
Clinical observation of Shu-acupuncture method in Nei Jing (Classic of Internal Medicine) for shoulder and arm pain
2018-03-13 12:57:18SongZhongyang宋忠阳QinXiaoguang秦晓光FangXiaoli方晓丽ChenYuchan陈玉禅
Song Zhong-yang (宋忠阳), Qin Xiao-guang (秦晓光), Fang Xiao-li (方晓丽), Chen Yu-chan (陈玉禅)
1 School of Acupuncture and Tuina, Gansu University of Chinese Medicine, Lanzhou 730000, China
2 Cooperation of Chinese and Western Medicine Department, Gansu University of Chinese Medicine, Lanzhou 730000, China
Shoulder and arm pain is a common disorder involving the muscles and joints. It mainly causes pain in the arm and shoulder joints, coupled with a sensation of soreness, heaviness or numbness. Although multiple factors may cause shoulder/arm pain, the most common causes are chronic neck/shoulder muscle strain or soft tissue problems[1]. Today, shoulder and arm pain is being seen in younger people who spent too much time using electronic devices. Clinical studies have proven that acupuncture has a remarkable effect,fewer side effects and lower cost for shoulder and arm pain[2-3]. Since conventional acupuncture often has a shallow insertion, produces a mild needling sensation and requires a long treatment course, the authors of this paper treated 45 cases with the classicalShu-acupuncture method and compared with the efficacy obtained by the conventional acupuncture. The results are now summarized as follows.
1 Clinical Materials
1.1 Diagnostic criteria
In reference to the diagnostic criteria for cervical spondylopathy and shoulder joint problems inCriteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine, the diagnostic criteria in this study were self designed[4]:pain in the neck and shoulder, with uncomfortable stiffness and difficult motion; history of long-term strain in the neck and shoulder, repeated history of neck pain,history of soft tissue injury, history of shoulder joint problem or cervical spondylopathy, abnormal X-ray results; sore and stuck sensation in the shoulder and arm, possibly accompanied by numbness in the fingers and radiating pain. The diagnosis was made based upon the presence of previous 2 items, or items 2 and 3, or items 1 and 2, or previous 3 items.
1.2 Inclusion criteria
In conformity with the above diagnostic criteria; with the age ranging between 20 and 60 years old, and duration from 1-36 months; willing to accept the clinical observation and having signed the informed consent.
1.3 Exclusion criteria
Not in conformity with the above diagnostic criteria;patients with shoulder and arm pain not only caused by cervical and soft tissue problems; patients with diseases of other systems (such as heart diseases, hepatitis) and on long-term administration of medications; pregnant women; patients with mental disorders.
1.4 Rejecting criteria
Those unable to tolerate the treatment or the treatment continued less than 2 courses; unable to follow the doctor’s advice, on medications or other therapies during the treatment; those dropped out voluntarily and unable to receive the observation of the therapeutic effects.
1.5 Statistical analysis
The SPSS 20.0 version statistical software was used for statistical analysis. The measurement data were first processed by the normality test. The measurement data in conformity with the normal distribution were expressed by mean ± standard deviation (x±s). The comparison between the groups was processed by the two independent samplet-test. The comparison within the group was processed by pairedt-test. The measurement data not in conformity with the normal distribution were processed by non-parametric test. The grading data were processed byRiditanalysis. The comparison of the rates was processed by Chi-square test.P<0.05 indicated a statistical difference.
1.6 General data
A total of 90 patients recruited in this study came from the Outpatient of Acupuncture Center of Gansu University of Chinese Medicine between November 2014 and June 2016. Based upon the order of their visit,the patients were divided by the random digital table into an observation group and a control group, 45 cases in each group. In the observation group, the age ranged from 20 to 57 years old and the duration ranged from 1 month to 34 months. In the control group, the age ranged from 22 to 60 years old and the duration ranged from 2 months to 36 months. In comparison of the general data of the gender, age and duration between the two groups, the differences were not statistically significant (allP>0.05), indicating that the two groups were comparable (Table 1).
