients with surgically resected NSCLC and EGFR mutations were identified. PD-L1 expression and CD8+tumor-infiltrating lymphocyte (TIL) density were assessed by immunohistochemistry. A literature review of publications that assessed the predictive and prognostic value of PD-L1 expression in advanced EGFR-mutant NSCLC patients treated with EGFRTKIs was performed.Results: Nineteen (26.0%) patients were positive for PD-L1 expression, which was significantly associated with concomitant KRAS mutation (P = 0.020) and marginally associated with higher CD8+ TILs density (P = 0.056). Positive PD-L1 expression was associated with markedly inferior overall survival (OS) in multivariate analysis (P = 0.032). The combination of PD-L1 and CD8+TILs expression could be used to stratify the population into three groups with distinct prognoses. A meta-analysis of six publications showed that positive PD-L1 expression was not associated with OS [hazard ratio (HR) = 0.90; 95% confidence interval (CI), 0.42–1.38] or progression-free survival (HR = 1.03; 95 CI, 0.73–1.33) in advanced EGFR-mutant NSCLC patients receiving EGFR-TKIs.Conclusions: PD-L1 expression tended to correlate with CD8+ TIL expression, concomitant KRAS mutation, and poor survival in surgically resected EGFR-mutant NSCLC. PD-L1 expression was neither the predictive nor the prognostic factor in advanced EGFR-mutant NSCLC patients treated with EGFR-TKIs.
KEYWORDS Non-small cell lung cancer; EGFR mutation; PD-L1; CD8; survival
Introduction
Targeted therapy on epidermal growth factor receptor(EGFR)-activating mutations has revolutionized the treatment landscape of patients with advanced EGFR-mutant non-small cell lung cancer (NSCLC)1. Several large-scale phase 3 trials have demonstrated the superior efficacy of firstand second-generation EGFR tyrosine kinase inhibitors(TKIs) to standard platinum-based chemotherapy in the first-line setting2-4. However, almost all responders acquired drug resistance after 9–12 months (acquired resistance), and 30% of the initial cohorts showed no response to EGFR-TKIs(primary resistance)1,5-7. A series of resistance mechanisms have been associated with primary and/or acquired resistance, including Bcl-2 family member (BIM) deletion polymorphism, second site mutations, downstream or bypass signaling pathway activation, and histological transformation; however, 25%–30% of acquired resistance and half of primary resistance mechanisms remain undetermined1,7. Therefore, drug resistance is the major challenge for the application of EGFR-TKI in EGFR-mutant NSCLC. There is an urgent need to identify more effective biomarkers to better predict the efficacy of EGFR-TKIs.
Immune checkpoints are orchestrated by a set of costimulatory and co-inhibitory molecules to regulate the activation and effector functions of tumor-infiltrating lymphocytes (TILs)8. Blockade of inhibitory immune checkpoints by antibodies may release the immune inhibition of effector T cells, especially CD8+ T cells9. To date,therapeutic antibodies targeting programmed cell death 1 (PD-1) and its ligand (PD-L1) have been associated with remarkable response rates in various cancers and are another significant breakthrough in the treatment of patients with advanced NSCLC. Three PD-1/PD-L1 antibodies, including nivolumab, pembrolizumab, and atezolizumab, have been approved for second-line or subsequent treatment of advanced NSCLC for their promising anti-tumor effect compared to that of standard chemotherapy10-13.Furthermore, pembrolizumab was approved in the first-line setting for patients with PD-L1 expression ≥ 50%14,15.However, in clinical practice, Gainor et al.16reported a limited effect of PD-1/PD-L1 inhibitors in patients with EGFR-mutant NSCLC. A recent phase 2 clinical study reported a 12.2% objective response rate (ORR) to an anti-PD-L1 antibody among EGFR-mutant NSCLC patients, with at least 25% of tumor cells expressing PD-L1, compared to an ORR of 3.6% in those with PD-L1 expression < 25%17,suggesting the clinical value of PD-L1 expression in EGFR-mutant NSCLC patients treated with anti-PD-L1 antibody.However, there are limited data to characterize the PD-L1 expression in EGFR-mutant NSCLC patients. A recent preclinical study demonstrated that the expression of mutant EGFR in bronchial epithelial cells could significantly induce PD-L1 expression and that EGFR-TKIs could reduce PD-L1 expression in NSCLC cell lines with activated EGFR18,indicating a potential relationship between PD-L1 expression and EGFR mutations in NSCLC. Several groups, therefore,investigated the predictive and prognostic value of PD-L1 expression on EGFR-mutant NSCLC patients treated with EGFR-TKIs. However, their findings were paradoxical. Lin et al.19reported that PD-L1 expression was associated with a better response to EGFR-TKI and longer survival, while Tang et al.20suggested that PD-L1 expression was neither the predictive nor the prognostic factor in EGFR-mutant NSCLC patients treated with EGFR-TKIs.
