
Clinical observation on electroacupuncture plus hydro-acupuncture for low back pain caused by compression fractures
2018-06-28 09:27:56YangFengxiang杨凤翔ZhouFang周芳WangChengxiu王成秀GuoLihong郭俐宏
Yang Feng-xiang (杨凤翔), Zhou Fang (周芳), Wang Cheng-xiu (王成秀), Guo Li-hong (郭俐宏)
1 Department of Rehabilitation Center, Taihe Hospital, Hubei University of Medicine, Shiyan 442000, China
2 Shiyan City Hospital of Hubei Province, Shiyan 442000, China
Elderly vertebral compression fractures are mostly caused by osteoporosis. These fractures often cause significant pain in thoracolumbar vertebrae, deep in the lower back muscles, or on one or both sides of the posterior superior iliac spine[1]. Osteoporosis is the underlying cause of the disease. Due to the decrease inbone mass, bone microstructure destruction, and bone fragility, osteoporosis is clinically characterized by shortened height, limited mobility, kyphosis, and low back pain. In severe case, a fracture may occur. In addition to surgical treatment, acupuncture and hydro-acupuncture are effective for the treatment of osteoporosis[2-4].
Sinomenine, an anti-rheumatic drug, has the effect of dispelling wind and dampness, activating blood circulation and meridians, and promoting diuresis to eliminate swelling. There is definite effect of sinomenine hydrochloride injection and electroacupuncture (EA) at Jiaji (EX-B 2) points on low back pain[5-6]. In order to improve the therapeutic effect, we used the EA and sinomenine hydro-acupuncture at Jiaji(EX-B 2) points to treat low back pain caused by compression fractures and report as follows.
1 Clinical Materials
1.1 Diagnostic criteria
Referring toChinese Experts’ Consensus for Osteoporosis Diagnostic Criteria(third draft, 2014 edition) to establish the diagnostic criteria for this study[7]: middle-aged and elderly people, complaining of pain in the buttocks, lumbosacral region, lower back,etc., for more than 3 months, severe cases with kyphosis; a history of minor trauma, CT or MRI examinations showing the thoracolumbar osteoporotic vertebral compression fractures caused by trauma, or spinal deformity; bone mineral density decreased more than two standard deviations to mean (M-2SD).
1.2 Inclusion criteria
Meeting the above diagnostic criteria; aged 60 to 80 years old, gender not limited; willing to participate and signed informed consent.
1.3 Exclusion criteria
Those who did not sign informed consent; suffering from multiple systemic organic diseases, spinal infections, or pathological fractures; receiving other treatments that affect the present study; followed by other severe concurrences, symptoms, adverse reactions or worsening of their condition during the study period; pregnant or lactating women, mental disorder patients; patients who failed to complete treatment due to poor compliance; bone mineral density test showed osteoporosis, and CT scan showed no compression or compression fractures not exceeding 1/4 of the vertebral body.
1.4 Statistical method
The SPSS version 17.0 software was used for statistical analysis. The measurement data were tested for normal distribution and homogeneity of variance.Normally distributed data were expressed as mean ±standard deviation (x±s). Pairedt-test was used for comparison within the group, and independent samplet-test was used for comparison between groups; the correctiont-test was used when variance was not uniform. The rates were compared using Chi-square test.The difference was statistically significant atP<0.05.
1.5 General data
The subjects of this study were selected from hospitalized aged patients with compression fractures and low back pain in the Department of Rehabilitation Center of Taihe Hospital, Hubei University of Medicine between January 2016 and April 2017. A total of 95 patients were included. They were randomly divided into an EA group (48 cases) and an observation group(47 cases). There were no significant differences in gender, age, and duration of disease between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).
