
Lesson Eighty-three Cardiacmemory-diagnostictool in the making1
2018-06-06 03:03:15童鸿
心电与循环 2018年3期
(童鸿)
Classic definition of the term cardiac memory(CM)refers to the persistent T-wave changes on the ECG after a period of wide QRS rhythms that become evident once normal ventricular activation pattern is restored.It is related to the term ventricular electric remodeling sometimes used in basic science literature.Although CM itself is considered as an adaptive reaction to the change in the ventricular activation sequence,its manifestations (usually T-wave inversions,TWIs)are often confused with pathological conditions manifesting with TWI,such as myocardial ischemia or infarction.
In 1982,Rosenbaum et al introduced the term heart memory and presented the first unified hypothesis of how abnormal ventricular activation could lead to the development of T-wave abnormalities regardless of the wide QRS cause by a process he referred to as electrotonic modulation.In this seminal article,3 principles of CM were formulated:(1)the direction of the T waves in sinus rhythm follows (remembers)the direction of the QRS complex during preceding episode of abnormal activation;(2)the amplitude of memory T waves increases the longer abnormalconduction continues,and (3)repeatepisodesofabnormal activation after complete normalization of T waves result in more rapid and prominent accumulation of T-wave changes(hence the term memory).
Molecular Mechanisms
In brief,CM comprises a spectrum of 2 distinct but overlapping phenomena which differ in the mechanisms by which repolarization changes are achieved:shortterm and long-term CM.Short-term CM observed within minutes of ventricular pacing is thought to occur from modulation and modification of existing proteins and channel trafficking.It is relatively short-lived and dissipates within minutes.Long-term CM is seen after longer periods of abnormal activation and is longer lasting (days to weeks).It includes changes in gene transcription and protein synthesis.Molecular changes observed in the setting of CM include alterations of multiple ion channels,receptors,and cell coupling,including the transient outward current,Ito,IKr,ICa,Na/Ca exchanger,AT1 receptors,stretch-activated receptors,and gap junction redistribution.
Triggers of CM
Perhaps the most important discovery in the physiology of CM was establishing its relationship to the mechanical function of the heart.The notion that it is the change in ventricular contraction pattern and local ventricular wall stress (as opposed to electrotonic modulation originally proposed by M.Rosenbaum)that triggers CM was first made on the basis of CM inhibition by the renin-angiotensin system blockade.It was later confirmed in elegant experiments with excitation-contraction uncoupling demonstrating that pacing-induced CM only develops if the change in the electric activation sequence is accompanied by the active mechanical contraction, whereas CM-like changes can develop as the result of local mechanical myocardial stretching alone without electric activation change.
Role of Vectorcardiography in Evaluation of CM
As originally noted by Rosenbaum et al,not only the T waves follow the direction of the wide QRS complex in each ECG lead,but also the whole T-wave 3-dimensional vector aligns with the wide QRS vector when assessed using vectorcardiography.
This3-dimensionalnature ofrepolarization changes in CM made vectorcardiography a preferred tool of its assessment so that instead of tracking disparate T-wave polarities and amplitudes in individual leads the change in the whole T-wave vector can be observed and measured. The vectorcardiography-based measurement of CM,T-vector peak displacement was developed.It allowed to express CM magnitude as a single numeric value and track its changes under different experimental conditions.
Why was CM Initially Described only during Normal Ventricular Activation
Traditionally,CM has been associated with TWI during sinus rhythm with narrow QRS for several reasons:
First,normal T waves during sinus rhythm are positive in mostleads,whereasTWIisusually associated with pathological conditions (eg,ischemia,strain, cerebral hemorrhage). Therefore, T-wave changes are more likely to be noticed when TWI is present.Second,in the most common situations leading to CM development (LBBB,right ventricular apical pacing),wide QRS deflections initiating CM are negative in the majority of the leads and therefore produce TWI.Third,large secondary repolarization changes during wide QRS rhythms mask CM until the QRS becomes narrow(Figure 1).
