
A study of the characteristics of alexithymia and emotion regulation in patients with depression
2017-11-29 03:16HaoZHANGQingFANYanSUNJianyinQIULishengSONG
上海精神医学 2017年2期
Hao ZHANG, Qing FAN, Yan SUN, Jianyin QIU*, Lisheng SONG*
•Original research article•
A study of the characteristics of alexithymia and emotion regulation in patients with depression
Hao ZHANG, Qing FAN, Yan SUN, Jianyin QIU*, Lisheng SONG*
depression; alexithymia; emotion regulation; emotion reappraisal; emotion suppression
1. Introduction
Depression is a common mood disorder which is characterized by significant and lasting depressive mood, lack of internal vitality or losing interest in things.[1]The characteristics of depression are a high prevalence, high recurrence rate, high disability rate and high suicide rate; and the incidence of disease is around 10% (WHO, 2002). Epidemiological investigations in China have shown that the point prevalence is 6.1% to 7.5%.[2] Recently, the prevalence of depression has been climbing every year, and it is estimated that by 2020 depression will be ranked number one in China’s burden of disease. Depression causes severe impairments in an individuals’ emotions,cognitive ability, behavior and physical development,and can lead to a decrease in social functioning, bring about a heavy economic burden and affect the normal order of family life.[3]
The cause of depression still remains unclear.Biological and psychological social factors both significantly affect the incidence of depression.According to the social cognition theory, depression is the result of an interaction between cognitive psychological factors and stress. Cognitive psychological factors include an individual’s traits, concept of the self, cognitive appraisals, attribution and coping styles,and so forth; and these are all likely correlated with susceptibility to depression.
Alexithymia is a cognitive processing and regulation disorder in emotions, and its symptoms are having difficulty in recognizing and describing emotions, in distinguishing emotional and physical perceptions, and lacking externally oriented thinking. Clinical research has shown that the incidence of alexithymia in patients with depression is significantly higher than that of the general population.[5]However, the mechanism of alexithymia in patients with depression is still unclear. Some researchers suggest that alexithymia is a personality trait, and it is a predisposing factor for depression,[6]while other researchers view alexithymia as a state reaction to depression[7-8](i.e. a defense mechanism).[9]
Emotion regulation is an individual’s monitoring and regulation process for the internal processing and external presentation of emotions. It has an adaptive function, and it is an individual trait. There are different kinds of emotion regulation. According to one theory,there is antecedent-focused emotion regulation and response-focused emotion regulation. Antecedentfocused emotion regulation is referred to as regulating the causes of emotions (e.g., cognitive reappraisal);while response-focused emotion regulation is regulating the emotions which have already emerged on the emotional expression level (e.g., expression suppression). Currently, it is generally accepted that cognitive reappraisal is an adaptive emotion regulation strategy, while expression suppression is a nonadaptive emotion regulation strategy. Previous research indicates that in comparison with healthy controls,patients with depression are more inclined to employ non-adaptive emotion regulation strategies than to use adaptive emotion regulation strategies spontaneously.[10]This phenomenon applies to the patients with depression in both active and remissive phases.[11]To this day, there is little research utilizing experimental methods to evaluate depressive patients’ ability to employ different emotion regulation strategies (e.g.,cognitive reappraisal and expression suppression).
The present study aims to further explore the characteristics of alexithymia in patients with depression, and the relationships between depressive symptoms, alexithymia and individual emotion regulation ability.
2. Methods
2.1 Subjects
2.1.1 Depression group
Subjects in this group were recruited through the recommendations of nurses, the diagnoses of doctors and other methods in the outpatient department of Shanghai psychological consultation and treatment center, and they were recruited from May to September in 2016.
The inclusion criteria were the following: (a)meeting diagnostic criteria for depression according to the DSM-IV; (b) ratings of no less than 20 on the Hamilton Depression Scale-24 (HAMD-24); (c) age range from 18 to 55; (d) female or male; (e) education level being no less than junior high; (f) visual and auditory senses were good enough to complete the examinations; (g) provided written informed consent to participate in the study. The exclusion criteria were the following: (a) previous brain injury or history of stroke;(b) currently suffering from a severe medical condition;(c) having severe risk of suicide or self-injury; (d)currently pregnant or lactating; presence of comorbid psychotic disorder, psychotic symptoms, psychoactive substance dependency or abuse, personality disorder,or mental retardation.