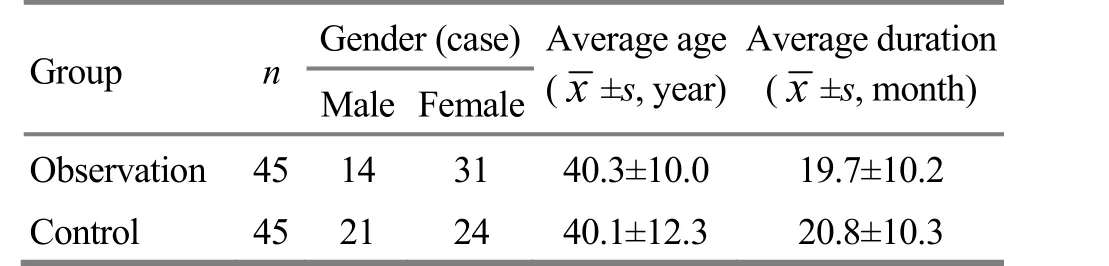
Table 1. Comparison of general data between the two groups
2 Treatment Methods
2.1 Observation group
Major points: Jianyu (LI 15), Jianliao (TE 14), Jianzhen(SI 9), Jianqian (Extra), Yanglingquan (GB 34) and Ashi point.
Adjunct points: Houxi (SI 3) and Shenmai (BL 62)were added for neck pain; Quchi (LI 11) and Hegu (LI 4)were added for serious pain in the upper limb.
Method: After the patient took a sitting position and routine disinfection of the points, filiform needles of 0.30 mm in diameter and 50 mm in length were selected. ByShu-acupuncture method, the needles were inserted perpendicularly in the major points, for about 2 cun with the needle tip reaching the surface of the bone. After the arrival of the needling sensation,the needles were slightly twisted till a sinking and tight sensation appeared. The adjunct points were managed by routine needling method[5], with the needles retained for 30 min. After the treatment, the patients were asked to exercise the neck, shoulder and upper limb.
2.2 Control group
Points: Same as the observation group.
Method: After the patient took a sitting position and routine disinfection of the points, filiform needles of 0.30 mm in diameter and 50 mm in length were selected. By pressing skin of the point with the index finger or thumb of the left hand, the needles were inserted by the right hand into the points for about 1.0-1.5 cun. After arrival of the needling sensation, the needles were twisted by an angle of 180-360° and at a frequency of 60-90 r/min[5], repeatedly for 1 min, and then retained for 30 min. After the treatment, the patients were asked to move the neck, shoulder and upper limb.
The two groups were treated once every day, with 5 treatments as one course, and a 2-day rest between two courses, for 3 courses in total.
3 Observation on Therapeutic Effects
3.1 Observed items
Respectively before and after the treatment, pain was assessed by visual analog scale (VAS)[6]: a cardboard scale of 10 cm in length, the left side marked 0 cm,expressing no pain, scored 0 point; the right side marked 10 cm, expressing intolerable serious pain,scored 10 points. The patients were asked to score based upon the pain degree.
3.2 Criteria of therapeutic effects
Cure: Pain disappeared, with VAS scored 0, and the patient can have normal life and work.
Remarkably effective: Pain basically disappeared, or VAS score decreased by ≥ 3 cm.
Effective: Pain was somewhat alleviated, or VAS score decreased by ≥ 1 cm, but < 3 cm.
Failure: Pain did not disappear, or VAS score decreased by < 1 cm.
3.3 Results
3.3.1 Comparison of VAS score
The difference in VAS score between the two groups before the treatment was not statistically significant(P>0.05), indicating that the two groups were comparable. After the treatment, VAS scores decreased in both groups, and the intra-group differences were statistically significant (P<0.01,P<0.05), indicating that both protocols can alleviate pain. After the treatment,VAS score of the observation group was obviously lower than that of the control group, with a statistical intergroup difference (P<0.05), indicating thatShuacupuncture method is better than the routine needling method for shoulder and arm pain (Table 2).