Therefore, the current study aimed to characterize PD-L1 expression in patients with surgically resected EGFR-mutant NSCLC and to investigate the effect of PD-L1 expression on clinical outcomes in patients with advanced EGFR-mutant NSCLC treated with EGFR-TKIs. Because the antitumor effect of anti- PD-1/PD-L1 antibodies is mainly dependent on the proliferation and activation of CD8+ TILs8,9, we further evaluated the prognostic value of the combination of PD-L1 expression and CD8+ TIL density in surgically resected NSCLC with EGFR mutations.
Patients and methods
Patient cohort
We retrospectively identified patients who underwent surgical resection of the lung (lobectomy or pulmonectomy)due to the histologically-confirmed NSCLC, between 2011 and 2015, at Shanghai Pulmonary Hospital and our cooperative medical centers. The major patient baseline characteristics including age, sex, smoking history, histology[World Health Organization (WHO) classification]21, and stage of NSCLC at initial diagnosis were collected. Never smoker was defined as a person who has smoked fewer than 100 cigarettes during their lifetime. This study was conducted in accordance with the provisions of the Declaration of Helsinki and was approved by the ethics committee of Shanghai Pulmonary Hospital. The exclusion criteria included histologically-confirmed SCLC, stage IIIB-IV before surgery, and chemotherapy and/or radiotherapy administered before surgery. Patients who could not provide adequate samples for EGFR detection and PD-L1/CD8 staining or who disagreed with the study protocols were ineligible.
PD-L1 expression analysis
PD-L1 expression was evaluated by immunohistochemistry(IHC) as described previously22. In brief, tumor sections of formalin-fixed and paraffin-embedded specimens were treated with 3% H2O2for 10 min, blocked with 5% goat serum, and incubated with a primary anti-human PD-L1 antibody (#13684, clone E1L3N, Cell Signaling Technology,Danvers, MA, diluted 1:200). Next, a peroxidase-labeled secondary antibody (REAL EnVision Detection Reagent Peroxidase Rabbit/Mouse, DAKO, Denmark) was applied to the sections for 30 min at room temperature. PD-L1 positive/negative expression was defined using a cut-off value of 5%23-26.
CD8+ TIL analysis
A mouse anti-CD8 monoclonal antibody (M7103, clone C8144B, DAKO, Denmark) was utilized for CD8+ TIL density assessment as described previously27,28. TILs were enumerated on immunostained CD8 preparations and scored using a four-tier scale (details in supplemental file).The cut-off point for high/low CD8+ TIL expression was 5%.
EGFR and KRAS mutation detection
EGFR and KRAS mutation analyses were conducted at Shanghai Pulmonary Hospital & Thoracic Cancer Institute,Tongji University School of Medicine (Shanghai, China). The samples were tested using an Amplification Refractory Mutation System (ARMS) as previously described (Amoy Diagnostics Co., Ltd., Xiamen, China)22,29,30.
Meta-analysis
We performed a publication search of the PubMed/Medline, EMBASE, Google Scholar, Cochrane Library, and Web of Science databases through December 31, 2017, using“lung cancer” and “PD-L1” and “EGFR-TKI” and their related words. Data on the relationship between PD-L1 expression and overall survival (OS), progression-free survival (PFS), and clinicopathological characteristics in EGFR-mutant NSCLC patients treated with EGFR-TKIs were collected from publications meeting the eligibility criteria(Supplementary Table S1). The details of our methodology are described in the supplemental file.