In total thirty-six patients with depression were included in the present study, including 6 males and 30 females. The mean(sd) age was 27.33 (7.26), and 33(91.7%) of them had a college education or higher.
2.1.2 Control group
All participants in the control group were recruited via advertisements and social contacts. The inclusion criteria were the following: (a) individuals who were determined as having no mental disorders after being evaluated by psychiatrists; (b) HAMD-24 scores less than 8; (c) Hamilton Anxiety Scale (HAMA) scores less than 6; (d) aged from 18 to 55; (e) female or male; (f)junior high school education or higher; (g) no history of taking psychiatric drugs; (h) no family history of mental disorders; (i) visual and auditory senses were good enough to complete the examinations; (j) providing written informed consent to participate in this study.
Exclusion criteria were the following: (a) individuals with risk of self-injury or suicide; (b) currently suffering from a severe medical condition or central nervous system disease; (c) current substance abuse;(d) pregnant or lactating women. Thirty-one healthy volunteers were included in the control group,including 4 males and 27 females. The mean(sd) age was 27.2 (6.4), and 28 (90.3%) of them had a college education or more.
2.2 Assessment tools
HAMD-24 and HAMA were employed to evaluate the depression and anxiety levels of participants. Toronto Alexithymia Scale (TAS) was used to evaluate the degrees of alexithymia.
The computer emotion regulation experiment programmed with E-Prime was employed to measure the emotion regulation ability. This experiment procedure was programmed by the researchers in the Institute of Psychology at the Chinese Academy of Sciences. It was provided by Chuqiao Chen and Yi Wang, and was operated under their supervision.
Seventy-two pictures were presented in the experiment, with 18 neutral emotion pictures and 54 negative emotion pictures. The negative emotion pictures were divided into three groups with 18 pictures in each group, and manipulated in three conditions. There were four conditions in total:neutral pictures-watched freely, negative pictureswatched freely, negative pictures-cognitive reappraisal and negative pictures-expression suppression. Their abbreviations were watch-neutral, watch-negative,negative-reappraisal, and negative-suppression. The four conditions were presented randomly.
Before the experiment began, the subjects were informed that there were neutral and negative pictures in the experiment with most of them being negative. There were three cues during the experiment: “watch freely”, “cognitive reappraisal”and “expression suppression”. “Watch freely” was referred to as watching the picture naturally. “Cognitive reappraisal” meant understanding the pictures that caused negative emotions in a more positive way. For example, the pictures that induce negative emotions can be comprehended as movies’ special effects instead of real situations, or can be explained as something irrelevant to themselves. “Expression suppression” was controlling their facial expressions and refraining from expressing the negative emotions when they saw the unpleasant pictures.
Ten negative emotion pictures were prepared as a practice for the participants. These pictures were not presented in the formal experiments. They were presented to the participants one by one. The experimenter used the first two as examples to explain how to perform cognitive reappraisal, and the participants practiced cognitive reappraisal orally by themselves with the remaining images until they were proficient in performing this task.
After the experiment began, a cue was presented on the screen for two seconds, which was either“watch freely”, “cognitive reappraisal” or “expression suppression” tasks. Then a neutral or negative picture was presented on the screen for ten seconds. During this period, according to the cue, the subjects eitherwatched the picture naturally or regulated their emotions with the emotion regulation strategies that they just learned (i.e., cognitive reappraisal and expression suppression). Following this, a rating interface was presented. The subjects were requested to rate the intensity of their emotions at that moment on a scale of 1 to 7. The lowest emotional intensity was 1; while the highest was 7. The subjects were supposed to react by pressing buttons on the keyboard.The rating interface was presented for four seconds.It would not disappear after the subjects pressed the button, and it would go to the next interface automatically after four seconds if the subjects did not press any buttons. Then a cue saying “relax” was presented for four seconds, which allowed the subjects to relax for a bit. Then another experiment would continue to other blocks with the same procedure. The total duration of the experiment was 24 minutes with one break during the whole time.