3.3.2 Comparison of clinical effect
After the treatment, the total effective rate was 100%in the observation group, higher than 91.1% in the control group (χ2=4.186,P=0.041), and the curative rate was 93.3% in the observation group, higher than 24.4%in the control group (χ2=25.613,P=0.000), indicating that the therapeutic effect in the observation group was better than that in the control group (Table 3).

Table 2. Comparisons of VAS scores before and after the treatment (x±s, point)

Table 3. Comparison of clinical effect between the two groups (case)
4 Discussion
Today, the shoulder and arm pain is mainly treated by topical herbal application, injection or acupuncture. All these therapies help to relieve pain to some degree[2-3,7-8]. However, conventional acupuncture has a shallow insertion and cannot relieve the pain in the shoulder and arm, which often involves the bones and sinews. TheShu-acupuncture method, one of the five classical needling techniques recorded in theHuang Di Nei Jing(Yellow Emperor’s Classic of Internal Medicine)is mainly indicated for bone pain, limb numbness/pain/paralysis or hemiplegia[9]. Consequently,this study aims to observe its efficacy for shoulder and arm pain.
In Chinese medicine, the pain, numbness and impaired movement of the shoulder and arm result from chronic strain and retention of wind, cold and dampness in the joints, muscles or sinews. According to theHuang Di Nei Jing(Yellow Emperor’s Classic of Internal Medicine), pain most commonly occurs when wind, cold and dampness obstructs the flow of qi and blood[10]. The shoulder and arm pain occurs when cold dampness obstructs the flow of meridian qi and causes local muscle spasm.
In modern medicine, the shoulder and arm pain is commonly caused by degeneration of the shoulder joint,cervical vertebrae and humerus. Some patients may have soft tissue problems[11]. This study mainly focuses on bone degeneration. Individuals included in the study have long sedentary work hours or a history of local muscle strain and/or exposure to cold. The pain often has no fixed positions. Despite the intense pain in some patients, they have normal range of joint motion and normal radiological findings[1]. As a result, the treatment strategy is mainly to relieve local pain. Studies have found that acupuncture can speed up the local tissue metabolism and circulate qi and blood[12], reduce the skin electrical resistance, increase the skin conductivity,improve the local circulation, and thus alleviate pain[13].
‘Shu’, inShu-acupuncture method of the five classic needling techniques, means to discharge pathogenic cold and dampness from the muscles and bone joints[14].In the operation, the perpendicular puncture, deep to the bone, plus manipulation of the needles by the lifting,thrusting, twisting and rotating techniques in small amplitude, is supposed to soothe the tendons, dredge the collaterals, circulate qi, activate blood, strengthen the tendons and stop pain. The importance in its operation is the perpendicular insertion and perpendicular withdrawal of the needles, deep to the bone area of the points. On one hand, the perpendicular insertion of the needle can promote the needling sensation directly to the diseased area, for effectively exciting the meridian qi in the deep region.On the other hand, the perpendicular withdrawal of the needle can guide the pathogenic factor of the deep region to come out, so as to dredge the meridians and collaterals, dispel the pathogens and stop pain.Additionally, in terms of five Zang organs, the kidney dominates bone and produces marrow. Bone and marrow are the deep tissues of the human body[15].Shoulder and arm pain in the patients is mostly caused by the accumulation of pathogenic cold and dampness in the bone, and tendons and muscles of the deep region, deeper in the pathologic position. Therefore,only by deep puncture, can it be possible to excite the meridian qi of the human body, guide the meridian qi of the whole body to flow upward and discharge the pathogens[16]. In accordance with