
Status Investigation of Outpatients Receiving Methadone Maintenance Treatment (MMT) in Shanghai from 2005 to 2016
2018-01-15 04:53:45JiayiBAOLeiZHANGZhenNINGJieFUMinZHAOJiangDU
上海精神医学 2017年6期
Jiayi BAO, Lei ZHANG, Zhen NING, Jie FU, Min ZHAO*, Jiang DU*
1. Background
Methadone as a replacement therapy drug for those with heroin addiction was put forward by Dole and Nyswander in 1965. Afterwards, western countries began to use MMT as the foremost treatment for opioid addiction, and gradually popularize the application.[1]MMT has now become one of the most effective measures to control drug abuse and prevent AIDS among heroin users.[2-3]Since 2004, MMT pilot clinics have gradually been established in China. As of May 2016, a total of 788 MMT clinics have been set up in 29 provinces.[4]Evaluation of the therapeutic efficacy administered by the first batch of 8 MMT pilot clinics[5]and the MMT clinic in Urumqi[6]showed positive functions of MMT in reducing drug use, preventing drug-related high-risk sexual activities, unlawful acts and crimes, and improving patients’ family and social functions. However, relevant surveys in recent years showed that the number of outpatients receiving MMT and the number of new outpatients showed a downward trend year by year, respectively.[7,8]
The first Shanghai MMT clinic was officially launched in Changning District in May 2005. As of now,there are 14 MMT clinics in Shanghai. In this paper, data from patients receiving MMT since 2005 in Shanghai were analyzed to understand the variations in patient numbers, maintenance treatment rate, and causes of drop out for outpatients receiving MMT, in order to provide data support for the improvement of MMT clinics in the future.
2. Subjects and methods
2.1 Subjects
The subjects of this study included a total of 7181 patients, who received maintenance treatment at each MMT clinic in Shanghai from May 2005 to June 2016, according to the Community Drug Maintenance Treatment Program for Opioids-Abuse Addicts in Shanghai. Referral MMT patients from out of Shanghai were not included, without other exclusion criteria. All the subjects’ data were from the AIDS Comprehensive Prevention and Control Data Information Management System of the China AIDS Prevention and Control Center.These data are open for use in scientif i c research, afer application to the China CDC. This study has been approved by the ethical review committee of Shanghai Municipal Center for Disease Control and Prevention.
2.2 Methods
This study was a retrospective investigation, with relevant data including demographic data (i.e. age,gender, ethnicity, education level, marital status, and employment status), dosage, outpatient number,number of new outpatients, causes of withdrawal, and treatment maintenance rate. According to the National Center for Disease Control and Prevention, outpatient maintenance rate = number of patients treated in the past month/(number of patients being treated−number of dropouts due to special reasons in the past year)*100%. ‘Special reasons’ refer to death, contraction of a rare disease, pregnancy, unlawful acts and crimes not involving drug use.
2.3 Statistical methods
Descriptive statistics using SPSS 20.0 were employed to describe demographic data, treatment maintenance rates, and number of new outpatients receiving MMT.The causes of dropout were summarized and analyzed.
3. Results
3.1 Outpatient treatment
3.1.1 Number of patients
From May 2005 to June 2016, there were a total of 7181 outpatients receiving MMT in Shanghai. There was an increase in the number of new patients from 2007-2009, with average new patient numbers exceeding 1000. After peaking in 2008, the number of new patients decreased year by year. The number of patientsincreased continuously between 2005 and 2011, with the peak in 2011 (3840 patients), and then gradually decreased, see Figure 1.

Figure 1. The flowchart of the study
3.1.2 Comparison of number of heroin-related arrests and the number of people treated by methadone treatment clinics in Shanghai (2009-2015)
From 2009-2015, the number of heroin-related arrests showed a slow downward trend in Shanghai. In 2012, the number of arrests considerably increased.Afterwards, the number continued to decrease year by year. The number of new treatments in methadone clinics was 1141 in 2009. Afterwards and until 2015,the number was <1000 each year, showing a downward trend year by year, see Figure 2.
