
Prevalence of osteoarthritis and association between smoking patterns and osteoarthritis in China: a cross-sectional study†
2018-08-01 06:22:14Originalarticle
Frontiers of Nursing 2018年2期
Original article
Qian-Qian Hea, Jun-Feng Zhanga,b,*
a School of Management, Shanxi Medical University, Taiyuan, Shanxi 030001, China
bThe Publishing house, Chinese Journal of Rheumatology, Taiyuan, Shanxi 030001, China
Abstract: Objective: The aims of this study were to estimate the prevalence of radiographic osteoarthritis (OA) and to assess the association between smoking patterns and OA prevalence in adults aged 50 years or older belonging to the Shanxi province of China.Methods: A cross-sectional study in the rural regions of the Shanxi province was conducted among 2638 Chinese adults (aged≥50 years). Demographic characteristics and behavioral information were collected through epidemiological surveys. All participants with joint pain underwent plain radiographic examination and were diagnosed by a professional orthopedist. Associations between smoking patterns and the prevalence of OA were assessed using binary logistic regression modeling.Results: Among 2638 individuals (men, 50.3% and women, 49.7%; mean age, 61.5 years) included in the analysis, 49.8% had radiographic OA and 27.5% had knee OA. The prevalence of radiographic OA was higher in women than in men (P<0.001). After adjusting for potential confounding factors, there was a nonsignificant correlation between smoking and OA prevalence in the multivariate model. Odds ratios (ORs) for all types of OA and knee OA were higher in active and passive smokers than in nonsmoking individuals after adjustments (OR 1.374; 95% confidence interval [CI] 1.049–1.802; OR 1.440; 95% CI 1.059–1.958, respectively).Conclusions: This study showed that smoking may not be an independent risk factor for OA; however, there was a positive correlation between active and passive smoking and OA.
Keywords: osteoarthritis • prevalence • smoking patterns • correlation • radiographic© Shanxi Medical Periodical Press.
1. Introduction
Osteoarthritis (OA) is the most common chronic progressive joint disease characterized by synovial tissue cartilage degeneration, inflammation, and/or thickening of the subchondral bone metabolism, leading to joint pain and stiffness and impaired physical function.1From the epidemiological point of view, with the increasing prevalence of OA and the gradual increase in life expectancy, OA has now become one of the most important causes of disability in the world.2In particular, the highest prevalence affecting a significant percentage is among elderly people.3A recent study has reported that OA affects half the population aged 65 years or older, and the prevalence in postmenopausal women is double than that in men.4Indeed, a recent meta-analysis reported a high prevalence of radiographic OA in those presenting with knee pain, with symptomatic knee OA of approximately 50%,and one-fourth of them had severe, disabling pain.5,6
Several studies have shown that OA symptoms can seriously damage the physical and mental health and physical function of the patients, limiting daily activities and reducing quality of life.7Some people who suffer from physical disabilities or need informal care lose their jobs, resulting in an economic burden on the family.8Additionally, OA has been associated with an increased risk of mortality among older people.9Since 1999, China has become an aging society; OA is a common, frequently occurring disease, and new cases are increasing every year in the elderly population.10A large-scale survey conducted in China has shown that the prevalence of OA in the knee, hand, and cervical and lumbar spines in adults aged >40 years is as high as 46.3%.11
According to statistics, as of 2015, the current number of cases in China has risen to 120 million. At the same time, the prevalence rate in women is higher than that in men, and the age of onset is younger in women than in men12; the incidence of knee OA increases sharply in women post retirement.11,13A French study showed that the total prevalence of OA was about 15% and that in patients >60 years old, it was 50%.14,15Among participants aged >45 years in the Framingham study, the prevalence of knee OA was 19.2%, and the prevalence increased to 43.7% in people aged >80 years.16According to data from the Dutch Institute for Public Health,the prevalence of knee OA in men aged 55 years or older was 15.6% and that in women was almost twice as high.17There is a wide gap in OA prevalence rates in different regions, which may be due to differences in race, culture, lifestyle, and risk factors of OA.