Statistical analysis
Categorical variables were analyzed using the Chi-square or Fisher’s exact tests. Continuous variables were analyzed by analysis of variance and Tukey’s multiple comparison tests.Kaplan-Meier curves were used to assess patient survival, and log-rank tests were used to evaluate the significance of differences between two or four groups. Cox proportional hazards models were used for uni- and multivariate survival analyses to calculate the hazard ratios (HRs) and corresponding 95% confidence intervals (CIs). The OS was calculated from the date of lung cancer diagnosis to death from any cause or was censored at the last follow-up date.P-values less than 0.05 (two-sided) were considered to be significant. Meta-analysis was conducted using STATA version 12.0 (Stata Corporation, TX). All statistical analyses were performed using IBM SPSS Statistics for Windows,version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Characterization of PD-L1 expression in EGFR-mutant NSCLC
In total, 201 patients with surgically resected NSCLC were initially enrolled. After EGFR detection, 73 patients with surgically resected EGFR-mutant NSCLC were finally identified. Most (63.0%) were < 65 years old at the time of diagnosis. Forty-two (57.5%) of the patients were female and 44 (60.3%) were never-smokers. The most predominant histological type was adenocarcinoma (71 patients). Three patients (4.1%) had concomitant KRAS mutations. Nineteen patients (26.0%) had positive PD-L1 expression and 22 (30.1%) had high CD8+ TILs density. Representative images of IHC for PD-L1 expression and CD8+ TILs are shown in Supplementary Figure S1. The clinical features of the 73 patients are summarized in Table 1.
There was a significant correlation between PD-L1 expression and concomitant KRAS mutations (P = 0.020).Patients with high CD8+ TIL density were more likely to have positive PD-L1 expression, but the relationship did not reach statistical significance (P = 0.056). There were no significant differences in PD-L1 expression in terms of age(P = 0.570), gender (P = 0.297), smoking status (P = 0.429),pathologic types (adenocarcinoma vs. non-adenocarcinoma)(P = 0.973), pathologic stages (I/IIIA vs. IIIB/IV) (P = 0.591),and lymph node metastasis (P = 0.661).
Prognostic value of PD-L1 expression in surgically resected NSCLC with EGFR mutation
The median follow-up time was 25.7 months (range, 5.6–54.9 months). Univariate analysis revealed that patients with positive PD-L1 expression showed a marginally shorter OS than that in patients with negative expression (HR = 2.339,95% CI: 0.992–9.835; P = 0.057) (Table 2 and Figure 1A).High CD8+ TIL density tended to be associated with longer OS but it did not reach the statistical significance (HR =0.409, 95% CI: 0.185–1.246; P = 0.138) (Table 2 and Figure 1B). Other factors including gender, age, smoking status,lymph node metastasis, and EGFR mutant types were not associated with OS (Table 2). Multivariate analyses suggested that positive PD-L1 expression was significantly associated with a shorter OS (HR = 2.995, 95% CI: 1.097–8.178; P =0.032) (Table 2). While patients with high CD8+ TIL expression showed a longer OS than that in those with low CD8+ TIL expression, the difference was not statisticallysignificant (HR = 0.296, 95% CI: 0.080–1.103; P = 0.070)(Table 2).