Figure 1. Flowchart of the study
2.3 Statistical methods
SPSS 17.0 statistics software package was used to conduct statistical analysis. The main statistical methods included descriptive statistical methods, χ2tests,independent sample t tests, and Pearson correlation analysis. Statistical significance was set at p<0.05.
3. Results
3.1 Demographic characteristics of the participants and the clinical features of the patient group
Thirty-six depressive patients were enrolled into the present study, including 6 males and 30 females. The mean (sd) age was 27.3 (7.3) years old, and 33 (91.7%)of them had a college education or more. There were 31 healthy volunteers in the control group, including 4 males and 27 females. The mean (sd) age was 27.2(6.4), and 28 (90.3%) of them had a college education or more. There were no significant differences between two groups’ in gender (χ2=0.186, p=0.666),educational level (χ2=0.037, p=0.848) and age(t=0.102, p=0.919).
The patient group mainly consisted of newly diagnosed female patients with depression. The onset of depression was mostly during adolescence, and most of them had not received any systematic medical treatment or psychological therapy in the past. The mean (sd) score on HAMD-24 was 27.78 (5.78), and the mean (sd) score on HAMA was 19.28 (5.52).
3.2 The comparison of TAS scores between the two groups
The ratio of individuals with alexithymia in the patient group was 66.67%, while that in the control group was 3.23%. The difference between two ratios was significant (χ2=28.661, p<0.001). The total scores of TAS in the patient group were significantly higher than those in the control group (t=7.378, p<0.001). The patient group was significantly higher than the control group in scores reflecting having difficulty recognizing one’s own emotions factor (t=7.182, p<0.001),having difficulty describing one’s own emotions factor(t=6.688, p<0.001) and externally oriented thinking factor (t=3.337, p<0.001). See table 1.
3.3 Comparison of the emotion regulation experiment results between the two groups
Among the 36 subjects in the patient group, 27 of them completed the emotion regulation experiment.The rest dropped out of the experiment due to feeling uncomfortable while watching the negative pictures,the relatively long duration of the experiment and other reasons. Among the 31 subjects in the control group, 30 of them finished the experiment; while one quit due to not being able to use a computer. The data of one healthy control group member was lost due to the experimenter’s operational error. Therefore,the data for 27 subjects in the patient group and 29 subjects in the control group were collected in total.
There were no significant differences between two groups under the negative-watch, negative-reappraisal and negative-suppression conditions. But the patient group’s scores under neutral-watch condition was significantly higher than those of the control group(t=2.080, p=0.043). See Table 2.
After comparing the patient group’s scores under four conditions, it was found that the score under the negative-watch condition was significantly higher than that under neutral-watch condition (t=11.160, p<0.001),negative-reappraisal condition (t=4.652, p<0.001) and negative-suppression condition (t=3.857, p=0.001). The score under negative-reappraisal was not significantly different from that under the negative-suppression condition (p=0.279). After comparing the control group’s scores under four conditions, it was shown that the score under negative-watch was also significantly higher than that under neutral-watch condition (t=14.558, p<0.001),negative-reappraisal condition (t=5.042, p<0.001) and negative-suppression (t=4.631, p<0.001). The scores under negative-reappraisal and negative-suppression conditions were not significantly different from each other (p=0.225). See Table 3.
3.4 Correlations of the scores of HAMD-24, HAMA and TAS in the patient group
In the patient group, the TAS total score had significant positive correlations with the HAMD-24 total score (Pearson correlation coefficient (r) was 0.388, p=0.019) and the HAMA total score (Pearson correlation coefficient (r) was 0.379, p=0.023). The score measuring having difficulty recognizing own emotions factor was positively correlated with theHAMD-24 total score (Pearson correlation coefficient (r)was 0.491, p=0.002) and the HAMA total score (Pearson correlation coefficient (r) was 0.465, p=0.004) which statistically significant. See Table 4.