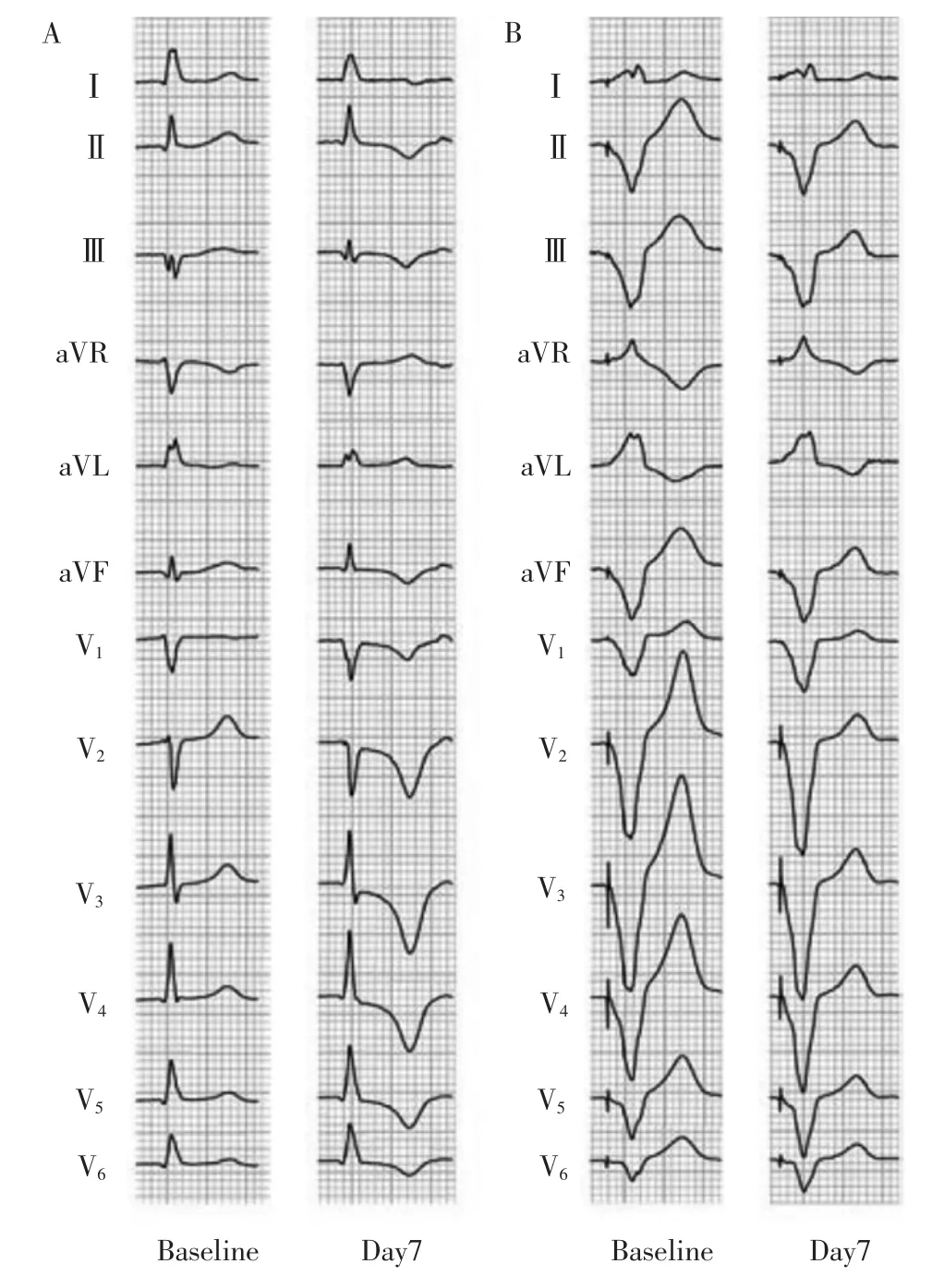
Figure 1 ECG during narrow (AAI pacing,A)and wide QRS(DDD pacing,B)before (baseline)and after cardiac memory(CM)induction(day 7).A,At baseline,the T waves during AAI pacing are positive in most leads.On day 7 during AAI pacing,inverted T waves in multiple leads assume the polarity of the paced QRS complex consistent with CM.B,During wide QRS rhythm,CM manifests as a decrease in the T-wave amplitude with no change in polarity on day 7 compared with the baseline. Unless quantitative vectorcardiography methods are used to measure the T-wave loop,this change usually goes unnoticed on a 12-lead ECG.