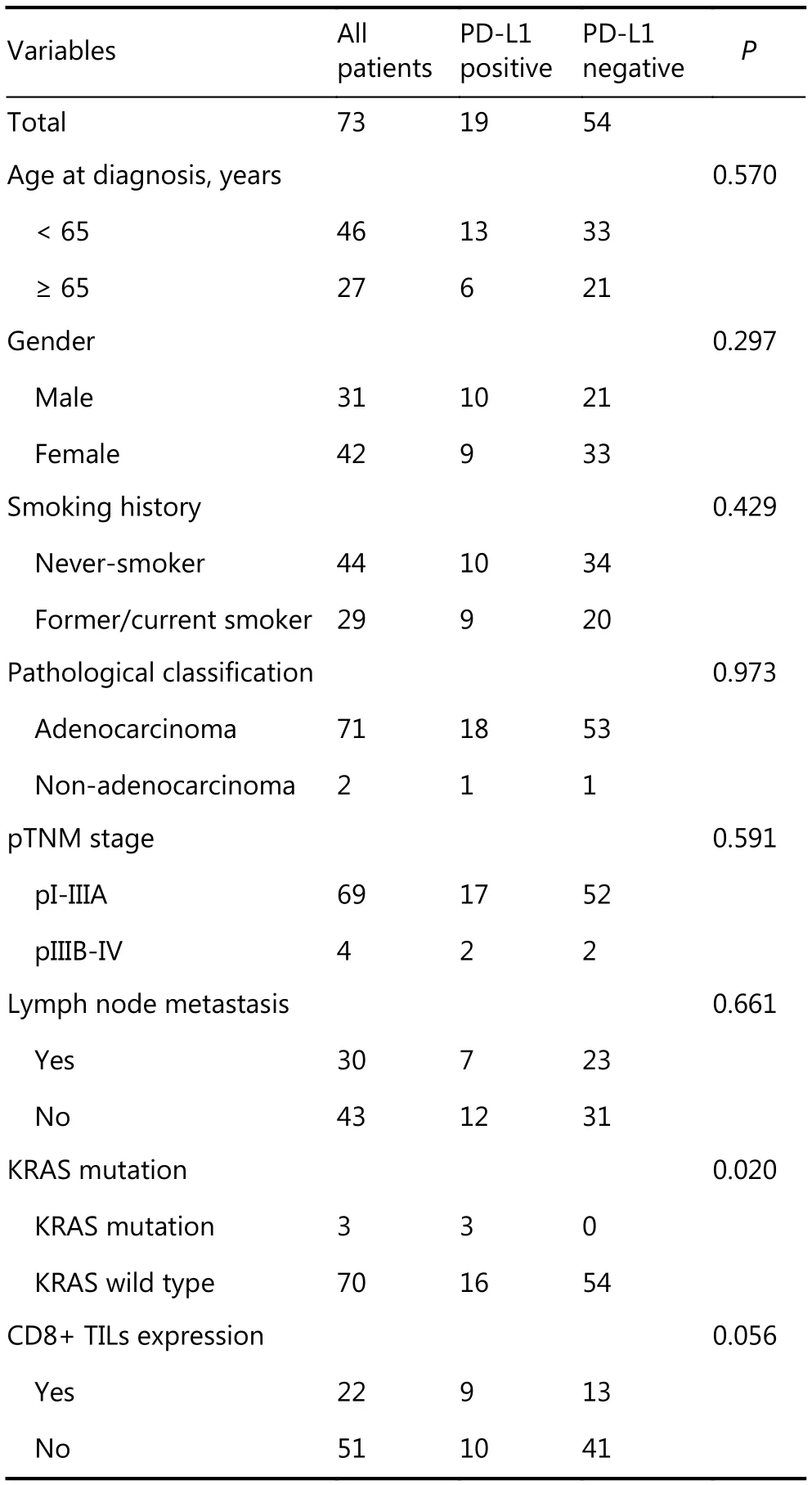
Table 1 Baseline characteristics of the study population
We further assigned the population into four groups according to PD-L1 and CD8+ TIL expression. The median OS was not reached in the PD-L1+/CD8-high and PD-L1-/CD8-high expression groups but was 29.0 months in the PD-L1+/CD8-low group and 45.0 months in the PD-L1-/CD8-low group (P = 0.056, Figure 1C). Patients with PD-L1-/high CD8+ TIL density expression had the longest OS (HR =0.196, P = 0.072), while the PD-L1+/CD8-low group had the shortest OS (HR = 3.087, P = 0.020) (Supplementary Figure S2).