3.1.3 Maintenance treatment rate
The maintenance treatment rate at methadone clinics in Shanghai increased year by year, from 66.1% (2008) to 84.3% (2010). Although with a slight decline in the subsequent four years, the maintenance treatment rate was stable above 80%. In 2015, the outpatient maintenance rate was 87.7%, showing good maintenance treatment effects. See Figure 3.
3.2 Patient conditions
3.2.1 Demographic characteristics
MMT clinic patients in Shanghai were primarily male(77.9%), predominantly young adults 25 to 54 years old, with below-average education, i.e. junior high school education level and below (65.4%), single (total of unmarried, divorced and widowed: 63.1%), and unemployed or underemployed (81.5%), see Table 1.
3.2.2 Dosage
Between 2008 and June 2016, the daily average number of people taking medication through Shanghai MMT clinics was 1687. In 2012, the number of people taking medication peaked, followed by a downward trend. The average daily dosage of methadone per patient was 56ml. The daily average number of MMT medication users and daily average dosage per patient in each year are shown in table 2.
In each year, the daily average number of MMT medication users exceeded 100 in Pudong New Area,Hongkou District, Xuhui District, Yangpu District,Zhabei District, Putuo District and Huangpu District,respectively. The average daily dosage of methadone per patient exceeded the Shanghai average 56ml/d in Hongkou District, Putuo District, Huangpu District,Baoshan District and Qingpu District, respectively. The average number of daily MMT medication users and average daily dose per person in each district are shown in Figure 4.
In year 2008-2015, there was a significant correlation between the maintenance rate and the average daily dosage in the methadone clinics in Shanghai (r=0.199, p<0.001).
3.2.3 Causes of dropout
Statistical data showed that, the main causes for the withdrawal from outpatient services were not collected due to an inability to follow up, see Figure 5.
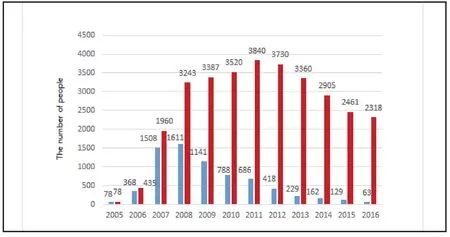
Figure 1. Number of patients in methadone maintenance clinics in Shanghai (2005-2016)