Table 2. Comparison of emotion regulation experiments’ scores between the patient group and the control group
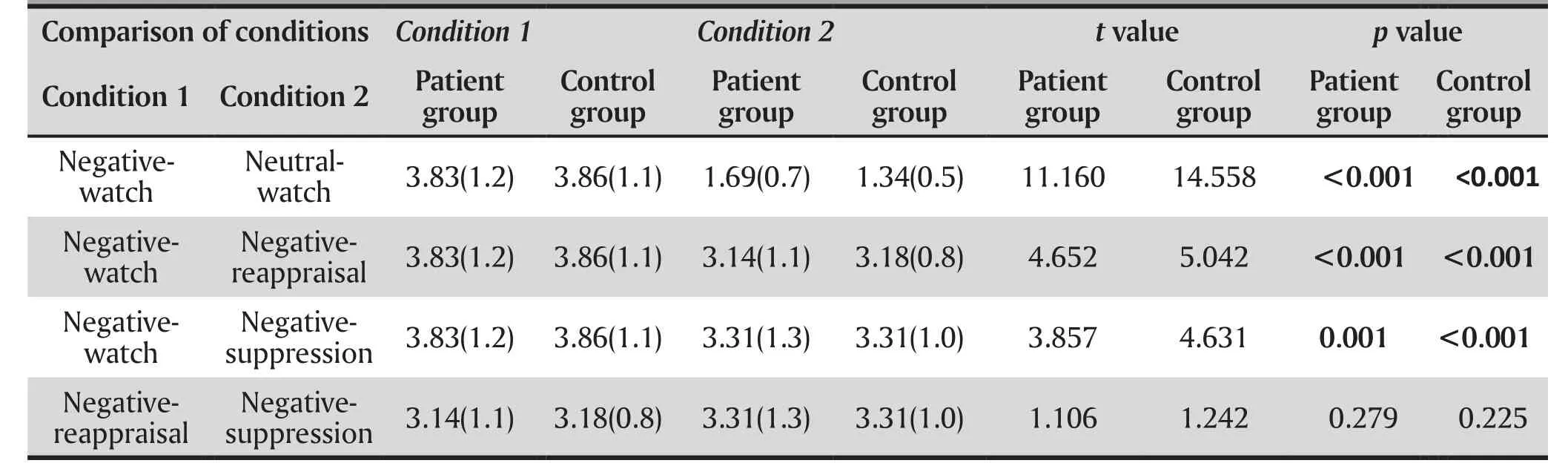
Table 3. The comparison of the scores of four emotion regulation conditions between the patient group(n=27) and the control group (n=29)
3.5 Correlations of the scores of HAMD-24, HAMA,TAS and the emotion regulation experiment in the patient group
In the patient group, the scores of the emotion experiment, HAMD-24, HAMA and TAS were not correlated with each other significantly. See Table 5.
4. Discussion
4.1 Main findings
According to the results of the present study, the rate of incidence of alexithymia in the patient group was 66.7%, which was significantly higher than that of the control group (3.2%). It indicates that depressive patients are more likely to have alexithymia than the general population. Generally speaking, patients with depression showed more obvious symptoms of alexithymia, such as having difficulty recognizing and describing their own emotions, paying more attention to the details of the external world than inner experiences and so forth; and this is in accordance with the findings of previous studies.[12-13]
Previous studies indicate that the severity of alexithymia might be affected by gender, education level, the severity of depression and other factors.[14]Meanwhile, the degree of depression and the severity of somatization symptoms might also be affected by the severity of alexithymia.[15]Supporting this point of view,the present study’s result demonstrates that the TAS total score of depressive patients has a significant positive correlation with their depression and anxiety levels.

Table 4. Pearson correlations of HAMD-24, HAMA, TAS total scores and factor scores in patients with depression

Table 5. Correlations of HAMD-24, HAMA total scores, TAS total scores, factor scores and the scores of four emotion regulation experiments in patients with depression
It has been found that in the clinical and normal groups, alexithymia and its factors have relatively high stability.[16]This suggests that alexithymia might be a personality trait or a predisposing factor of depression.[6]However, other scholars propose that alexithymia is a state reaction of depression. According to Haviland and colleagues’ study, alexithymia is a kind of defense mechanism for patients.[17]In the patient group of the present study, most of the subjects were young females with mild to moderate depression, who had a relatively high education, were being diagnosed with depression for the first time and had received no psychiatric or psychological treatment. These features may have affected their degrees of alexithymia. Based on the information collected during the recruitment interviews and results of the present study, alexithymia might be a relatively stable personality trait, which is probably a predisposing factor for depression. When facing a stressful event, individuals with alexithymia employ response-focused emotion regulation instead of using antecedent-focused emotion regulation automatically, because it is common for them to have difficulty recognizing their own emotions. Responsefocused emotion regulation is regulating the results of emotions, which is suppressing emotions; so it is not an effective method of truly regulating negative emotions.Therefore, it is possible that alexithymia influences individuals’ depression levels as an emotion cognitive processing and regulation defect. However, based on the data of the emotion regulation experiment,we did not find any correlation between depressive patients’ emotion regulating ability and the severity of alexithymia. The reason for this phenomenon could be that alexithymia is correlated with the emotion regulation methods which individuals tend to employ in real life. By contrast, the subjects were asked to consciously employ specific strategies to regulate emotions according to the experimenter’s requests.This is an important ability, but it might be irrelevant to alexithymia.