Features of the studies included in the metaanalysis
A total of 192 potentially relevant studies were screened.Most of the excluded publications were reviews, comments,duplications, or studies with incomplete data. The current study assessed 648 cases from six publications19,20,31-34to investigate both the predictive and prognostic value of PD-L1 expression in advanced EGFR-mutant NSCLC patients treated with EGFR-TKIs. The main features of the eligible studies are shown in Table 3 and Supplementary Table S2.In addition, prognostic and predictive data on OS and PFS were obtained from the included studies. Figure 2 depicts a flowchart of publication inclusion.
Predictive and prognostic value of high PD-L1 expression in EGFR-mutant NSCLC treated with EGFR-TKIs
A meta-analysis was performed to evaluate the overall effect of positive PD-L1 expression in the studies containing predictive and prognostic data. The pooled results showed that positive PD-L1 expression was not correlated with OS(HR = 0.90, 95% CI: 0.42–1.38; P > 0.05; Figure 3A).Similarly, the pooled results indicated that positive PD-L1 expression was not associated with PFS (HR = 1.03, 95% CI:0.73–1.33; P > 0.05; Figure 3B). Both results showed high heterogeneity (I2= 80.3%, P < 0.001; I2= 60.8%; P = 0.013;respectively).
Publication bias
Sensitivity analysis was conducted by deleting one study at one time to assess its effect on the pooled HRs. Deletion of the study by Meniawy et al.31slightly decreased the heterogeneity in the analysis of pooled HRs of PFS and OS.No other studies influenced the pooled results. Begg’s funnel plots and Egger’s tests were used to evaluate the publication bias. The Begg’s funnel plot was symmetric, and Egger’s tests suggested no evidence of publication bias (Supplementary Figure S3).
Discussion
Emerging evidence suggested that blocking PD-1/PD-L1 showed a limited efficacy in patients with EGFR-mutant NSCLC. A preclinical study reported that EGFR activation could regulate PD-L1 expression in lung cancer, indicating a sophisticated interaction between EGFR mutations andPD-L1 expression. Improved understanding of PD-L1 expression in EGFR-mutant NSCLC would contribute to the development of more effective immunotherapy. Additionally,clarifying the predictive and prognostic value of PD-L1 expression in EGFR-mutant NSCLC patients treated with EGFR-TKIs would be helpful to precisely determine the populations who could most benefit from EGFR-TKIs therapy. To achieve these goals, the current study systematically investigated the clinicopathological features of PD-L1 expression in surgically resected EGFR-mutant NSCLC and the effect of this expression on clinical outcome patients with advanced EGFR-mutant NSCLC treated with EGFR-TKIs. Our results showed that positive PD-L1 expression was significantly correlated with concomitant KRAS mutations and seemed to be associated with high CD8+ TILs density without statistical significance, mainly due to the small sample size. Positive PD-L1 expression was associated with a significantly shorter OS, and the combination of PD-L1 and CD8+ expression could further stratify the population into three groups with distinct prognoses. Furthermore, a meta-analysis of six publications indicated that positive PD-L1 expression was neither a predictive nor a prognostic factor in advanced EGFR-mutant NSCLC patients treated with EGFR-TKIs.