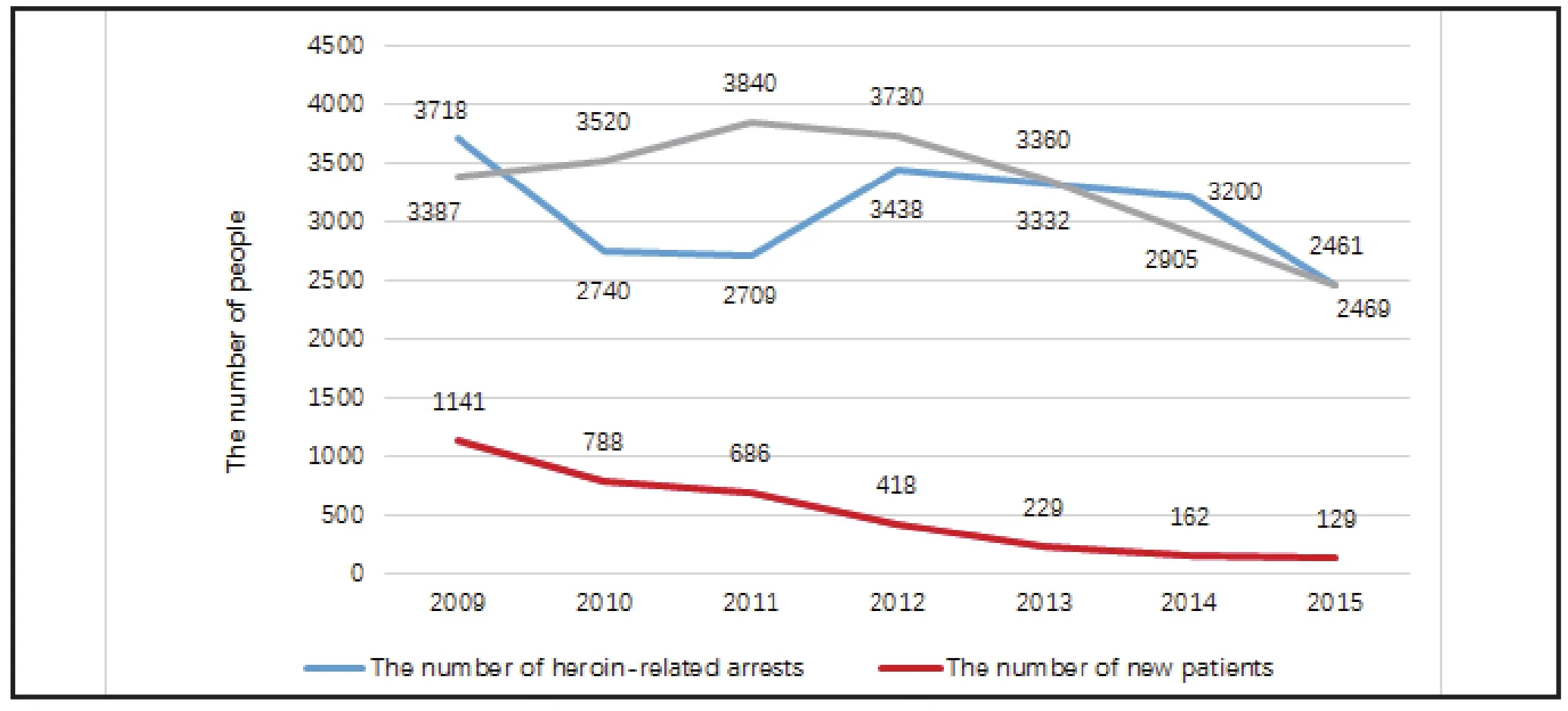
Figure 2. Comparison of number of heroin-related arrests and the number of people treated by methadone treatment in Shanghai (2009-2015)

Figure 3. The maintenance treatment rate at methadone clinics in Shanghai (2008-2015)
4. Discussion
4.1 Main findings
China began to establish MMT pilot clinics in multiple provinces and cities starting in 2004. In early years,the number of outpatients increased rapidly. In recent years, the number of MMT outpatients nationwide showed a downward trend, from 209,000 in 2012 down to 165,000 in 2016 (the National HIV AIDS Epidemic Situation and Progress of Prevention and Control Work). This study for the first time carried out descriptive analysis on the treatment work over the years for MMT clinics in Shanghai. It was found that,since the beginning of the MMT clinics in Shanghai, the clinic maintenance rate was fairly high. The number of outpatients increased initially and then decreased subsequently, which is similar to the overall trends in the country. The main causes for patient dropout were related to crime and relapse. In the meantime, it was also found in the study that there were differences in patient number and dosage of medication among the districts in Shanghai. The details are as follows.

Table 1. Demographic characteristics of outpatients receiving MMT in Shanghai
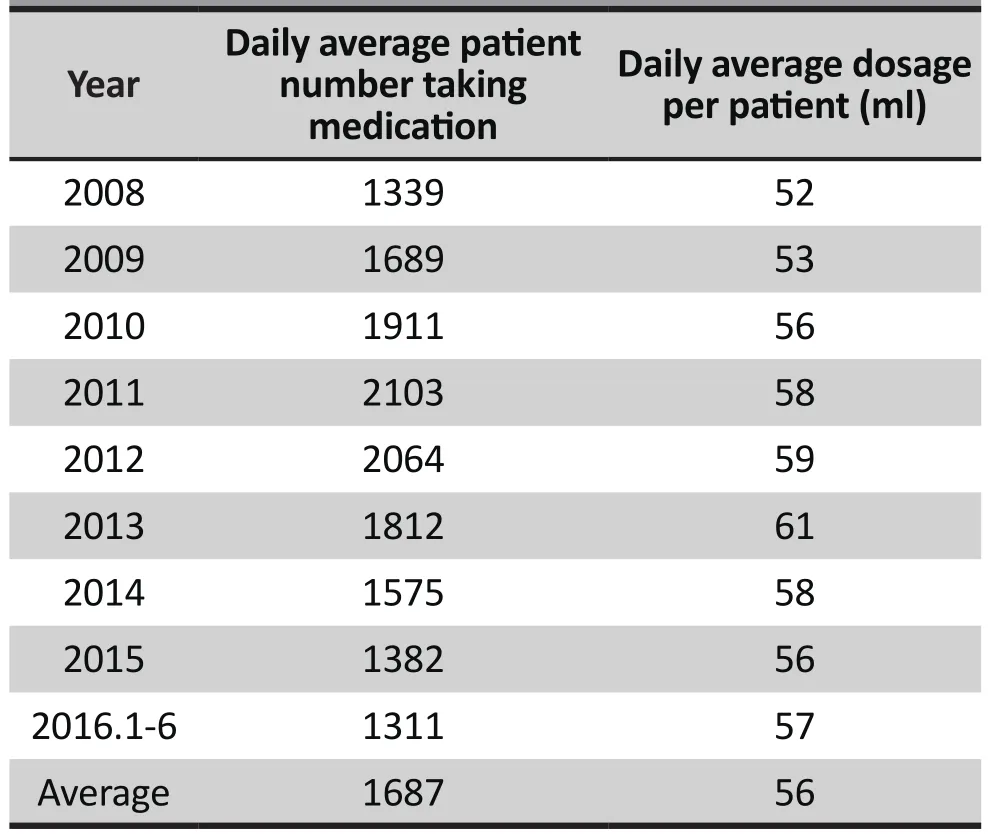
Table 2. Patients’ dosages at MMT clinics in Shanghai
First, the results showed that the number of MMT patients in Shanghai increased initially and then decreased subsequently, which was similar to the situation at MMT clinics in Wenzhou.[7]The reason may be that, at the beginning stage of clinical treatment,MMT as an effective alternative therapeutic method supported by relevant national policy was heavily publicized and promoted. The degree of acceptance of medical institutions and patients was high fairly, which led to the sharp increase in patient number during the early years of the MMT clinics between 2005 and 2008. Since 2011, MMT clinics in Shanghai showed a downward trend. The decline in patient number was possibly related to various factors. The daily cost of treatment increased the economic burden for heroin users. Convenience in access to MMT began to gradually come out.