The results of the emotion regulation experiment have shown that negative pictures evoked depressive patients’ negative emotions effectively, and after learning, depressive patients were able to employ cognition reappraisal and expression suppression emotion regulation strategies to regulate negative emotions successfully under guidance. The regulation effects of two strategies were not different from each other. The control group showed the same results.Some previous studies had similar findings. For example, Erk and colleagues suggest that patients with depression can reduce the intensity of negative emotions through cognition reappraisal, but emotion regulation is not consistent.[18]
After comparing two groups’ data, we found that the patient group’s scores were significantly higher than those of the control group while they were watching the neutral pictures, and this could be because depressive patients were more sensitive and their emotions were evoked more easily. But while they were watching negative pictures and rating them with cognitive reappraisal and expression suppression, there was no significant difference between the two groups.Patients with depression showed the same emotional regulation ability as the healthy controls. Findings from some previous studies are consistent with this result,while others are not. For instance, in 2010, Ehring and colleagues suggested that rehabilitated depressive patients were able to utilize a cognitive reappraisal strategy to regulate negative emotions effectively under guidance. The results of this emotional regulation strategy were similar to those seen in the general population.[19]However the results of a study by Zhang and colleagues in 2016 were different than those reported by Ehring. They found that patients with mild to moderate depression could employ cognitive reappraisal strategy under guidance, but the effect was worse than that for non-depressed subjects.During cognitive reappraising, the amplitude of LPP wave generated by patients with depression reduced,but it was still greater than that seen in non-depressed subjects.[20] In the present study, the participants’ mean score on the HAMD-24 was 27.8, which is closer to the results of Zhang and colleagues’ study. The reason for this difference could be that nine subjects in the patient group in our study dropped out due to not being able to endure negative pictures, hence only patients with better emotion regulation ability completed this experiment.
This study is different from previous research done on this topic. It explored depressive patients’ two emotional regulation abilities: cognitive reappraisal and expression suppression. Cognitive reappraisal plays a role in the early stage of emotion generation;while expression suppression affects the late stage of emotion generation.[21]It was found that depressive patients’ scores in the emotion regulation experiment were irrelevant to their levels of depression and anxiety.In the present study, patients with depression showed the same emotional regulation ability as the normal controls did, even though not all subjects completed the experiment. But it can be interpreted that some patients with depression may have maintained relatively good emotional regulation ability. With some guidance and practice, this ability can be fully utilized. Moreover, this ability may not be influenced by patients’ alexithymia or depressive symptoms. This may help explain why psychological therapies that teach depressive patients to self-regulate emotions, such a cognitive behavioral therapy, are effective.
4.2 Limitations
There are several limitations of the present study. First of all, the sample size is relatively small, and most participants in the patient group were highly-educated female patients with depression. Therefore, we need to be cautious about explaining the results of this study and generalizing the findings. Secondly, nine of the participants (i.e. 25% of the total sample) did not finish the emotional regulation experiment. It has affected the results to a certain degree.
4.3 Implications
Depression is a common mental illness. As society develops, the economic and psychological impact of depression also appears to be growing. In China,psychological therapies to treat depression are becoming more widely used. Psychological therapies can be improved by further understanding the characteristics of alexithymia and emotional regulation strategies of patients with depression. Understanding these issues can also aid patients in gaining insight the way they perceive their emotions, which can be useful in the treatment and relapse prevention of depression.