the sayings of ‘where the meridian goes through, where can be treated’, the points are selected by the combination of the local points and remote points, local points in predominance,in order to dredge the local meridians and collaterals,circulate qi and activate blood, plus the remote points to dredge the meridian qi and ensure the smooth circulation of the meridian qi[17]. Yanglingquan (GB 34),the influential acupoint of tendons in the Eight Influential Points, is able to soothe the tendons, activate the collaterals and stop pain. Houxi (SI 3) and Shenmai(BL 62) are the intersecting points of the eight meridians.Houxi (SI 3) links with the Governor Vessel and the Governor Vessel governs yang qi of the whole body.Shenmai (BL 62) links with the Yang Heel Vessel, and the Yang Heel Vessel dominates the activity of the limbs of the human body. The combination of those two points can dredge qi and blood in the neck and shoulder, and regulate the circulation of local qi and blood. Quchi(LI 11) and Hegu (LI 4) are respectively He-sea point and Yuan-Primary point of the Large Intestine Meridian of Hand Yangming. Two points in combination can dredge the meridians of the upper limbs and promote the circulation of the meridian qi of the upper limbs[18].Such a combination of the needling technique and points can ensure ‘problem eliminated while the needles are punctured’. Therefore, the satisfactory therapeutic effects can be achieved. Now, there are many clinical reports on application ofShu-acupuncture method. For instance, the better therapeutic effects are achieved in the treatment of the diseases, such as heel pain, numbness and pain of the lower limbs by lumbar disc herniation, knee osteoarthritis, byShuacupuncture method[19-21], proving that the therapeutic effects are satisfactory in the treatment of bone Bi-impediment syndrome and pain and numbness of the limb byShu-acupuncture method.
It has been found thatShu-acupuncture method in acupuncture treatment of shoulder and arm pain in predominance is strong in the needling sensation,obvious in propagation, fast in the therapeutic action,and short in the course, and can avoid the disadvantages of shallow needling stimulation, weak needling sensation, unobvious propagation, failure to reach the diseased area and long course in routine acupuncture. Therefore, it is worthy of clinical popularization.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
This work was supported by Project of Zheng’s Acupuncture Manipulation Academic Schools Heritage Work Room, Gansu Province, State Administration of Traditional Chinese Medicine (国家中医药管理局甘肃郑氏针法学术流派传承工作室项目, No. 2305135901).
Statement of Informed Consent
Informed consent was obtained from all individual participants in this study.
[1] Liu GQ. Differentiation diagnosis and integrative Chinese and Western medicine treatment of shoulder and arm pain.Fujian Zhongyiyao, 2014, 45(2): 32-33.
[2] Bao HM, Pan SR. Efficacy observation on acupuncture for 26 cases with shoulder and arm pain. Gong Qi Yikan, 1995,8(2): 72.
[3] Yu RZ, Zhang YL. Treatment of 20 cases with shoulder and arm pain by acupuncture, cupping and medication.Zhongguo Minjian Liaofa, 1999, 7(1): 29.
[4] State Administration of Traditional Chinese Medicine.Criteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing:Nanjing University Press, 1994: 200.
[5] Lu SK. Techniques of Acupuncture and Moxibustion.Beijing: China Press of Traditional Chinese Medicine, 2007:70-79.
[6] Wei XX. Clinical Algesiology in Chinese and Western Medicine. Beijing: China Press of Traditional Chinese Medicine, 1996: 14-15.
[7] Bayi LT, Yun H, Yan ZM.Qian Teng Bai Cao Tong Luopaste for pain of neck, shoulder and arm. Ren Ren Jiankang,2016, 35(14): 119.
[8] Tian RY, Zhang J, Xu L, Liu HL. Injecting medication into epidural space for 56 cases with pain of neck, shoulder and arm. Renmin Junyi, 2008, 51(12): 764.
[9] Yang SY, Lin XF, Liang ZF, Jiang XY, Tang K. Clinical and experimental studies of acupuncture and moxibustion for chronic pain syndrome. Xin Zhongyi, 1995, 27(6): 31.
