上颌前方牵引配合螺旋扩弓器治疗对替牙期骨性Ⅲ类错儿童颌面结构、上气道的影响
2017-10-26 01:46:09车霄楠
河北医药 2017年21期
车霄楠
doi:10.3969/j.issn.1002-7386.2017.21.004
车霄楠
目的探讨上颌前方牵引配合螺旋扩弓器治疗对替牙期骨性Ⅲ类错儿童颌面结构、上气道的影响。方法选取口腔科收治的替牙期骨性Ⅲ类错合儿童40例,根据随机数字表法分为研究组和对照组,每组20例。研究组患者给予上颌前方牵引配合螺旋扩弓器治疗,对照组给予上颌前方牵引治疗,比较2组患者颌面结构及上气道变化。结果治疗后,研究组17例患儿错完全解除;对照组8例患儿错完全解除;2组患者SNA、ANB、L1-MP、FH-MP、Ptm-A、SN-PP、ANS-Me、Wits值较治疗前比较,差异有统计学意义(P<0.05);且研究组ANB、FH-MP、SN-PP、ANS-Me、Wits值显著高于对照组(P<0.05),研究组U1-SN、L1-MP值显著低于对照组(P<0.05);2组PNS-R值较治疗前显著升高(P<0.05),且研究组显著高于对照组(P<0.05);2组SPL值较治疗前显著降低,但组间比较差异无统计学意义(P>0.05);2组患者NP volume、NP area、NP sag.、NP cor.值较治疗前显著升高(P<0.05),且研究组NP volume、NP area、NP sag.、NP cor.值显著高于对照组(P<0.05)。结论上颌前方牵引配合螺旋扩弓器治疗儿童替牙期骨性Ⅲ类错的效果良好,能够维持患者上下颌骨和牙列稳定,减少错复发,并且使患者的上气道间隙上部扩大,下部缩小,上气道容积得到增加,有利于呼吸功能改善。
上颌前方牵引;螺旋扩弓器;替牙期;颌面结构;上气道
1 资料与方法
1.1 一般资料 选取2014年1月至2016年1月收入我院口腔正畸科的替牙期骨性Ⅲ类错儿童40例,根据随机数字表法分为研究组和对照组,每组20例。研究组:男10例,女10例;年龄7~10岁,平均年龄(8.54±0.41)岁。对照组:男9例,女11例;年龄7~10岁,平均年龄(8.62±0.39)岁。纳入标准:(1)颈椎骨发育处于S1~S3期,颈椎骨龄7~10岁;(2)替牙期,前牙反,第一恒磨牙萌出;(3)矢状骨面型Ⅲ类,凹面型,-5°
1.2 治疗方法 研究组患者治疗方式是扩缩治疗,先扩后缩,给予上颌前方牵引配合螺旋扩弓器治疗;对照组给予上颌前方牵引治疗。(1)研究组患者采用Hass扩弓器,采用铸造式将不锈钢丝和上颌第一恒磨牙、第一前磨牙、第二前磨牙6个带环,通过螺旋扩弓器焊接成一整体,上尖牙近中焊接牵引钩,采用玻璃离子粘结带环。采用螺旋扩弓器进行快速扩弓,每次旋转1/4圈,每天加力2次,至深覆盖后牙。再行前方牵引,使用双杆可调式前方牵引器,牵引时间12~14 h/d,力值350~400 g,牵引方向为前下方,与平面呈20°~30°,至前牙错解除。(2)对照组患者采用粘结式上颌牙合垫矫治器,在尖牙近中颊侧放置牵引钩,采用玻璃离子粘结牙合垫,直接前方牵引。
1.3 观察指标 采用锥形束CT机、口腔X线计算机体层摄影系统(韩国VATECH公司),扫描条件为85 kV、8 mA,持续曝光24 s,球管频率36 kHz,层厚0.1~0.3 mm,影像重建时间180 s,探测器与X线焦点距离770.0 mm。
1.3.1 头影测量:所有患者于治疗前后拍摄头颅侧位片,进行头影测量,均由同一技师操作。
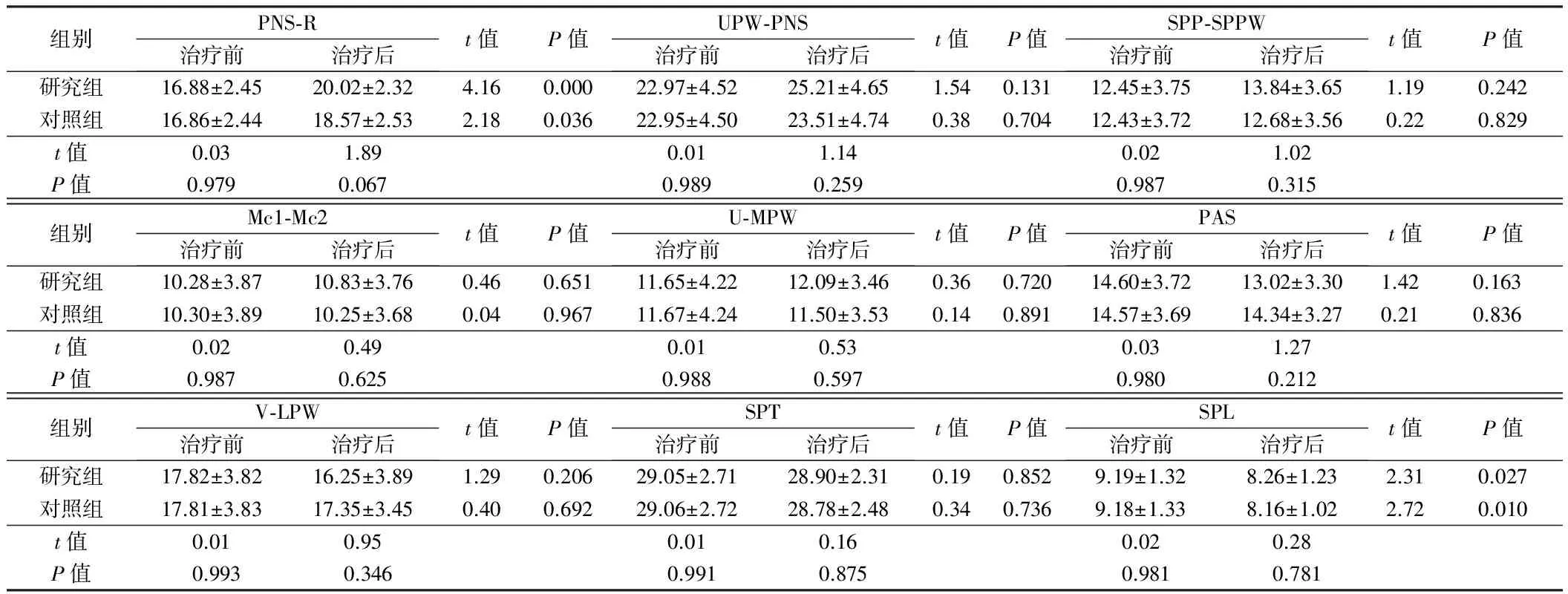