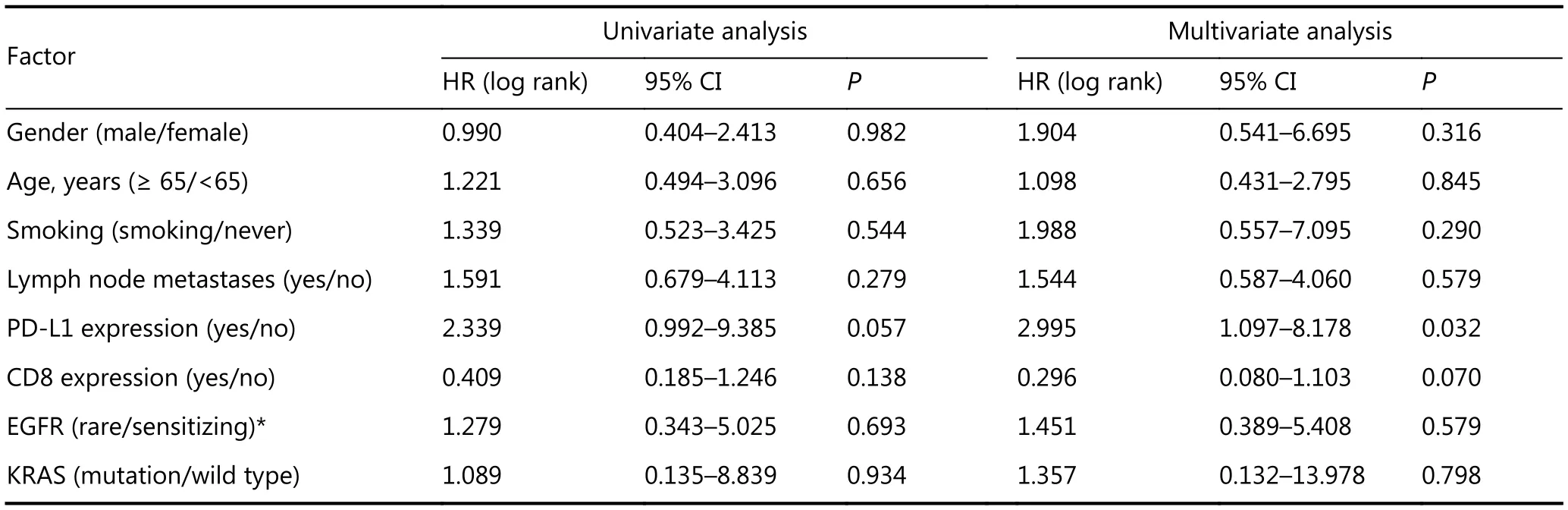
Table 2 Univariate and multivariate analyses of clinical parameters on OS in patients with EGFR muttaions.
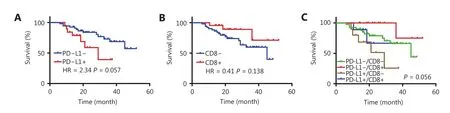
Figure 1 Prognostic value of PD-L1 expression (A) CD8 TILs expression (B) and combination of PD-L1 and CD8 TILS expression (C) in surgically resected NSCLC with EGFR mutation.
Several studies have reported a positive association between EGFR mutations and positive PD-L1 expression in completely resected NSCLC20,35-37. However, few studies have characterized PD-L1 expression in patients with EGFR-mutant NSCLC. In our study, we observed that positive PD-L1 expression was significantly correlated with concomitant KRAS mutations in patients with EGFR-mutant NSCLC. PD-L1 is frequently highly expressed in NSCLC with driver mutations, which subsequently activates key oncogenic pathways such as PI3K-AKT and RAS-MAPK. Hence, it is anticipated that more cases with high PD-L1 expression had concomitant EGFR and KRAS mutations. Notably, only three patients in the present study had concomitant EGFR and KRAS mutations. We should interpret this result with caution. In addition, positive PD-L1 expression was marginally significantly associated with high CD8+ TIL density in this population, suggesting high PD-L1 expression of CD8+ TILs in EGFR-mutant NSCLC. Further investigation of the potential role of PD-1/PD-L1 pathway in inhibiting CD8+ TIL function in EGFR-mutant NSCLC is required.

Figure 2 The flowchart of publication selection.