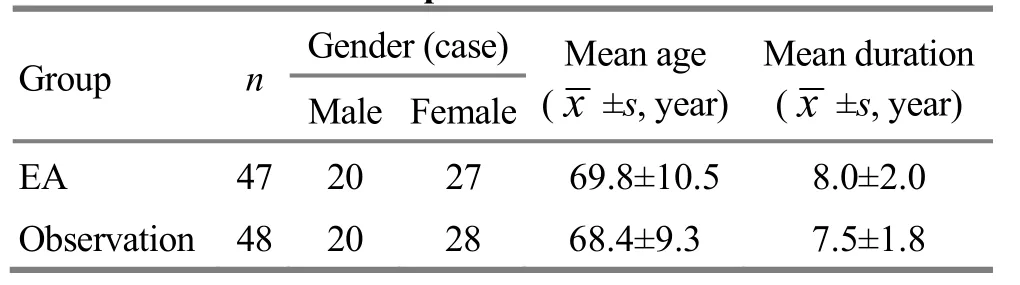
Table 1. General data comparison
2 Treatment Methods
Patients in both groups received the same basic treatment: intravenous infusion of calcitonin injection(China Food and Drug Administration approval number:H20040338, Shandong Lüye Pharmaceutical Co., Ltd.,China), 20 μg daily, every other day, 10 infusions; oral calcium carbonate D3 tablets (China Food and Drug Administration approval number: H10950029, Jiangsu Wyeth Pharmaceutical Co., Ltd., China), 1 tablet at a time, once daily; oral vitamin D (China Food and Drug Administration approval number: H20113033, Qingdao Shuangjing Pharmaceutical Co., Ltd., China),1-2 capsules/time, once a day.
2.1 EA group
In addition to the above basic treatment, patients in the EA group also received EA at Jiaji (EX-B 2) points.
Acupoints: Jiaji (EX-B 2) points (below the spinous process of lumbar spine and 0.5 cun away) on both sides of the spine[8].
Methods:Took 3 to 6 pairs of acupoints each time according to the condition. Disposable needles of 0.30 mm in diameter and 60 mm in length were used.The needle tip was directed toward the spine and pierced 15 to 30 mm at a 75° angle into the skin. After qi arrived, needles were connected to the G6805-2A instrument with sparse-dense wave and 10 Hz. The stimulation intensity was within patient’s tolerance.Each stimulation lasted for 30 min, once a day, 6 times per week, for 3 weeks. During the treatment, the patient was told to reduce activity.
2.2 Observation group
The observation group received the same basic treatment and EA at Jiaji (EX-B 2) points as the EA group.In addition, the observation group received a treatment of sinomenine hydrochloride injection at Jiaji (EX-B 2)points.
Points: Five to ten tender points on both sides of the spine.
Methods:After routine disinfection, 2-4 mL sinomenine hydrochloride injection (China Food and Drug Administration approval number: Z43020279,Hunan Zhengqing Pharmaceutical Group Co., Ltd., China,2 mL, 50 mg) was drawn and the needle was perpendicularly inserted into the tender points 1-2 cm to inject 0.5 mL (a total of no more than 4 mL a day).The above points were injected every other day for a total of 10 injections.
3 Observation on Results
There was no dropout case in the two groups during this study.
3.1 Observation items
3.1.1 Laboratory indicators
Venous blood was taken from the two groups before and on the 21st day of treatment. Enzyme-linked immunosorbent assay (ELISA) was used to detect osteoprotegerin (OPG) and interleukin-1β (IL-1β)contents in peripheral blood.
3.1.2 Low back pain dysfunction degree
Oswestry disability index (ODI) was used to evaluate the degree of dysfunction caused by the subjective low back pain before treatment and on the 21st day of treatment. The ODI scale has 50 points, including 10 questions about activity, pain, walking, lifting, standing,sexual function, sitting, sleeping, and traveling. Each question is set up with 6 options corresponding to 0-5 points. Patients filled the ODI scale by themselves and the ODI score was calculated. The higher the ODI score,the severer the dysfunction.