1.3.2 气道测量:所有患者于治疗前后拍摄头颅侧位片,进行气道测量,包括鼻咽直径(PNS-R)、硬腭后气道间隙(UPW-PNS)、软腭后-软腭后咽壁距离(SPP-SPPW)、软腭后气道间最狭窄处(Mc1-Mc2)、软腭尖与中后咽壁点间距离 (U-MPW)、TB点-TPPW点距离(PAS)、会厌点与下咽后壁点间距离(V-LPW)、软腭厚度(SPT)、软腭长度(SPL),均由同一技师操作。
1.3.3 上气道三维测量:所有患者于治疗前后,采用软件Mimics10.01重建上气道三维影像,包括鼻咽段容积(NP volume),鼻咽段最小截面积(NP area),最小截面积处矢状径(NP sag.),最小截面积处冠状径(NP cor.);口咽段容积(OP volume),口咽段最小截面积(OP area),最小截面积处矢状径(OP sag.),最小截面积处冠状径(OP cor.)。

2 结果
2.1 2组患者治疗效果比较 研究组患者治疗后,17例错完全解除,前牙覆牙合、覆盖正常,磨牙为正中关系;3例前牙呈对刃关系,磨牙为偏近中关系。对照组患者治疗后,错完全解除8例,磨牙为正中关系;12例磨牙为正中偏近中关系。
2.2 2组患者头颅侧位片指标比较 治疗前,2组患者检测指标比较差异无统计学意义(P>0.05);治疗后,2组患者SNA、ANB、L1-MP、FH-MP、Ptm-A、SN-PP、ANS-Me、Wits值较治疗前比较,差异有统计学意义(P<0.05);研究组ANB、FH-MP、SN-PP、ANS-Me、Wits值显著高于对照组,研究组U1-SN、L1-MP值显著低于对照组,差异有统计学意义(P<0.05);2组间SNB、Y轴角值比较差异无统计学意义(P>0.05)。见表1。

2.3 2组患者上气道间隙变化比较 治疗前,2组患者检测指标比较差异无统计学意义(P>0.05);治疗后,2组PNS-R值较治疗前显著升高,研究组显著高于对照组,差异有统计学意义(P<0.05);2组SPL值较治疗前显著降低,差异无统计学意义(P>0.05);2组UPW-PNS、SPP-SPPW、Mc1-Mc2、U-MPW、PAS、V-LPW、SPT值比较差异无统计学意义(P>0.05)。见表2。

组别PNS⁃R治疗前治疗后t值P值UPW⁃PNS治疗前治疗后t值P值SPP⁃SPPW治疗前治疗后t值P值研究组16.88±2.4520.02±2.324.160.00022.97±4.5225.21±4.651.540.13112.45±3.7513.84±3.651.190.242对照组16.86±2.4418.57±2.532.180.03622.95±4.5023.51±4.740.380.70412.43±3.7212.68±3.560.220.829t值0.031.890.011.140.021.02P值0.9790.0670.9890.2590.9870.315组别Mc1⁃Mc2治疗前治疗后t值P值U⁃MPW治疗前治疗后t值P值PAS治疗前治疗后t值P值研究组10.28±3.8710.83±3.760.460.65111.65±4.2212.09±3.460.360.72014.60±3.7213.02±3.301.420.163对照组10.30±3.8910.25±3.680.040.96711.67±4.2411.50±3.530.140.89114.57±3.6914.34±3.270.210.836t值0.020.490.010.530.031.27P值0.9870