Distin guishing between TWI from CM and Ischemia
Since the time CM was first described,its similarity to ischemic TWI made it a significant confounder in the diagnosis of myocardial ischemia often resulting in excessive cardiac testing.In particular,precordial TWI because of intermittent right ventricular pacing or LBBB(by farthe mostcommon presentationsofCM encountered in clinical practice)can be easily confused with the Wellens'syndrome2characteristic of transient proximalleftanteriordescending coronary artery occlusion,a condition requiring promptcoronary intervention.
In general,the direction of the ischemic T-waves points away from the area of ischemia.Because the ischemic region attributable to the proximal left anterior descending coronary artery lesion involves the left ventricle,the ischemic precordial TWI has a rightward axis in the frontal plane and is characterized by TWI in leads I and aVL.The rare cases of right coronary artery ischemia producing precordial TWI with the leftward axis have deeper TWI in inferior leads than that in the precordial leads.However,right ventricular apical pacing and LBBB produce QRS vectors positive in leads I and aVL resulting in positive T waves in these leads on resumption of normal conduction consistent with CM principles.It also produces precordial TWI deeper than the inferior TWI.
The combination of positive T in lead aVL and positive/isoelectric T in lead I,and precordial TWI>inferior TWI produces a unique pacing induced CM signature that was 92%sensitive and 100%specific in differentiating pacing-induced TWI from ischemia in a retrospective study.

Figure2 Vectorcardiogram of the patient in Figure 1 during AAI and DDD pacing in frontal (A)and transverse(B)projections before(baseline)and after the induction of cardiac memory (CM;day 7).On day 7 during AAI pacing,the T vector assumes the direction of the paced QRS complex while increasing in magnitude.At the same time in DDD mode,the T-vector magnitude decreases with no change in direction.Black arrows indicate the direction and magnitude of the projection of T-peak displacement as the result of CM and are similar in AAI and DDD modes.
Cardiac Memory in Wide QRS Rhythms
Despite the fact that processes underlying CM do not develop suddenly on QRS normalization but rather progress gradually during abnormal ventricular activation,for a long time it was thought that CM cannot be detected until QRS becomes narrow.Secondary T-wave changes in wide QRS rhythms occur immediately and are dominant,whereas CM-induced T-wave changes are initially subtle and while gradually increasing over time are obscured by the secondary changes.The assessment of CM by surface ECG in the setting of wide QRS is limited because of the dominance ofthesecondaryT-wave changes.Repolarization changes because of CM in this situation have been largely overlooked,being masked by the large discordant T waves.Nevertheless,vectorcardiogram can readily detect CM in this situation.Figure 2 presents the vectorcardiogram of the patient shown in Figure 1 demonstrating the 3-dimensional T-vector displacement after 7 days of right ventricular pacing during the narrow(AAI pacing)and wide(DDD pacing)QRS.The actual T-vector change (T peak displacement)in the narrow and wide QRS is nearly identical in both magnitude and direction.As seen on both Figures 1 and 2,CM in wide QRS rhythms presents as a decrease in T-vector magnitude without directional change (another reason why they are usually missed)in contrast to the narrow QRS rhythm,where T vector becomes larger and rotates toward the paced QRS. Using quantitative vectorcardiograpic analysis,CM can be detected in paced rhythm within minutes after the onset of pacing.