3.1.3 Pain intensity
The visual analog scale (VAS) was used to assess pain intensity before treatment and on the 21st day of treatment. A special ruler with two ends marked with 0 and 10 was used for evaluation. 0 was marked on one end, indicating no pain; 1-3 was classified as mild pain;4-7 for moderate pain; 8-9 for severe pain; and 10 for unbearable severe pain. Patients were asked to fill in VAS scores based on subjective pain. The higher the VAS score, the severer the pain.
3.2 Criteria of therapeutic effect
The criteria of therapeutic effect were developed with referring to the literature[9].
Cured: The X-ray examination showed fracture healing, the patient's clinical symptoms disappeared,and the spinal function was completely restored.
Markedly effective: Low back pain almost disappeared, X-ray examination showed fracture healing,and the appearance of the vertebral body improved.
Improvement: Low back pain was significantly reduced, X-ray examination showed fracture healing,and the appearance of the vertebral body improved,but local deformities were still present.
Failure: Low back pain was mildly or not relieved, an obvious local deformity and the patient's spinal dysfunction did not improve.
3.3 Results
3.3.1 Clinical efficacy comparison
After 21 d of treatment, the cured and markedly effective rate was higher in the observation group than that in the EA group with a statistically significant difference (P<0.05), suggesting that the observation group was superior to the EA group; the difference in the total effective rate between the two groups was not statistically significant (P>0.05), (Table 2).

Table 2. Efficacy comparison (case)
3.3.2 Comparison of OPG and IL-1β contents
There were no significant differences in the levels of OPG and IL-1β between the two groups before treatment (allP>0.05). After 21 d of treatment, the content of IL-1β in the EA group significantly decreased(P<0.05). The level of OPG increased, but the difference was not statistically significant (P>0.05). The content of IL-1β in the observation group was significantly lower than that before treatment, and the OPG content significantly increased. There were significant intragroup differences in the observation group after treatment (bothP<0.05), and the between-group differences were statistically significant (bothP<0.01),(Table 3).
3.3.3 Comparison of ODI and VAS scores
There were no significant differences in ODI and VAS scores between the two groups before treatment (allP>0.05). After 21 d of treatment, the ODI and VAS scores of the two groups were lower than those before treatment in each group. The differences within the groups were statistically significant (allP<0.05). The scores of the observation group were lower than those of the EA group, and differences between the two groups were statistically significant (allP<0.05). This indicated that the improvements of the functional disorders and pain in the observation group were more significant than those in the EA group (Table 4).

Table 3. Comparison of OPG and IL-1β contents (x±s)

Table 4. Comparison of ODI and VAS scores (x±s, point)
4 Discussion
Osteoporotic compression fractures occur in the elderly resulting from bone destruction, degeneration,and decreased bone strength due to bone imbalance and anabolic imbalance[10-11]. The severe back pain that occurs in osteoporotic compression fractures can affect the quality of life of patients. In severe cases, it may also lead to dysfunction of multiple systems, such as breathing and digestion, and even death[12-13].Sinomenine is an alkaloid extracted from the dried rhizomes ofQing Feng Teng(Caulis Sinomenii) and has analgesic, anti-inflammatory and anti-rheumatic effects[14]. Because of its obvious inhibitory effect on IL-1β and other inflammatory factors, it is often used in clinic to treat rheumatism, rheumatoid arthritis and osteoarthritis[15].