.6250.9880.5970.9800.212组别V⁃LPW治疗前治疗后t值P值SPT治疗前治疗后t值P值SPL治疗前治疗后t值P值研究组17.82±3.8216.25±3.891.290.20629.05±2.7128.90±2.310.190.8529.19±1.328.26±1.232.310.027对照组17.81±3.8317.35±3.450.400.69229.06±2.7228.78±2.480.340.7369.18±1.338.16±1.022.720.010t值0.010.950.010.160.020.28P值0.9930.3460.9910.8750.9810.781
2.4 2组患者上气道三维变化比较 治疗前,2组患者上气道三维数据比较差异无统计学意义(P>0.05);治疗后,2组患者NP volume、NP area、NP sag.、NP cor.值较治疗前显著升高,且研究组NP volume、NP area、NP sag.、NP cor.值显著高于对照组,差异有统计学意义(P<0.05);2组间OP volume、OP area、OP sag.、OP cor.值比较差异无统计学意义(P>0.05)。见表3。

组别NPvolume(mm2)治疗前治疗后t值P值NParea(mm2)治疗前治疗后t值P值NPsag.(mm)治疗前治疗后t值P值研究组3461.94±1146.454722.98±1010.943.690.000175.98±34.28199.85±35.842.150.00010.32±1.4812.45±1.254.920.000对照组3461.81±1147.524492.28±985.483.340.000176.15±33.81190.47±34.821.780.02310.34±1.4211.84±1.341.150.049t值0.003.410.024.850.043.93P值1.0000.0010.9870.0000.9650.000组别NPcor.(mm)治疗前治疗后t值P值OPvolume(mm2)治疗前治疗后t值值P值OParea(mm2)治疗前治疗后t值P值研究组26.97±3.9229.78±4.322.150.0387235.85±2397.547335.45±2476.810.130.898199.64±63.54222.21±68.841.080.288对照组27.01±3.9028.94±4.251.960.0477235.82±2396.377532.28±2364.270.390.696199.58±63.49211.63±57.240.630.532t值0.033.350.000.260.000.53P值0.9740.0041.0000.7990.9980.600组别OPsag.(mm)治疗前治疗后t值P值OPcor.(mm)治疗前治疗后t值P值研究组10.95±1.6311.58±1.331.340.18829.47±4.4830.43±4.620.670.509对照组11.01±1.6710.75±1.260.560.58229.51±4.5230.28±4.610.530.597t值0.112.040.030.10P值0.9090.0510.9780.919
3 讨论