A number of surveys have investigated risk factors for OA and reported factors such as age, sex, occupation, weight status, sports, and recreational activities as being important in the progression of OA.18There is some limited evidence to suggest that mental health issues, heart disease, and hysterectomy may also be related to OA occurrence and development.6,19However, smoking as a risk factor for OA has always been controversial. Smoking is a risk factor for a variety of diseases, including diabetes, cancer, and cardiovascular disease,6,20and is also related to chronic pain, back pain, and rheumatoid arthritis (RA). However, a large sample size study is required to demonstrate a correlation between smoking and OA.21,22Amin et al. conducted a study on natural history, over a period of 30 months,in patients with knee OA symptoms and found that smoking men suffered from more severe cartilage damage and more severe knee pain than nonsmokers.23In addition, Ding et al. reported that smoking caused knee cartilage loss and defective development.24Contrary to this, Leung et al. showed through a prospective cohort study of 63257 participants, aged between 45 and 74 years, that smoking was a protective factor for knee arthroplasty following total knee arthroplasty.25The USA’s Health and Nutrition Examination Survey showed that knee OA was negatively correlated with the risk of smoking.26At the same time, the Framingham population-based prospective study also concluded that smokers had a significantly lower risk of incident radiographic knee OA.27Furthermore, smoking as a depressant in OA incidence was only observed in active smokers and not in passive smokers or in active and passive smokers. Therefore, this study explored the occurrence of OA in several different statuses of smoking. Of course,there are a couple of limitations, such as the diagnostic criteria of OA and smoking behavior classification are different by study and analyses were not conducted for associations between smoking habits (smoking amount,period, and pack-years) and OA prevalence. In addition, only a few studies have explored the precise relationship between passive smoking, active and passive smoking, and the prevalence of OA.
The main purpose of this study was to investigate the relationship between smoking patterns and the prevalence of OA in elderly people aged 50 years or older (nonsmoking, active smoking, passive smoking,and active and passive smoking) using the data of the Shanxi province.
2. Methods
2.1. Data sources
A total of 2638 participants aged 50 years or older were selected for this cross-sectional study, based on their characteristics and smoking status assessment. Participants were selected according to the following inclusion criteria: (1) aged 50 years or older; (2) all baseline data were available, including age, sex, and body mass index(BMI); and (3) data on usability of living habits, such as ventilation, forms of heating, and alcohol consumption,were available. The epidemiological investigation was conducted in the Shanxi province.3,28The study was approved by the research ethics boards at Shanxi Medical University. All data were collected directly from the participants. Participation was completely voluntary.
2.2. Osteoarthritis
All patients had symptoms of joint pain and agreed to undergo plain radiographic examination and diagnosis.Two orthopedists, without knowing participants’ clinical symptoms, independently evaluated and graded all radiographs using the Kellgren–Lawrence scale. When diagnosis using the radiographic film was ambiguous,the final diagnosis was made after discussion. If the score of at least one joint was 2 or higher, the participant was diagnosed with radiographic OA.28
2.3. Smoking status
We classified subjects on the basis of smoking behavior as nonsmokers, active smokers, passive smokers, and active and passive smokers. Nonsmokers were identified as those who never smoked or smoked less than five packs of cigarettes per year.Active smokers, namely self-smokers, were those who smoked more than five packs of cigarettes or those who smoked at least one pack of cigarettes in the previous month. People who have never smoked or who have smoked fewer than five packs of cigarettes as of the date of the survey are often exposed to indirect smoke at home or at work; therefore, they were classified as passive smokers. Smokers who smoked regularly and were often exposed to passive smoking at home or at work were classified as active and passive smokers.
2.4. Covariates
Potential covariates included age, BMI, waist circumference, hip circumference, sex, education background,occupation, ventilation, forms of heating, alcohol consumption, and dietary habits preference.