Studies have shown that after fracture increased synthesis of IL-1β will promote the apoptosis of chondrocytes and reduce osteoblasts. This will greatly slow down the formation of bone callus. Sinomenine can reduce the synthesis of serum IL-1β, which is beneficial to the proliferation of osteoblasts after fracture, and can promote the formation of callus and accelerate fracture healing[16]. OPG maintains normal bone calcification and is a coupling factor for osteogenic and osteoclastic process. Increased OPG can inhibit osteoclast differentiation and induce apoptosis, which is of great significance for reducing bone resorption[17]. EA at Jiaji (EX-B 2) points can regulate the meridian qi,improve the local micro-environment of muscles,promote IL-1 metabolism, promote the absorption of inflammation and detumescence, relieve psoas muscle spasm, and restore muscle tension, thereby reducing back pain[18]. Studies have shown that sinomenine can increase OPG synthesis. EA at Jiaji (EX-B 2) points followed by sinomenine hydrochloride injection at Jiaji(EX-B 2) points can transfer the drug directly to the disease area, to achieve the purpose of dispelling wind and dampness and activating meridian[19].
In this study, the observation group was treated with sinomenine hydrochloride injection at Jiaji (EX-B 2)points on the basis of the treatment in the EA group.After 21 days of treatment, the content of OPG in the observation group was significantly higher than that before treatment and after treatment in the EA group(P<0.05), indicating that OPG synthesis and osteoblast activity increased, calcium and phosphorus metabolism returned to normal, bone calcium deposition increased,the formation of new bone and callus was accelerated,and osteoporosis also improved. The content of IL-1β,ODI and VAS scores in the observation group were significantly lower than those before treatment and after the treatment in the EA group (allP<0.05). This indicated that the symptoms of low back pain were relieved and the patients’ self-care ability improved in the observation group. These results suggested that on the basis of conventional drug therapy, EA at Jiaji(EX-B 2) points plus injection of sinomenine hydrochloride should be superior to EA alone.
Conflict of Interest
There was no potential conflict of interest in this article.
Acknowledgments
This work was supported by 2013 Integrated Traditional and Western Medicine Scientific Project of Traditional Chinese Medicine, Health Department of Hubei Province(2013年湖北省卫生厅中医药中西医结合科研项目,No. 2013Z-B13).
Statement of Informed Consent
Informed consent was obtained from all individual participants or their relatives in this study.
Received: 12 September 2017/Accepted: 15 October 2017
[1] Shan JL, Zhang Y, Shan ZL, Li F. Mechanism of lumbosacral pain in thoracolumbar vertebral compression fractures. Jizhu Waike Zazhi, 2015, 12(1): 33-36.
[2] Zhu XJ, Wang XJ, Chi MY, Huo LL. Interventive study on health management of senile osteoporosis in alpine region combined with acupuncture. Zhenjiu Linchuang Zazhi,2015, 31(4): 4-6.
[3] Liu XW, Sun LR, Xia Y. Clinical observation on acupuncture combined with self-made Bu Shen Zhuang Gu decoction to improve osteoporosis pain. Zhongguo Zhongyi Jizheng, 2015, 24(2): 303-305.
[4] Ke LJ, Xu J. Clinical observation on treatment of senile osteoporotic lumbar compression fracture with Jian Yao Zhuang Gu decoction. Zhongguo Zhongyi Jizheng, 2014,23(6): 1138-1139.
[5] Liang Y, Pi M, Xie Z, Li YL. Clinical observation of Shao’s points injection with kukoline hydrochlorid injection in treating chronic lower back pain due to disorders of posterior ramus of spinal nerves.Xin Zhongyi,2014, 13(1): 154-157.
[6] Chen J, Lei NW, Liu JF, Zhu LW. Therapeutic effect of Jiaji (EX-B 2) electroacupuncture with botulinum toxin type A on chronic low back pain.Zhenjiu Linchuang Zazhi,2016, 32(4): 4-6.
[7] Zhang ZH, Liu ZH, Li N. Expert consensus on the diagnosis of osteoporosis in Chinese population (3rd draft,2014 edition). Zhongguo Guzhi Shusong Zazhi, 2014,20(9): 1007-1010.
[8] Wang QC. Therapeutics of Acupuncture and Moxibustion.Beijing: China Press of Traditional Chinese Medicine,2007: 60-61.