Acknowledgement
Many thanks to Professor Chuqiao Chen, Professor Yi Wang, Dr. Lanlan Wang of the Shanghai Psychological Consultation and Treatment Center, Dr. Yanle Bai, Dr.Weijun Chen, Dr. Junhan Yu, Dr. Yanru Wu, Dr. Jingjing Huang, Dr. Lan Cao, Dr. Han Chen and Head-nurse Jin Dang for providing help on the present study.
Funding
Funding provided by the Shanghai Mental Illness Medical Center cultivation project; national clinical priority project– Shanghai Mental Health Center(Department of Health Administration 2011-873):Treatment effect of mindfulness on depressive patients with comorbid borderline personality disorder and fMRI before and after treatment comparison study.
Ethical approval
The present study was approved by the Shanghai Mental Health Center ethics committee. All participants provided written informed consent to participate in this study.
Conflict of interest statement
Authors declare no conflict of interest related to this manuscript.
Authors’ contribution
Hao Zhang: scales ratings, carrying out the experiments, data analysis, article writing and revision Jianyin Qiu: study design, screening, data analysis and article revision
Lisheng Song: screening, data analysis and article revision
Qing Fan: study design and screening
Yan Sun: screening
1. Li ZJ. [Clinical Psychology]. Beijing: People’s Medical Publishing House; 2014. p: 93-94. Chinese
50多个国家和地区,4000多名世界顶级舞者,齐聚美国凤凰城,嘉琪是年纪最小的参赛选手。当她出现在比赛现场时,人群中的高手们都一脸质疑,甚至有人直接走过来,拿手在嘉琪的脑袋前比划了两下,“意思是说我很矮。”嘉琪没有生气,也丝毫不怯场,在场外的battle(对抗)环节中,跟着音乐来了一场freestyle(即兴发挥),结果让本来一脸轻视的围观舞者,心服口服地为这个中国小学生欢迎鼓掌;等到真正比赛时,她拿着一个粉色的保温杯就上台了,先是向台下深深地鞠一躬,乖巧的样子,丝毫没有斗舞的气势。
2. Phillips MR, Zhang J, Shi Q, Song Z, Ding Z, Pang S, et al.Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-2005: An epidemiological survey. Lancet. 2009;373: 2041-2053. doi:http://dx.doi.org/10.1016/s0140-6736(09)60660-7
3. Kelly BD, Nur UA, Tyrer P, Casey P. Impact of severity of personality disorder on the outcome of depression.Eur Psychiatry. 2009; 24(5): 322-326. doi: http://dx.doi.org/10.1016/j.eurpsy.2008.12.004
4. Ramel W, Goldin PR, Eyler LT, Brown GG, Gotlib IH, McQuaid JR. Amygdala reactivity and mood-congruent memory in individuals at a risk for depressive relapse. Biol Psychiatry.2007; 61: 231-239. doi: http://dx.doi.org/10.1016/j.biopsych.2006.05.004
5. Honkalampi K, Hintikka J, Tanskanen A, Lehtonen J,Viinamäki H. Depression is strongly associated with Alexithymia in the general population. J Psychosom Res.2000; 48(1): 99. doi: http://dx.doi.org/10.1016/s0022-3999(99)00083-5
6. Saarijarvi S, Salmineb JK, Toikka TB. Alexithymia and depression. A 1-year follow-up study in outpatients with major depression. J Psychosom Res. 2001;51: 729-733. doi:http://dx.doi.org/10.1016/s0924-9338(02)80566-1
7. Honkalampi K, Saarinen P, Hintikka J, Virtanen V, Viinamäki H. Factors associated with Alexithymia in Patients suffering from depression. Psychother Psychosom. 1999;68: 270-275.doi: http://dx.doi.org/10.1159/000012343
8. Zhang JX, Yang QL. [Correlation study of alexithymia,depression and anxiety of patients with depression].Zhongguo Jian Kang Xin Kang Xue Za Zhi. 2007;15(6):492-493. Chinese. doi:http://dx.chinadoi.cn/10.3969/j.issn.1005-1252.2007.06.007
9. Haviland MG, Mac Murray JP, Cummings MA. The relationship between Alexithymia and depressive symptoms in a sample of newly abstinent alcoholic inpatients.Psychother Psychosom. 1988;49: 37-40. doi: http://dx.doi.org/10.1159/000288065