2.5. Statistical analysis
The prevalence of OA was obtained according to the acquired data to determine characteristics on the basis of age categories and OA classification. Analysis of variance was used to compare continuous variables between the groups, and chisquared tests analyzed the differences in categorical variables among the groups. Mean (M) and standard deviation (SD) and frequency and percentage (%)were used for continuous variables and categorical variables, respectively. Binary logistic regression analysis was used to adjust for covariates, calculate odds ratios (ORs) and 95% confidence intervals(CIs), and assess the association between smokingrelated status and OA. Statistical analysis was performed using the Stata 14.0 software, andP<0.05 was regarded as statistically significant.
3. Results
3.1. Study participants
Of the 2638 subjects who participated in the crosssectional survey, 50.3% were men. The subjects’age ranged between 50 and 90 years, with an average age of 61.5 years (standard deviation[SD] 8.6 years). Mean BMI was 23.9 kg/m2(SD 3.3 kg/m2).
3.2. Prevalence of OA
The prevalence of OA in the Shanxi province of China in subjects aged 50 years or older was 49.8%(n=1315), with a higher prevalence in women than in men (54.2% vs. 45.5%, respectively) (χ2=20.05,P<0.001). In all types of OA, knee OA was the most common, accounting for 27.5% (Figure 1). The prevalence of OA by age group was as follows: 39.0% in men in their 50s, 41.6% in men in their 60s, 42.4%in men in their 70s, and 42.6% in men in their 80s and 41.3% in women in their 50s, 46.1% in women in their 60s, 53.5% in women in their 70s, and 62.0%in women in their 80s, showing a sharp increase in prevalence in women of older age. The prevalence in men and women among all age groups was statistically significant, and women had a higher prevalence rate than men (P<0.05) (Figure 2).
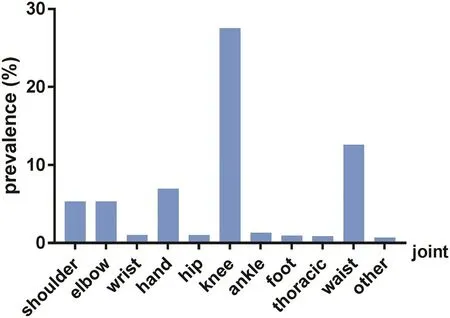
Figure 1. The distribution type of OA in Chinese adults aged 50 years or older.
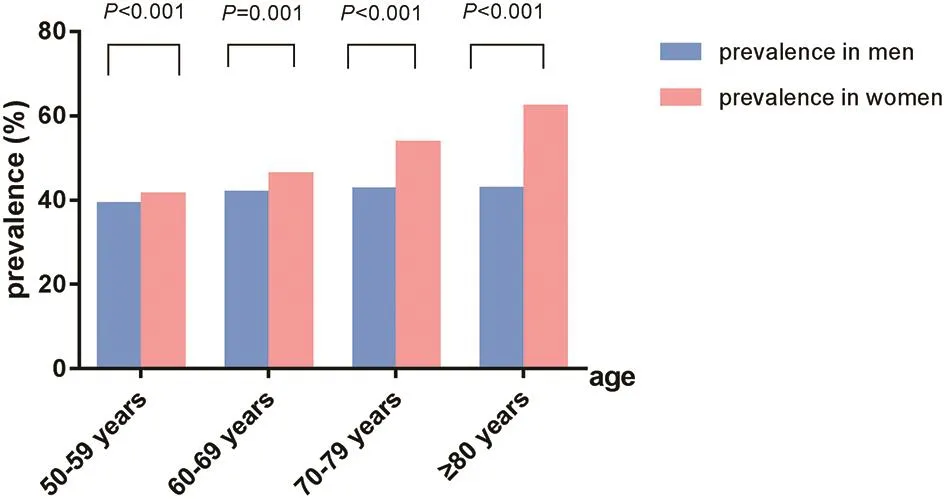
Figure 2. Prevalence of OA in Chinese adults aged 50 years or older classified by age.