We further evaluated the prognostic value of PD-L1 expression in surgically resected NSCLC with EGFR mutations. As expected, positive PD-L1 expression was significantly associated with inferior OS and CD8+ TIL density was marginally correlated with a longer OS. When we combined PD-L1 expression and CD8+ TIL density, the total populations could be divided into three groups with distinct prognoses. Similarly, a large number of studies consistently reported positive PD-L1 expression to be an independent negative prognostic factor in NSCLC. In 2014, Azuma et al.35assessed the prognostic value of PD-L1 expression in 164 surgically resected NSCLC, reporting high PD-L1 expression to be significantly associated with a shorter OS independently of other factors. Two recent meta-analyses also demonstrated the prognostic value of PD-L1 expression in NSCLC.However, another meta-analysis reported no statistically significant difference between PD-L1 expression and prognosis in patients with NSCLC38,39. Of note, the driver gene mutations of the populations in these studies were unknown. Thus, high-quality studies with larger sample sizes are needed to determine the prognostic value of PD-L1 expression in NSCLC with specific driver mutations. Our finding of the prognostic value of PD-L1 expression combined with CD8+ TIL density was consistent with those of other studies28. For example, Tokito et al.28observed that a combination of a lack of PD-L1 expression and CD8+ TIL density was significantly associated with favorable survival in patients with locally advanced NSCLC receiving concurrent chemoradiotherapy, indicating that PD-L1 expression in combination with CD8+ TIL density was a useful predictive biomarker in patients with stage III NSCLC. These results suggested that the combination of PD-L1 expression and CD8+ TIL density may be useful to predict the prognosis and efficacy of immunotherapy in NSCLC.
To clarify the predictive and prognostic value of PD-L1 expression in EGFR-mutant NSCLC patients treated with EGFR-TKIs, we conducted a meta-analysis of six eligible publications. Although preclinical studies reported that EGFR activation could induce PD-L1 expression to facilitate immune escape and that EGFR-TKI could significantly down-regulate PD-L1 expression in EGFR-mutant NSCLC cells18,35, the pooled results indicated that positive PD-L1 expression was not correlated with OS or PFS in this population. Whether PD-L1 expression is a reliable biomarker for EGFR-TKI treatment in advanced EGFR-mutant NSCLC patients requires further investigation.
The current study had several limitations. First, the number of publications included in the meta-analysis was relatively small and all were retrospective studies. Second,publication bias is inevitable in this area of research. We identified several abstracts published at meetings withoutfurther detailed publications and excluded these abstracts from the meta-analysis. Third, the quality of data was heterogeneous due to a multitude of confounding factors(laboratory conditions, PD-L1 antibody, cutoff values of PD-L1 expression, etc.) that made direct comparisons difficult.

Table 3 Baseline characteristics of included studies

Figure 3 Meta-analysis to evaluate the predictive (A) and prognostic (B) value of high PD-L1 expression in EGFR-mutant NSCLC treated with EGFR-TKIs.
In conclusion, the present study showed that PD-L1 expression had a particular clinicopathological feature and was correlated with a shorter OS in patients with EGFR-mutant NSCLC. The combination of PD-L1 expression and CD8+ TIL density more precisely differentiated subpopulations with distinct prognoses after surgery. Positive PD-L1 expression was neither the predictive nor the prognostic factor in EGFR-mutant NSCLC patients treated with EGFR-TKIs. These results suggested that a meaningful graded prognostic assessment for patients with surgical EGFR-mutant NSCLC should incorporate PD-L1 and CD8+TILs and that PD-L1 expression should not be evaluated as a biomarker of EGFR-TKIs.
Acknowledgements
This study was supported in part by grants from the National Natural Science Foundation of China (Grant No. 81672286,81772467 and 81874036), “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission (Grant No. 16SG18), the Chronic Diseases Program of Shanghai Shen Kang Pharmaceutical Development Co. Ltd (Grant No. SHDC 12015314).
Conflict of interest statement
No potential conflicts of interest are disclosed.
 Cancer Biology & Medicine2018年4期
Cancer Biology & Medicine2018年4期
- Cancer Biology & Medicine的其它文章
- 2017 Chinese expert consensus on the clinical application of serum marker for thyroid cancer
- Multidisciplinary team for the diagnosis and treatment of 2 cases of primary intestinal yolk sac tumor
- Comparison of sentinel lymph node detection performances using blue dye in conjunction with indocyanine green or radioisotope in breast cancer patients: a prospective singlecenter randomized study
- Prognostic factors of refractory NSCLC patients receiving anlotinib hydrochloride as the third- or further-line treatment
- Five-CpG-based prognostic signature for predicting survival in hepatocellular carcinoma patients
- A new tumor-associated antigen prognostic scoring system for spontaneous ruptured hepatocellular carcinoma after partial hepatectomy