11. Ehring T, Fischer S, Schnulle J, Bosterling A, Tuschen-Caffier B. Characteristics of emotion regulation in recovered depressed versus never depressed individuals. Pers Individ Dif. 2008;44: 1574-1584. doi: http://dx.doi.org/10.1016/j.paid.2008.01.013
12. Zhu XZ, Hu SY, Yi JY, Yao SQ, Men LX. [The alexithymia of patients with depressive episode]. Zhongguo Xing Wei Yi Xue Ke Xue. 2005;12(4): 1073-1074. Chinese. doi: http://dx.chinadoi.cn/10.3760/cma.j.issn.1674-6554.2005.12.007
13. Honkalampi K, Hintikka J, Tanskanen A, Lehtonen J,Viinamäki H. Depression is strongly associated with Alexithymia in the general Population. J Psychosom Res.2000;48(1): 99. doi: http://dx.doi.org/10.1016/s0022-3999(99)00083-5
14. Hu CF, Li W, Reng QL, Zhang JX, Zhang Z. [A multianalysis on the influencing factors contributing to alexithymia of patients with depression in period of onset]. Jing Shen Yi Xue Za Zhi. 2010;23(1): 13-15. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1009-7201.2010.01.005
15. Tang QP, Zhang YT, Zhu XZ. [Effect of alexithymia on depressive symptoms]. Zhongguo Xing Wei Yi Xue Yu Nao Ke Xue Za Zhi. 2011;20(6): 545-546. Chinese. doi: http://dx.chinadoi.cn/10.3760/cma.j.issn.1674-6554.2011.06.021
16. Luminet O, Rime B, Bagby RM, Taylor GJ. A multimodal investigation of emotional responding in alexithymia.Cogn Emot. 2004;18(5): 741-766. doi: http://dx.doi.org/10.1080/02699930341000275
17. Haviland MG, Mac Murray JP, Cummings MA. The relationship between Alexithymia and depressive symptoms in a sample of newly abstinent alcoholic inpatients.Psychother Psychosom. 1988;49: 37-40. doi: http://dx.doi.org/10.1159/000288065
18. Erk S, Mikschl A, Stier S, Ciaramidaro A, Gapp V, Weber B, et al. Acute and sustained effects of cognitive emotion regulation in major depression. J Neurosci. 2010;30(47): 15726-15734. doi: http://dx.doi.org/10.1523/jneurosci.1856-10.2010
19. Ehring T, Tuschen-Caffier B, Schnülle J, Fischer S, Gross JJ. Emotion regulation and vulnerability to depression:Spontaneous versus instructed use of emotion suppression and reappraisal. Emotion. 2010;10(4): 563-572. doi: http://dx.doi.org/10.1037/a0019010
20. Zhang K, Wang CM, Wang JX. [The Effect of Reappraisal and Distraction for Patients of Depression: ERPs Study]. Xin Li Xue Tan Xin. 2016;36(3): 245-250. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1003-5184.2016.03.010
21. Goldin PR, McRae K, Ramel W, Gross JJ. The neural base of emotion regulation: Reappraisal and suppression of negative emotion. Biol Psychiatry. 2008;63: 577-586. doi:http://dx.doi.org/10.1016/j.biopsych.2007.05.031
抑郁症患者的述情障碍特征及情绪调节研究
张灏,范青,孙岩,仇剑崟,宋立升
抑郁症;述情障碍;情绪调节;认知重评;表达抑制
Background:Even though patients with depression often show significant alexithymia, the underlying mechanism of their alexithymia remains unclear. Furthermore, few experimental studies have explored their ability to regulate emotions.
Objective:To explore the characteristics of alexithymia in patients with depression, and the relationship of depressive symptoms, alexithymia and emotion regulation.
Methods:A total of 36 patients with depression and 31 healthy controls were enrolled. HAMD-24 and HAMA were used to evaluate depressive and anxious symptoms. Toronto Alexithymia Scale (TAS) was employed to assess alexithymia. A computer experiment was used to evaluate emotion regulation.