3.3. Characteristics by smoking status and risk
The demographic and lifestyle characteristics of the subjects are summarized in Table 1. All factors,including age, BMI, waist and hip circumferences,sex, education background, occupation, home/residency ventilation, forms of heating, and alcohol consumption, showed significant differences, except dietary habits in nonsmokers, active smokers, passive smokers, and active and passive smokers. Compared with the other groups, the number or ratio of the nonsmoking group was relatively high in terms of demographic and lifestyle characteristics data. In addition to age and alcohol consumption, the number of demographic and lifestyle characteristics ofthe active smoking group was the lowest of the four groups.
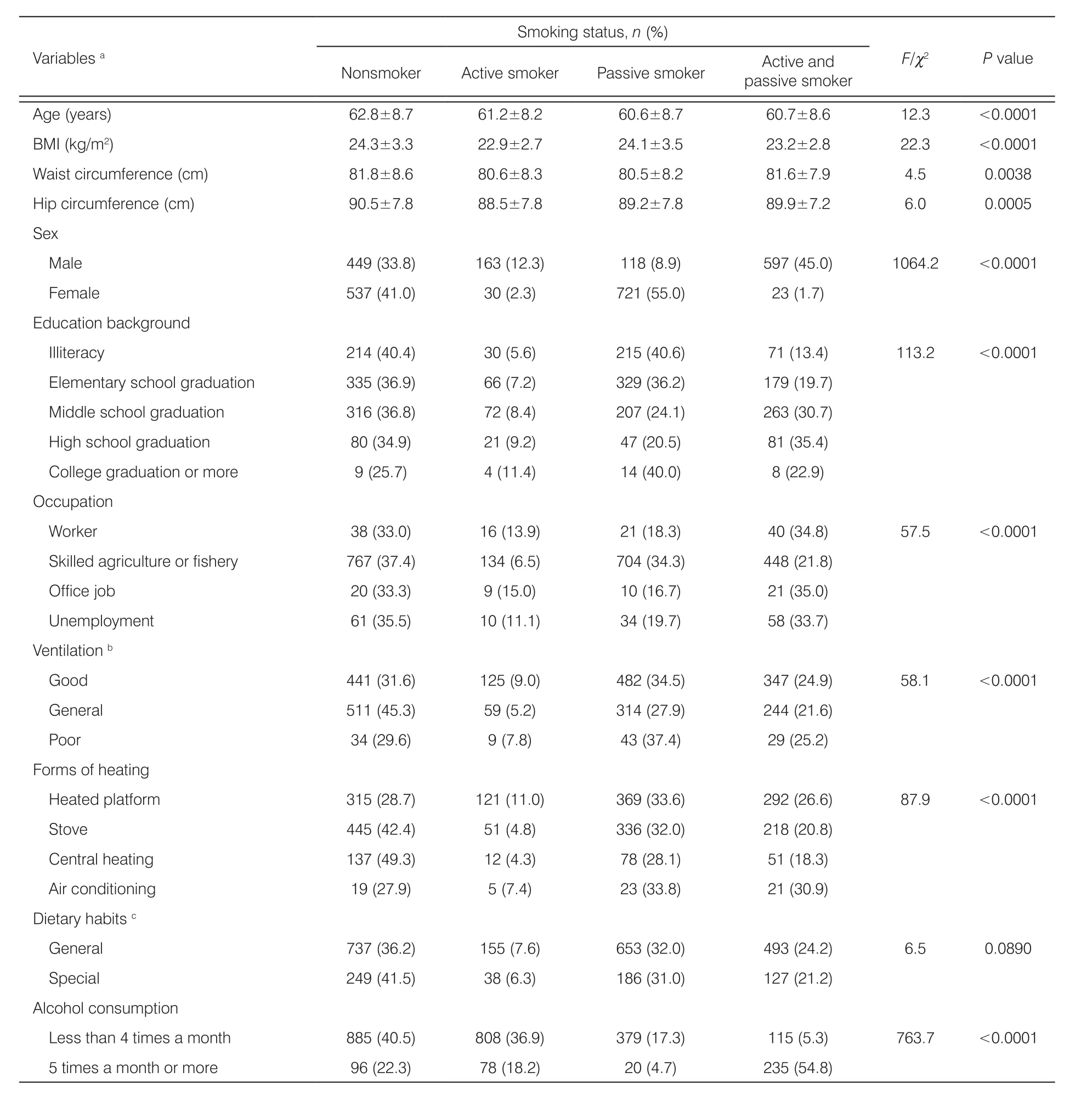
Table 1. Characteristics of Chinese adults aged 50 years or older by smoking status (n=2638).