[9] Wang G, Long XY, Liu LJ, Liu H. Effect of warm needling moxibustion on bone density, BGP and IL-6 in osteoporotic compression fracture. Shanghai Zhenjiu Zazhi, 2017,36(12): 1455-1458.
[10] Wang XZ, Fu Q. Research progress of postmenopausal osteoporosis treated by chinese medicine. Henan Zhongyi,2014, 34(3): 565-566.
[11] Li ZL, Yang ZK. The application of balloon vertebroplasty in the treatment of senile vertebral compression fracture.Zhongguo Yiyao Kexue, 2016, 6(4): 172-175.
[12] Chen Y, Li JY, Xiao B, Zhao R. Characteristics review of clinical studies on acupuncture-moxibustion for osteoporosis. Shanghai Zhenjiu Zazhi, 2014, 33(3): 274-277.
[13] Wang SM, Chen C, Huang XB. Analysis of the causes of residual low back pain after percutaneous vertebroplasty for osteoporotic vertebral compression fractures. Jilin Yixue, 2014, 35(30): 6751-6752.
[14] Zhang XY, Gao YX. Research Progress of immunosuppression and anti-inflammatory activity of Sinomenine. Hunan Zhongyi Zazhi, 2016, 32(3): 193-194.[15] An YB, Lu TZ, Hai B. Effects of sinomenine injection on knee osteoarthritis fluid and serum cytokines of rabbit.Zhongguo Laonianxue Zazhi, 2016, 36(4): 788-791.
[16] Yang HQ, Chen LR. Effects of sinomenine on synovial fluid and serum content of interleukin-1β in rabbits with osteoarthritis. Zhong Xi Yi Jie He Xue Bao, 2008, 6(12):1275-1279.
[17] Wagner D, Fahrleitner-Pammer A. Levels of osteoprotegerin (OPG) and receptor activator for nuclear factor kappa B ligand (RANKL) in serum: are they of any help? Wien Med Wochenschr, 2010, 160(17-18): 452-457.[18] Shang DF. Clinical observation and effect on pain of lumbar intervertebral disc protrusion treated with warm acupuncture at lumbar Jiaji (EX-B 2) points. Xin Zhongyi,2016, 48(7): 134-136.
[19] Ding CZ, Yao Y, Fang Y, Sun LY, Wang Y. Effects of sinomenine on OPG/RANKL, lL-17 in serum of collageninduced arthritis rats. Nanjing Zhongyiyao Daxue Xuebao,2012, 28(4): 330-333.
猜你喜欢
江科学术研究(2022年3期)2022-09-26 12:27:54
Journal of Acupuncture and Tuina Science(2022年1期)2022-02-24 04:33:50
Journal of Acupuncture and Tuina Science(2022年1期)2022-02-24 04:33:50
航天工业管理(2020年1期)2020-04-20 13:32:52
甘肃教育(2020年12期)2020-04-13 06:24:16
当代陕西(2019年23期)2020-01-06 12:17:42
当代陕西(2018年7期)2018-04-26 02:45:20
公民与法治(2016年4期)2016-05-17 04:09:24
西藏科技(2015年12期)2015-09-26 12:13:40
Journal of Beijing Institute of Technology(2015年1期)2015-04-24 05:37:46
 Journal of Acupuncture and Tuina Science2018年3期
Journal of Acupuncture and Tuina Science2018年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Influence of acupuncture on pulmonary function of patients with asthma: a review
- Observation on lower-reinforcing and upperreducing acupuncture method for hyperplasia of mammary gland and its influence on estradiol and progesterone
- Clinical observation on electroacupuncture at four sacral points for overactive bladder syndrome
- Observation on clinical efficacy of warm needling therapy for chronic lumbar strain
- Observation on clinical effects of acupuncture plus external medicine application forcervical radiculopathy
- Effect of acupoint sticking at Shenque (CV 8) for preventing spleen-stomach disharmony caused by venous analgesia pump