[9]Some studies found that patients with a low level of methadone awareness and those who were worried about methadone’s adverse reactions were not likely to accept MMT.[10]Improving patient awareness of methadone, through strengthened public education,was beneficial to improving the coverage rate of MMT in previous studies.[11]MMT outpatient service was an important way for patients to acquire relevant knowledge. However the staff of MMT outpatient services nationwide generally lacked psychological training, had high staff turnover[12]and job burnout.[12,13]These factors likely affect the users satisfaction with MMT clinics, and may reduce the number of those willing to seek MMT. In addition, changes in the drug abuse situation, from traditional drugs to synthetic drugs have contributed to the decline in patient numbers.
According to the national drug control report (2008-2015), among the nationwide total drug users, the percentage of heroin and other opioid users decreased significantly and showed a downward trend since 2008(77.5%). In 2014, it was less than half of all users (49.3%).The number of synthetic drug users increased rapidly year a fer year, from 6.7% in 2005 to 57.1% of the total number of drug users by the end of 2015. It is worth noting that, although there was a nationwide decrease in the number of heroin and other opioid addicts since 2008, and the number of new MMT outpatients in Shanghai had been decreasing, the number of heroin related arrests in Shanghai did not show a corresponding downward trend, see Figure 2. This suggests that the situation of heroin abuse in Shanghai was still relatively serious, and the crackdown effort was high. Nevertheless, only a small portion of patients had accepted MMT, i.e., the outpatient admission rate of MMT clinics in Shanghai was low, e.g. 6.87%, 5%,5.2% for 2013-2015 respectively (the ratio of number of new patients at MMT clinics to the number of captured heroin addicts each year in Shanghai ).