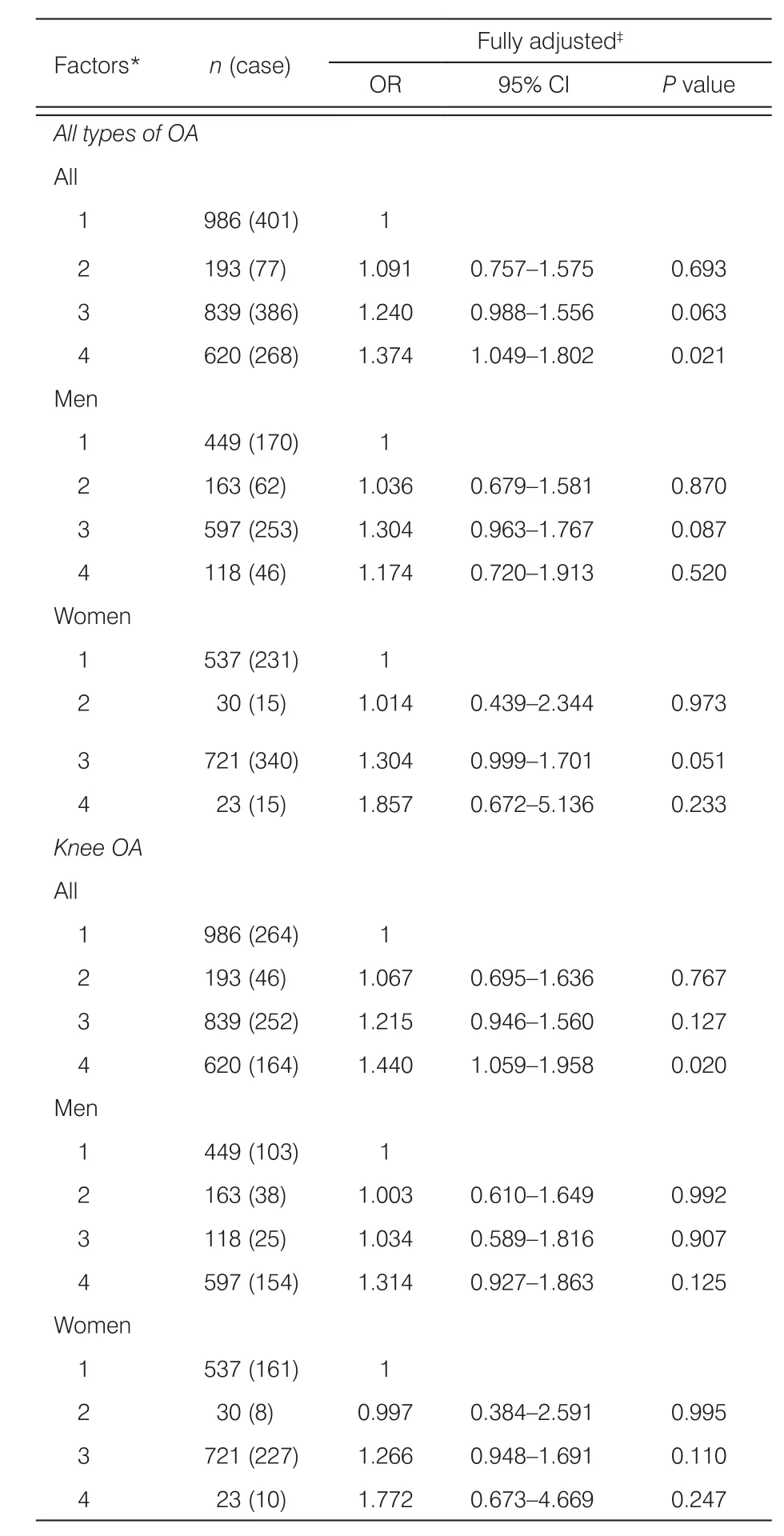
Table 2. Associations between smoking status and OA in Chinese adults aged 50 years or older.