[10] Lü XT. Discussion on clinical application ofShuacupuncture method inGuan ZhenofLing Shu. Zhongguo Zhen Jiu, 2004, 24(Z1): 38-39.
[11] Wang ZT, Peng L, Ouyang FS, Lu D, Zhong YT. Points selection and combinations of acupuncture-moxibustion for pain syndrome and action mechanisms of acupuncture analgesia. Changsha Yixueyuan Xuebao, 2007, 12(25):24-25.
[12] Liu DS. Talk about pain of shoulder and arm: analysis of 221 cases. Jing Yao Tong Zazhi, 1986, 7(1): 18-22.
[13] Zhang T, Hang Q. Modern Research and Clinic of Acupuncture and Moxibustion. Beijing: China Medical Science Press, 1998: 525-526.
[14] Lin SZ. Talk about classification of acupuncture techniques inGuan ZhenofLing Shu. Zhenjiu Linchuang Zazhi, 2008,24(7): 41-43.
[15] Cao TM, Sun Y. Clinical application of five acupuncture techniques inLing Shu. Shanghai Zhenjiu Zazhi, 1998,17(5): 35-36.
[16] Huang XF, Cao JH, Si KH, Lin HJ, Ning ZQ, Jia CW.Explore onShu-acupuncture method inNei Jing. Shaanxi Zhongyi Xueyuan Xuebao, 2013, 36(6): 24-25.
[17] Zheng KS. Acupuncture Highlights. Lanzhou: Gansu Science and Technology Press, 2009: 22-202.
[18] Shen XY. Meridians and Acupoints. Beijing: China Press of Traditional Chinese Medicine, 2002: 28-34.
[19] Wang XL. Treatment of 72 cases with talalgia byShu-acupuncture method plus Chinese herbal fumigation and washing. Jilin Zhongyiyao, 2001, 21(2): 34.
[20] Li H, Wen L, Zheng JQ. Treatment of 40 cases with numbness and pain of legs caused by lumbar intervertebral disc herniation byShu-acupuncture method at lumbar Hua Tuo Jiaji (EX-B 2) points. Guangming Zhongyi, 2013,28(11): 2348-2349.
[21] Liu CB. Observation onShu-acupuncture method plus warm needling moxibustion for 35 cases with knee osteoarthritis. Shiyong Zhongyiyao Zazhi, 2015, 31(1): 53.
猜你喜欢
Journal of Acupuncture and Tuina Science(2021年1期)2021-02-05 09:36:26
Journal of Acupuncture and Tuina Science(2020年4期)2020-08-29 02:49:56
Journal of Acupuncture and Tuina Science(2020年2期)2020-04-21 07:07:26
东坡赤壁诗词(2019年3期)2019-07-05 06:55:54
娃娃乐园·综合智能(2018年15期)2018-09-08 02:23:44
艺术品(2018年5期)2018-06-29 02:15:04
宝藏(2017年7期)2017-08-09 08:15:15
戏曲研究(2017年4期)2017-05-31 07:39:24
戏曲研究(2017年4期)2017-05-31 07:39:24
西藏教育(2016年7期)2016-03-01 21:36:58
 Journal of Acupuncture and Tuina Science2018年1期
Journal of Acupuncture and Tuina Science2018年1期
- Journal of Acupuncture and Tuina Science的其它文章
- Points selection pattern in acupuncture-moxibustion treatment of gouty arthritis: an analysis based on bibliometrics
- Analysis of points selection pattern in acupuncture treatment of sleep apnea syndrome based on data mining
- Efficacy observation on acupuncture plus moving cupping with compound white mustard oil for lumbar myofascitis
- Acupuncture plus bloodletting therapy for insomnia in blood stasis constitution: a clinical study
- Music electric stimulation of points for anxiety:a multi-center randomized controlled clinical trial
- Development of workplace-related Liver Meridian-depression scale