Clinical Application of CM in Wide QRS:Age Determination of LBBB
The finding that CM decreases discordant T-wave amplitude in wide QRS rhythms has important clinical implications.For example,it can be used to determine whether LBBB is old or new which becomes valuable in the setting of chest pain.
The criterion for LBBB age determination was developed on the premise that new LBBB would have larger T vector(and taller T waves on a 12-lead ECG)compared with the old one in accordance with CM development in wide QRS rhythm (Figure 3).As the duration of LBBB increases the discordant secondary T waves become smaller (Figure 3A).A retrospective analysis>1700 LBBB ECGs showed that indeed the new onset LBBB (defined as<24-hour duration)was rare(3%)and had significantly larger T waves(as well as smaller QRS vector magnitude)compared with the chronic LBBB (Figure 3B and 3C).Although the best results in LBBB age determination were achieved using quantitative vectorcardiography technique,a simplified 12-lead ECG criterion using the ratio of the maximal precordial S wave/maximal precordial T-wave amplitude(asapproximationsofthe QRS and T vectors,respectively)was also developed.A conservative cutoff of S/T<2.5 allowed to detect 100%of the new LBBBs.

Figure 3 Use of the maximal precordial S/T ratio in left bundle branch block (LBBB)age determination.S/T represents the ratio of the maximal precordial S wave/maximal precordial T-wave amplitude.A,As the duration of LBBB increases,the maximal precordial S/T ratio increases from 1.64 at 6 hours(=new)to 3.22 at 15 days(=old).B,A typical example of resolution of a new LBBB (<8-hour duration).S/T ratio is 1.61.Resolution of LBBB results in no apparent T-wave abnormalities during narrow QRS.C,A typical example of resolution of an old LBBB (>3-day duration).S/T ratio is 2.93.Typical changes of cardiac memory with precordial TWI are evident during narrow QRS.D,A new onset LBBB (<75 minutes)in a setting of an acute left anterior descending coronary artery thrombosis.S/T ratio is 1.68 consistent with the new LBBB.Note ST segment changes in the baseline tracing consistent with ischemia and loss of R waves after resolution of LBBB.
TheT-vectormagnitudein LBBB changes significantly during the first 24 hours.In cases of painful LBBB syndrome when ECG isrecorded within seconds/minutes of symptoms onset (often during an exercise stress test),S/T ratio can be as low as 1.4.The majority of the T-wave changes occur within the first 24 hours of LBBB persistence when it assumes chronic QRST configuration.In the true chronic LBBB,the S/T ratio is close to≥3.0 (Figure 3A and 3C).It is important to recognize that LBBB is often a dynamic phenomenon and can be intermittent or rate-dependent.Repeated episodes of intermittent LBBB can cause accumulation of CM-related T-wave changes,sometimes making the distinction between new and old LBBB difficult.
The new LBBB S/T criterion held true in a small subgroup of patients with acute coronary syndrome(Figure 3D)but needs to be confirmed in larger clinical trials.