Results of binary logistic regression modeling for all types of OA and knee OA are presented in Table 2.Within the overall sample, active and passive smoking was significantly associated with the prevalence of OA (OR 1.374; 95% CI: 1.049–1.802;P=0.021).The prevalence of knee OA was slightly higher among subjects who were both active and passive smokers compared with non-smokers (OR: 1.440; 95%CI: 1.059–1.958;P=0.020). There were no signi ficant differences in the prevalence of all patterns of OA and knee OA with smoking behaviors in all other analyses. The three different smoking statuses between men and women were not associated with OA or knee OA.
4. Discussion
The present study used baseline data from a crosssectional survey. The primary purposes of this study were to evaluate the prevalence of OA in people aged 50 years or older in the Shanxi province and to identify its association with each smoking behavior. As it is well known, OA may involve any joint, usually affecting the knees, hips, hands, feet, and facet joints. In this study,knee OA was reported in 27.5% of participants, while the overall prevalence of OA was reported in 49.8% of participants (Figure 1). Knee OA was, therefore, the most common form of OA, and this is consistent with other studies.3,8,11,19,23
The prevalence of OA and knee OA was higher in the studies of the Shanxi province of China than estimates from the Framingham OA study or other studies.14-16,29A knee OA study by Haq and Davatchi in the Community Oriented Program for Control of Rheumatic Disorders (COPCORD) studies showed that the prevalence of knee OA within rural areas of Iran is ten times higher than that within urban areas.30Part of the reason for this difference may be individual differences, material conditions, and the socioeconomic environment.This research mainly concentrated on rural regions of the Shanxi province, resulting in prevalence of OA relatively higher than the global average.
Similar to other studies, our results showed that the prevalence of OA in women was greater than in men across all age groups between the ages of 50 and 90 years (Figure 2). In the study by Srikanth et al., it is clear that the incidence of knee, hip, and hand OA in women was higher than that in men, and OA in women increased significantly after menopause.16,31Meanwhile, prevalence data from the Framingham study showed that both symptom-related data and radiographic data were higher in women than in men aged between 63 and 75 years.32,33In view of this phenomenon, it has been suggested that hormones may play an important role in the progression of OA; however,this has yet to be confirmed through clinical and epidemiological studies.34
Although it is well known that smoking has been associated with an increased risk of several diseases,such as diabetes, cancer, cardiovascular diseases,respiratory diseases, stroke, RA, and musculoskeletal diseases, so far reports of the consequences of smoking on OA are conflicting.21,35This study showed that there was no significant association between active smoking and nonsmoking in both knee OA and all types of OA, and the prevalence of OA and smoking behavior were not significantly different between sexes(Table 2). Active smokers were leaner, and residual confounding from the higher BMI among the nonsmokers could lead to no association observed in the study.However, the study of the effects of smoking on knee OA in the Framingham study showed that even adjusting for weight or BMI did not change the conclusion that smoking was harmless in terms of OA.23Several cross-sectional and longitudinal studies have confirmed that smoking seemed to decrease the risk of OA or showed no correlation.25,27,36-38A study showed that when nicotine concentration is 25–100 ng/ml, the mRNA and protein expression of type II collagen in chondrocytes of the articular cartilage increase signi ficantly and the proliferation of cells increases.39Some researchers have suggested that this may be related to smoking and reduced physical activity. Lastly, the effects of smoking may differ for incident and prevalent knee OA. When cartilage damage is caused by other mechanisms, the further study of the harmful effects of smoking on articular cartilage may result in falsepositive results. According to a study by Schouten et al., the risk of knee OA in smokers did not increase during 12 years of follow-up.40The latest research on Chinese people aged 45–74 years in Singapore has shown no difference in total joint replacement between active smokers and nonsmokers.25
Our analysis of smoking and OA showed sex differences that were not significant (Table 2). It is well known that OA is the most common cause of disability in the elderly, while women usually suffer from a higher prevalence of cartilage dysplasia, menopausal cartilage damage, and cartilage loss.41A recent meta-analysis showed that differences in smoking patterns between sexes were not related to the occurrence of knee OA.42The present study showed that smoking differences between men and women were not a risk factor for OA considering four different smoking patterns, which was consistent with the results of recent studies.