This study showed that the maintenance rate at MMT clinics in Shanghai was 66.1% in 2008, 78.1% in 2009, and had been greater than 80% since 2010. In 2015, the maintenance rate was close to 90% (87.7%). Itwas generally higher than the national average (74.9%).For example, the maintenance rate in Guizhou province between 2004 and 2012 was 74.1%.[14]The maintenance rate in Dali city, Yunnan Province was lower than 80%in the first four years of the 2008-2012 survey.[8]The factors influencing effectiveness of MMT include drug dosage, support services, medication compliance,duration of medication, and personal characteristics of individual drug users.[15]High average dosage was relevant to high maintenance rate of MMT.[16] The
average dosage in China was 45ml-55ml/d.[15]The average dosage for MMT patients in Shanghai was 56 ml/d. Over the years between 2008 and 2016, 2013 was the only year that the average dosage for MMT patients in Shanghai was greater than 60ml/d. The dosage of MMT has been controversial. Although earlier studies have shown that appropriate dosage applied to individual patients was critical to the success of MMT,[17]few patients could pass a urine test with negative results[18]if the methadone dosage was below 60mg.International studies have shown that a methadone dosage of 100mg/d was more beneficial in reducing relapse during MMT. Including Shanghai, the nationwide average MMT dosage was generally below 60 ml/d.[7,20]Due to issues such as lower surface area of Chinese ethnic groups than that of Caucasians, the administered dosage generally does not exceed 80mg/d.[20]However,the necessity of an individualized dosage with the 60 ml/d baseline according to the patients’ individual status still needs further study. It is worth noting that the difference in daily average number of MMT outpatients in different districts in Shanghai could be related to various objective factors. For example, the number of MMT outpatients in Minhang, Songjiang, and Qingpu were less. It could be related to factors such as the convenience of transportation to MMT clinics. However,in this study, it was found that there were differences in average daily dosage per patient among the districts.In Hongkou District, the dosage was the highest (62 ml/d), whereas in Songjiang District, the dosage was the lowest (40 ml/d). The inf l uencing factors and effects of average daily MMT dosage per patient have yet to be further investigated.
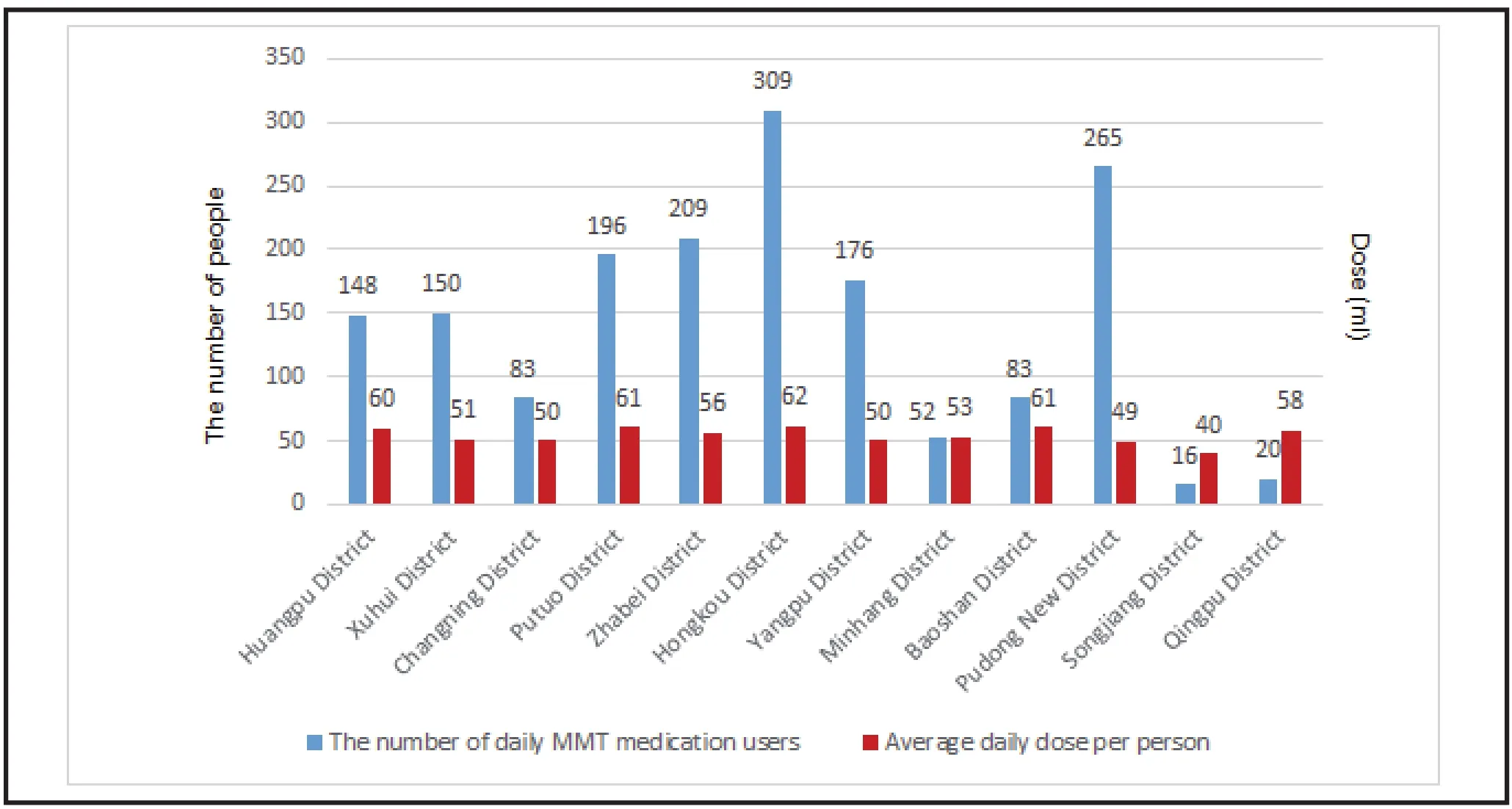
Figure 4. The average number of daily MMT medication users and average daily dose per person in each district

Figure 5. Cause for the withdrawal of outpatients from Shanghai MMT clinics