词 汇
seminal adj.精液的,繁殖的,种子的
trafficking n.非法买卖
dissipate v.驱散,使……消散,消散,使...散放,放荡,耗散,浪费,使……耗散
synthesis n.综合,合成,合题
elegant adj.雅致,优美的,精确的,上等的
vectorcardiography n.心电向量测定法
disparate adj.全异的
displacement n.移位,位移,撤换
confounder n.混乱者
resumption n.重新开始,恢复
obscure adj.&v.晦涩的,无名的,隐藏的;使……变暗,遮住,使……难解
premise n.假定,前提;v.引出
土壤消毒的方法有:高温消毒和药物消毒,高温消毒就是把整个大棚密闭,高温闷棚7~8天。药物消毒就是把多菌灵与湿润细土按1∶25的比例拌匀后与基肥均撒在地面上,同时用辛硫磷(500克/亩)对水喷雾,然后进行深翻,既灭菌又灭地下害虫。种子处理的做法有:将备足的种子用两份开水对一份凉温水(55℃)浸种10分钟,边浸边搅动,先用30℃温水浸种3~4小时,再用高锰酸钾1000倍液浸泡15分钟,随即将种子用清水洗净,包好放入盆内,置于25~30℃处进行催芽,种子有半数露白时即可播种。
conservative adj.&n.保守,保守的,保守党,稳当的;保守者,防腐剂
注 释
1.in the making指“正在兴起、正在形成、策划中、酝酿中”等,如A stem cell that loses its immunoprotection over time is a time bomb in the making.随着时间推移,失去免疫保护的干细胞是潜在的定时炸弹。
2.Wellens'syndrome是De Zwaan等于80年代首先描述的一种综合征,患者胸痛时心电图表现为V2、V3T波深倒(>5mm)或双向,ST段不抬高或轻度抬高,是冠状动脉前降支近端严重狭窄的特征性改变,预示前壁大面积梗死的危险,而当患者来急诊时通常已无胸痛症状,心肌酶正常或仅轻度增高,如果单纯药物治疗,75%会在数周内发生急性心肌梗死。
参考译文
第83课心脏记忆:新兴的诊断工具
术语心脏记忆的经典定义是指一段时间宽QRS节律后心电图上出现的持续性T波变化,一旦恢复正常心室激动图形后,这种T波变化就变得显而易见。这与有时用于基础科学文献中的术语心室电调节相关。虽认为心脏记忆本身是对心室激动顺序变化的适应性反应,其表现(通常为T波倒置,T-wave inversion,TWI)经常与呈现TWI的病理状态如心肌缺血或梗死相混。
1982年,Rosenbaum等引入术语心脏记忆,并首次提出,无论宽QRS波群的原因是什么,异常心室激动通过他称作电张调节的过程如何导致T波异常的统一假设。在这一开创性文章中,规定了心脏记忆的三原则:(1)窦性节律的T波方向追随其前一阵异常激动的QRS波群方向;(2)记忆T波振幅随异常传导持续时间延长而增大;(3)T波完全正常化后,重复一阵异常激动导致更快速和明显的T波变化累积。
分子机制
简言之,心脏记忆由两种复极机制明显不同但却重叠的一组现象构成,即短期和长期心脏记忆。短期心脏记忆见于心室起搏后数分钟内,认为与现存的蛋白调节和修饰以及通道的异常通行有关。持续时间短,数分钟内消失。长期心脏记忆见于较长时间的异常激动后,持续时间较长(数天到数周)。涉及基因转录和蛋白合成的变化。心脏记忆研究观察到的分子变化包括多个离子通道、受体、细胞偶联的改变,包含短暂外向电流、Ito,IKr,ICa,Na/Ca交换蛋白,AT1受体,伸拉活化受体和间隙连接再分布。
心脏记忆的促发因素