The smoke inhaled by indirect smokers contains more toxic and harmful substances because they inhale smoke not filtered by cigarette filters.43According to relevant reports, nonsmokers exposed often to secondhand smoke will be at an increased risk of bronchitis,asthma, pneumonia, otitis media, macular degeneration,neurological disorders, and other related diseases.43,44At present, reports of the relationship between passive smoking and the prevalence of OA are highly rare. In the present study, multivariate logistic regression analysis performed after adjustment for a series of factors,including age, BMI, waist and hip circumference, sex,education background, occupation, ventilation, heating, and alcohol consumption, revealed a nonsignificant association between passive smoking and OA (Table 2).However, active and passive smoking has been shown to be a risk factor for OA (Table 2). Although in the study by Kang et al., the unadjusted results partly showed that passive smoking in males was negatively correlated with OA compared to nonsmoking.6This finding is consistent with the results regarding passive smoking and OA after adjusting for all covariates.6For all types of OA or knee OA, with status of active and passive smoking,the values were OR>1 andP<0.05. There was no statistical significance when studying active smokers and passive smokers separately. However, when studying active and passive smokers, this combined situation was confirmed as a risk factor for OA. We can further speculate that this may be related to the duration of exposure, the total amount of smoking, and other factors. Since our findings may be due to the small sample size in this cross-sectional observation, these results need cautious explanation. Further studies on the relationship between smoking and OA using larger samples of different smoking statuses are required to draw more definitive conclusions.
Our study has several strengths. The wide range of people in this study can represents middle-aged and elderly people in the northwest of China. The Shanxi COPCORD study represents the middle-aged and elderly people in the northwest of China. We determined the final participants through rigorous multistage sampling procedures and conducted strict quality control of the survey. Therefore, this study can objectively describe the prevalence of OA in northwest China according to social, economic, and geographical location factors. In addition, considering the confounding effects of smoking and OA prevalence, we made targeted corrections to improve the accuracy of the statistical analysis. Our findings will contribute to the development of disease prevention and health promotion strategies and help to elucidate the potential etiology of radiographic OA in Chinese patients.
This study has some limitations. A major limitation is that only associations between smoking and OA prevalence could be drawn due to the cross-sectional design.Another limitation is that the participants were aged 50 years or older and were often accompanied by other diseases with intake of a large number of drugs, including those for treatment of many other diseases; this would have affected the prevalence of OA and analysis of the influencing factors. Furthermore, there were no data concerning activities of participants, and correlation results were limited.
5. Conclusions
Using data from the COPCORD study, we observed that the prevalence of radiographic knee OA in the Shanxi province of China was high. The prevalence of OA increased with age and was higher in women of all ages than in men. Larger cohort studies involving different smoking statuses are needed to explore the relationship between smoking and OA development.
Conflicts of interest
All contributing authors declare no conflicts of interest.
- Frontiers of Nursing的其它文章
- Preoperative nutrition and postoperative liver function: a correlation study of pediatric living donor liver transplantation†
- Characteristics of and management strategies for 54 suicidal inpatients in a general hospital†
- Visualization analysis of the study of fund-sponsored clinical nursing papers†
- A systematic review of the effectiveness of clinical nurse specialist interventions in patients with chronic obstructive pulmonary disease (COPD)
- The status quo and influence of self-management behaviors in convalescent stroke patients†
- Development and application of a closed-loop medication administration system in University of Hongkong-Shenzhen Hospital†