MMT clinic patients in Shanghai were primarily male, young adults, with junior-high-school-andbelow education level, single, and unemployed or underemployed. However, while investigating the marital status of MMT patients,[7,21]some studies reached different conclusions and found that married people accounted for the highest proportion of heroin users. Being married or not is one of the influencing factors affecting the quality of life for MMT patients.[22]Family is an important social support system to prevent patients from relapse. Patients with a stable marriage had a significantly higher rate of medication than patients with unstable marriage or without marriage.[23]This study showed that, except for the loss to followup cases, the main reasons for dropout at Shanghai’s MMT clinics included “non-drug related arrests” “sent to compulsory rehabilitation center due to drug use”,and “disease, pregnancy, or death”, with the percentage from high to low. This result was broadly consistent with the investigation results by Chen Hong et al. in Chongqing.[24]The withdrawal of patients from MMT medication involved many factors, such as the patient’s personal condition, environment, treatment process,and so on. With regard to the patients themselves,male patients with low educational level and short drug use time were more likely to withdraw from MMT.[24]At the same time, marital status, relationship between patients and family members, and the attitude of family members towards MMT had significant impact on patient dropout.[25]
4.2 Limitations
This study was a retrospective survey. Although descriptions were made regarding the causes of dropout and the trend of changes over the years at Shanghai’s MMT clinics in number of patients and maintenance rate, in-depth explanation of the relevant factors leading to patients’ withdrawal was lacking, due to the limitation of the available data.
Although differences in the number of patients at MMT clinics and average daily dosage per patient were found among different districts, this study had yet to find the cause of these differences. Therefore,follow-up qualitative study could be carried out, in order to explore the main reasons for the differences.In addition, this study takes Shanghai as an example.Shanghai has medical and healthcare services which are generally on a higher level than the rest of the country,so these results may not be generalizable.
4.3 Implications
MMT had positive functions[5-6]in reducing relapse,controlling the spread of drug-related HIV and other STDs, improving patient’s family and social functioning,and could effectively reduce social risks. Therefore, it is necessary to make a comprehensive analysis of the factors that affect treatment maintenance rate. This paper describes clinic and patient situations at MMT outpatient clinics since their establishment in Shanghai,and summarizes the development changes of Shanghai’s MMT clinics. It provides reliable data support for the subsequent development of relevant MMT measures.