Results:66.67% of the patients with depression were considered as having alexithymia, but the rate in the control group was only 3.23%. The rates showed a significant difference (χ2=28.661, p<0.001).The score of TAS was higher in patients with depression than healthy controls (t=7.378, p<0.001).In a computerized emotional regulation experiment, under watch-neutral conditions, the emotion experience ratings of patients with depression were higher than those of controls (t=2.080, p=0.043);while under watch-negative, negative-reappraisal and negative-suppression conditions, the ratings of patients with depression showed no difference from those of the controls. The scores of TAS were correlated with the HAMD-24 scores and the HAMA scores significantly in patients with depression.However, the ratings on the emotional regulation experiment had no correlation with the HAMD-24 scores, the HAMA scores or the TAS scores.
Conclusion:The incidence of alexithymia is higher in patients with depression than the general population. The depressive symptoms may have interplay with alexithymia in patients with depression.Emotion regulation ability may be an independent trait and have nothing to do with the depressive state.
[Shanghai Arch Psychiatry. 2017;29(2): 95-103.
http://dx.doi.org/10.11919/j.issn.1002-0829.216098]
Mental Health Center of Shanghai Jiao Tong University School of Medicine, Shanghai, China
*Correspondence: Jianyin Qiu, Mailing address: No.600 South Wanping Road, Shanghai, China. Postcode: 200030. E-mail: jianyin_qiu@163.com; Lisheng Song. Mailing address: 600 South Wanping Road. Postcode: 200030. E-mail: slslulu@163.com
背景:抑郁症患者表现出明显的述情障碍,而关于其述情障碍的机制尚未明确,也较少有关于抑郁症患者情绪调节能力的研究。
目的:探索抑郁症患者的述情障碍特征,以及抑郁症状、述情障碍与个体情绪调节能力的关系。
方法:采用汉密尔顿抑郁量表(HAMD-24)、汉密尔顿焦虑量表(HAMA)、多伦多述情障碍量表(TAS)和计算机情绪调节实验,对36名抑郁症患者和31名健康志愿者进行评定分析。
结果:病例组中述情障碍发生率为66.67%,对照组为3.23%,两组比例差异有显著性(χ2=28.661,p<0.001)。病例组的TAS得分显著高于对照组(t=7.378,p<0.001)。情绪调节实验中,病例组观看中性图片的评分显著高于对照组(t=2.080,p=0.043);而负性-观看、负性-重评和负性-抑制三种实验条件下,两组评分无显著差异。在病例组中,HAMD-24、HAMA与TAS得分之间存在显著相关,而情绪调节实验得分与HAMD-24、HAMA、TAS之间均未发现相关。
结论:抑郁症患者中述情障碍的发生率可能高于一般人群,其抑郁症状与述情障碍之间可能存在相互影响。情绪调节能力可能是一种独立的特质,与抑郁状态无关。
Hao Zhang is currently a master’s student at Shanghai Jiao Tong University Medical School. She has been working at the Shanghai Mental Health Center since 2014. Her main research interests are depression and using mindfulness in the treatment of depression.
猜你喜欢
青少年科技博览(中学版)(2022年11期)2023-01-07
汽车维修与保养(2021年8期)2021-02-16
心理学报(2021年1期)2021-01-29
基层中医药(2020年5期)2020-09-11
初中生学习指导·中考版(2020年2期)2020-09-10
时代英语·高一(2019年1期)2019-03-13
中国医药指南(2017年3期)2017-11-13
军营文化天地(2017年4期)2017-06-15
现代电生理学杂志(2016年1期)2016-07-10
工业设计(2016年4期)2016-05-04
- 上海精神医学的其它文章
- Efficacy towards negative symptoms and safety of repetitive transcranial magnetic stimulation treatment for patients with schizophrenia: a systematic review
- Factors related to acute anxiety and depression in inpatients with accidental orthopedic injuries
- Placement instability among young people removed from their original family and the likely mental health implications
- Efficacy and metabolic influence on blood-glucose and serum lipid of ziprasidone in the treatment of elderly patients with first-episode schizophrenia
- The current situations and needs of mental health in China
- Factitious disorder - A rare cause for unexplained epistaxis