心脏记忆电生理学中最为重要的发现也许是正在建立起其与心脏机械功能的关系。基于血管紧张素系统抑制剂对心脏记忆的抑制,首次提出促发心脏记忆的是心室收缩类型与局部室壁应力变化这一概念(与Rosenbaum最初假设的电张调节相对立)。这在以后兴奋-收缩解偶联的精准实验中得以证实,起搏诱发的心脏记忆只发生于电激动顺序变化伴随主动机械收缩时,而不伴电激动变化的局部机械性伸展会产生心脏记忆样变化。
心电向量在评价心脏记忆中的作用
正如Rosenbaum最初观察到的,采用向量图分析显示,不仅每个心电图导联上的T波追随宽QRS波群方向,整个T波三维向量与宽QRS波群向量相一致。
心脏记忆中复极变化的三维特性,使得心电向量图成为复极变化分析的优选工具,以致取代追踪各个心电图导联上T波反向极性和振幅,从而观察和测量整个T波向量的变化。已形成以心电向量图为基础的心脏记忆测定,即T波-向量峰值位移。这使得心脏记忆幅度可用单个数值表达,并可追踪不同实验条件下的变化。
为什么最初描述的心脏记忆只出现于正常心室激动期间
传统意义上,窦性节律窄QRS波群时心脏记忆总与TWI联系在一起有几个原因:
首先,窦性节律时的正常T波在多数导联呈正向,而TWI通常与病理状态(如缺血、劳损、脑出血)相关。因此,当出现TWI时更易观察到T波的变化。其次,在最常导致心脏记忆发生的状态 [左束支传导阻滞(LBBB),右心室心尖起搏],引发心脏记忆的宽QRS波群在多数心电图导联上是负向的,因此而产生TWI。第三,宽QRS节律时大的继发性复极变化掩盖了心脏记忆,直至QRS波群变窄(图1)。
心脏记忆与缺血所致TWI的鉴别
自从心脏记忆首次提出那一刻开始,它与缺血性TWI的相似性使得其成为心肌缺血诊断的重要鉴别对象,经常导致过度的心脏检测。特别一提的是源于间歇右心室起搏或LBBB(至今临床实践中最常遇见的心脏记忆)的胸导联TWI,易与冠状动脉前降支近端短暂阻塞引起的Wellans'综合征相混,后者需要紧急冠状动脉介入治疗。
通常,缺血性T波的方向背离缺血区。因前降支冠状动脉近端病变引起的缺血累及左心室,额面上缺血性胸导联TWI电轴右偏,特征表现为Ⅰ和aVL TWI。右冠状动脉缺血引起电轴左偏、胸导联TWI的罕见病例,下壁导联的TWI较胸导联深。然而,右心室心尖起搏和LBBB产生I和aVL QRS波向量向上,基于重新开始的正常传导与心脏记忆一致的原理,导致这些导联T波向上,这也导致胸导联TWI深度超过下壁TWI。
一项回顾性研究显示,结合aVL T波直立和ⅠT波直立/等电位线,以及胸导联TWI>下壁TWI,产生独特的起搏诱发心脏记忆特征,这对鉴别起搏和缺血诱发的TWI的敏感性和特异性分别达92%和100%。
宽QRS波群节律心脏记忆
尽管心脏记忆的过程并非突发于QRS波群正常化,而是在异常心室激动过程中逐渐进展,在很长一段时间内认为,除非QRS波群变窄,否则,不能探及心脏记忆。宽QRS节律时即刻发生继发性T变化且明显,而心脏记忆诱发的T波变化初始细微,随着时间推移逐渐增大却被继发性变化所掩盖。因为继发性T波变化明显,在宽QRS波群情况下通过体表心电图分析心脏记忆受限。在这种情况下,心脏记忆引起的复极变化多被忽视,因为受到大而反向的T波掩盖。尽管如此,心电向量图能随意检测到此时的心脏记忆。图2呈现的是图1的心电向量图,证实7d起搏后窄QRS波群(AAI起搏)和宽QRS(DDD起搏)波时的三维T-向量位移。窄和宽QRS波时实际T-向量变化(T波移位)的量和方向近乎一致。正如图1和图2所示,宽QRS节律时心脏记忆呈现T-向量降低而方向不变(这是为什么常被遗漏的另一原因),而窄QRS波群节律时,T向量增大并且旋转指向起搏QRS波群方向。采用定量心电向量图分析,于起搏后数分钟内即可探及起搏节律的心脏记忆。
宽QRS波群时心脏记忆的应用:LBBB时间的确定
心脏记忆降低宽QRS节律时反向T波幅度具有重要临床意义。例如,它可用于确定LBBB是陈旧的或新发的,这在胸痛时显得很重要。