Funding statement
National Institute of Clinical Specialties - Shanghai Mental Health Center (Office of Medical Administration,Ministry of Health) (OMA-MH 2011-873); Shanghai Education Commission High Peak and High Altitude Discipline Construction Plan (20152235)
Conflict of interest statement
The authors declare no conflict of interest related to this study
Ethical approval
This study has been approved by the ethical review committee of Shanghai Municipal Center for Disease Control and Prevention.
Authors’ contributions
Jiayi Bao: data analysis and article writing
Lei Zhang : data analysis
Zhen Ning : data support and explanation
Min Zhao : article review and modification
Jiang Du : article review and modification
1. Kuehn BM. Methadone treatment marks 40 years. JAMA.2005; 294(8): 887-889. doi: http://dx.doi.org/10.1001/jama.294.8.887
2. Feng SQ, Zhou JB, Guo YL, Shi TP, Li JH, Xu XG, et al. [Effective evaluation of community-based methadone maintenance treatment for heroin addicts]. Zhongguo Gong Gong Wei Sheng. 2010; 26(7): 924-925. Chinese
3. Feng WD, Weng YQ, Gan ZG, Bai Y. [Evaluation of AIDS prevention with risk-reducing measures among drug users in Liuzhou city]. Zhongguo Gong Gong Wei Sheng. 2010; 26(1):37-38. Chinese
4. Chinese Disease Prevention and Control Center. [Update on the AIDS/STD epidemic in China and main response in control and prevention in May, 2016]. Zhongguo Ai Zi Bing Xing Bing. 2016; 7: 487-487. Chinese
5. Pang L, Mi GD, Wang CH, Luo W, Rou KM, Li JH, et al.[Evaluation of first 8 pilot methadone maintenance treatment clinics in China]. Zhong Hua Shi Yan He Lin Chuang Bing Du Xue Za Zhi. 2007; 21(1): 2-4. Chinese
6. Liu JB, Dilixiati. YHF, Li F, Zhang F, Mo LR, Jiao LD, et al.[The Effective Evaluation of the Methadone Maintenance Treatment of Heroin Addicts]. Zhongguo Yao Wu Lan Yong Fang Zhi Za Zhi. 2007; 13(1): 10-13. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1006-902X.2007.01.004
7. Zhao LN, Wang DY, Ye ZM, Jin Q, Su DH, Wang RQ, et al.[Development status of methadone maintenance treatment in Wenzhou City, 2004-2013]. Xian Dai Yu Fang Yi Xue. 2015;42(13): 2434-2436
8. Li HY, Wang QL, Fang YH, Ji SL. [Analysis of Methadone Continuous Treatment Status in Dali from 2008 to 2012]. Dali Xue Yuan Xue Bao. 2014; 13(4): 67-70. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1672-2345.2014.04.021
9. Jiang HF, Du J, Wang ZH, Wu F, Hser YI, Zhao M. [The effect of comprehensive interventional strategy of psychosocial and medical treatment on the rate of methadone maintenance treatment]. Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2010; 5.Chinese
10. Li YF, Yao WW, Xia CY. [Qualitative study on methadone maintenance treatment of heroin addicts in Qingpu district of Shanghai]. Shanghai Yu Fang Yi Xue. 2016; 28(6): 385-387.Chinese
11. Zhang YH, Liu Y, Li LH, Huang YY, Xu J, Wang HY. [Correlation factors influencing the effect and countermeasures of methadone maintenance treatment]. Zhongguo Yao Wu Lan Yong Fang Zhi Za Zhi. 2011; 17(2): 69-72. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1006-902X.2011.02.003
12. Li JH, Zhang RM, Zhang B, Zhang CB. [Human resource development research on methadone maintenance treatment in China]. Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2013; 22(1): 64-68. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1007-9718.2013.01.016
13. Yang LP, Zhang B, Wang H, Li JH. [Investigation of burnout and related factors of methadone maintenance treatment clinic staff]. Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2014; 1: 60-64. Chinese
14. Fan L, Shen LM, Zhan L. [Survey on the operation of methadone maintenance treatment in Guizhou province].Zhongguo Yao wu Lan Yong Fang Zhi Za Zhi. 2013; 19(5):260-263. Chinese
15. Li XL, Tan HZ, Sun ZQ. [Research Progress on the inf l uencing factors of methadone maintenance treatment]. Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2009; 18(1): 7-9. Chinese
16. Shi S, Huang YS, Li X, Zheng X, Huang HF, Ye YG. [Correlation factors influencing the effect of methadone maintenance treatment]. Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2008; 17(1):56-61. Chinese
17. Blaney T, Craig R J. Methadone maintenance. Does dose determine differences in outcome? J Subst Abuse Treat.1999; 16(3): 221-228. doi: http://dx.doi.org/10.1016/S0740-5472(98)00031-2
18. Guo S. [Methadone maintenance treatment program].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2001; 10(2):91-94. Chinese. doi: http://dx.doi.org/10.3969/j.issn.1007-9718.2001.02.005
19. Donny EC, Walsh SL, Bigelow GE, Eissenberg T, Stitzer ML.High-dose methadone produces superior opioid blockade and comparable withdrawal suppression to lower doses in opioid-dependent humans. Psychopharmacology. 2002;161(2): 202-212. doi: http://dx.doi.org/10.1007/s00213-002-1027-0
20. Mao XY, Li T, Gong Y, Mou JF. [Survey on the operation of methadone maintenance treatment in Sichuan province].Zhongguo Yao Wu Yi Lai Xing Za Zhi. 2011; 20(2): 141-144.Chinese
21. Wang J, Liu GW, Zhao YJ, Xia DY, Lu HY, He X. [A study on dropping-out rate and associated factors of patients with methadone maintenance treatment in Beijing from 2010 to 2014]. Zhong Hua Ji Bing Kong Zhi Za Zhi. 2016; 20(8): 777-780. Chinese. doi: http://dx.chinadoi.cn/10.16462/j.cnki.zhjbkz.2016.08.006
22. Lu HY, Feng QM, Li YN, Luo HY, Chen HH, Zhang YX, et al.[Quality of life and its influencing factors among patients with methadone maintenance treatment]. Zhongguo Gong Gong Wei Sheng. 2014; 30(11): 1438-1440. Chinese. doi:http://dx.chinadoi.cn/10.11847/zgggws2014-30-11-23
23. Su YL, Pan Q, Zhang C, Tang YX, Xiao ZD, Su H, et al.[Research of the Effect of Marriage Status of Methadone Maintenance Treatment Patients on Medicine-taking Maintenance Rate]. Zhongguo She Hui Yi Xue Za Zhi.2016; 33(6). Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1673-5625.2016.06.030
24. Chen H, Wu GH, Wang XX. [Dropping out situation in patients with methadone maintenance treatment and its inf l uence factors]. Xian Dai Yi Yao Wei Sheng. 2016; 32(11):1612-1614. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1009-5519.2016.11.004
25. Fan JC, Huang B, Ma Q, Sun HB. [Analysis of factors associated with dropout of methadone maintenance treatment in Guiyang]. Zhong Hua Ji Bing Kong Zhi Za Zhi.2015; 19(12): 1215-1219. Chinese. doi: http://dx.chinadoi.cn/10.16462/j.cnki.zhjbkz.2015.12.008

- 上海精神医学的其它文章
- Comparisons of Superiority, Non-inferiority, and Equivalence Trials
- Analysis of Family Functioning and Parent-Child Relationship between Adolescents with Depression and their Parents
- CHN2 Promoter Methylation Change May Be Associated With Methamphetamine Dependence
- The Relationship between the Lifestyle of the Elderly in Shanghai Communities and Mild Cognitive Impairment
- Meta-analysis of the Eff i cacy and Safety of Repetitive Transcranial Magnetic Stimulation (rTMS) in the Treatment of Depression
- Senile Depression with Somatization Symptoms and Insomnia is Diagnosed as Multiple System Atrophy: A Case Report