根据宽QRS节律时心脏记忆的形成(图3),与陈旧的LBBB相比,新发LBBB T向量较大(12导联心电图上T波高尖),以此为前提,形成鉴别LBBB发生时间的标准。随着LBBB持续时间延长,反向的继发性T波变小(图3A)。回顾分析>1 700例LBBB心电图发现,新发LBBB(定义为<24h)极少见 (3%),与慢性LBBB比较具有明显高尖T波(而QRS向量较小)(图3B和3C)。虽然采用定量心电向量图技术确定LBBB时间能达到最佳结果,但采用胸导联最大S波与最大T波振幅比值的简单12导联心电图标准已经形成。取S/T<2.5的保守截点,能100%诊断新发LBBB。
LBBB时T-向量幅度最初24h变化明显。在疼痛性LBBB综合征,于症状发作的数秒或数分钟内记录到的心电图(常在运动负荷试验时),S/T比值可低至1.4。大多数T波变化发生于LBBB持续的最初24h内,其时表现为慢性QRST图形。对于真正的慢性LBBB,S/T比值≥3(图3A和3C)。重要的是应该认识到LBBB常呈动态变化,可呈间歇性或频率依赖。反复间歇性LBBB可引起心脏记忆相关T-波变化的累积,有时使得新发与陈旧LBBB难以鉴别。
新的LBBB S/T标准在小样本急性冠脉综合征亚组患者中保持准确性(图3D),但需在较大的临床试验中加以证实。
图1 诱发心脏记忆前(基础)后(第7天)窄(AAI起搏,A)和宽(DDD起搏,B)QRS心电图。A:基础状态下,AAI起搏期间T波多数导联直立。AAI起搏第7天,多个导联T波倒置,呈现起搏QRS综合波极性与心脏记忆的一致。B:宽QRS波群节律期间,与基础状态比较,第7天心脏记忆表现为T-波振幅降低而极性不变。除非采用定量心电向量图方法测定T-波环,否则,12-导联心电图上这种变化通常被忽视。
图2 图1患者AAI和DDD起搏期间诱发心脏记忆前(基础)后(第7天)的额面(A)和横面(B)心电向量图。AAI起搏第7天,T向量与起搏QRS波群方向一致,而振幅增大。DDD模式的同一时间,T-向量振幅减小而方向不变。黑色箭头标明因心脏记忆产生的T-峰位移突起的方向和幅度,AAI和DDD模式下相似。
图3 胸导联最大S/T比值在LBBB时间判断中的应用。S/T代表最大胸导联S波/最大胸导联T-波振幅。A:随着LBBB时间延长,最大胸导联S/T比值从6h(=新发)的1.64增至15d(=陈旧)的3.22。B:新发LBBB(<8h)缓解的典型病例。S/T比值是1.61,LBBB缓解致使窄QRS期间无明显T-波异常。C:陈旧LBBB(>3d)缓解的典型病例。S/T比值2.93,窄QRS波群期间呈典型的心脏记忆胸导联TWI变化。D:急性左前降支冠状动脉血栓导致的新发LBBB(<75min)。S/T比值1.68与新发LBBB相一致。注意基础状态下ST段变化与缺血相符,LBBB缓解后R波消失。
[1]Shvilkin A,Huang HD,Josephson ME.Cardiac Memory-Diagnostic Tool in the Making.Circ Arrhythm Electrophysiol.2015;8:475-482.
猜你喜欢
昆明医科大学学报(2021年4期)2021-07-23 01:22:00
自动化与信息工程(2021年1期)2021-03-12 11:20:48
心电与循环(2019年6期)2019-12-10 01:37:40
电子制作(2019年19期)2019-11-23 08:41:40
中国生物医学工程学报(2019年6期)2019-07-16 07:52:38
心电与循环(2019年2期)2019-04-10 12:09:24
心电与循环(2019年2期)2019-02-19 13:40:02
广西林业科学(2016年3期)2016-03-16 05:43:23
医学研究杂志(2015年5期)2015-06-10 06:43:26
四川生理科学杂志(2014年1期)2014-02-28 14:08:24