上颌前方牵引是通过改变上下颌骨的生长方向,达到改变面型的目的,主要是前移上颌骨和后移下颌骨[6]。在前移上颌骨前,可以采用螺旋扩弓器快速扩弓,使骨缝被打开,从而刺激间质细胞生长,使得前方牵引更加稳定[7]。研究指出骨性Ⅲ类错可在快速扩缩弓后再行牵引[8]。采用上颌扩缩治疗,一方面能够防止上颌牙弓宽度过大,维持正常咬合;另一方面可以刺激上颌骨缝,使牵引稳定性增加[9]。目前,研究认为上颌前方牵引治疗不仅能够解除错,还可以改善患者的面部软组织,影响患者的上气道间隙[10]。
有报道上气道间隙与呼吸、吞咽有密切关系,而上气道间隙与颌面结构有关[12]。由于不良习惯等使上颌骨向后移位,造成上颌平面的气道较窄,导致通气障碍,进一步影响颌面骨发育,出现骨性错[13]。上颌前方牵引能够改变上颌骨的生长,且牵拉软腭根部,进而影响气道。本研究结果显示,治疗后,2组PNS-R值较治疗前显著升高,研究组显著高于对照组,差异有统计学意义(P<0.05);2组SPL值较治疗前显著降低,但组间比较差异无统计学意义(P>0.05)。说明替牙期骨性Ⅲ类错儿童给予上颌前方牵引治疗后,患者上气道上部间隙明显增大,下部缩小。
综上所述,上颌前方牵引配合螺旋扩弓器治疗儿童替牙期骨性Ⅲ类错的效果良好,能够维持患者上下颌骨和牙列稳定,减少错复发,并且使患者的上气道间隙上部扩大,下部缩小,上气道容积得到增加。
1 Xu Y,Zhu P,Le L,et al.Conservative treatment for a growing patient with a severe,developing skeletal Class III malocclusion and open bite.American Journal of Orthodontics and Dentofacial Orthopedics,2014,145:807-816.
2 赵斌斌,孟丹洁,阮文华,等.人胎儿前颌缝发育与骨性Ⅲ类错儿童的中面部形态特征.国际口腔医学杂志,2014,41:184-186.
3 陶丽.正颌手术对骨性Ⅲ类患者上气道及周围结构影响的研究.口腔颌面外科杂志,2014,24:72-76.
4 Celikoglu M,Oktay H.Effects of maxillary protraction for early correction of class Ⅲ malocclusion.European journal of orthodontics,2014,36:86-92.
5 章依文,沈刚.上颌骨前方牵引配合快速括弓治疗骨性Ⅲ类错畸形的疗效分析.上海口腔医学,2016,25:327-333.
6 朱吉坤,张桂荣,郭艳明,等.上颌前方牵引矫治骨性Ⅲ类错儿童鼻上颌复合体部软组织变化的研究.国际儿科学杂志,2014,41:312-315.
7 陈磊,吴高义,段银钟,等.前方牵引联合快速扩弓治疗成人骨性反1例.实用口腔医学杂志,2014,30:435-437.
8 张贺佳,孙晓菊,张辉,等.上颌前方牵引器矫治骨性Ⅲ类错畸形的临床研究.中国美容整形外科杂志,2015,26:109-111.
9 Wang B,Shen G,Fang B,et al.Augmented corticotomy-assisted surgical orthodontics decompensates lower incisors in class Ⅲ malocclusion patients.Journal of Oral and Maxillofacial Surgery,2014,72:596-602.
10 王宏伟,齐素青,闫明,等.正畸联合下颌升支矢状劈开截骨术治疗骨性Ⅲ类错对上气道影响的锥形束CT分析.中华口腔医学杂志,2015,50:615-618.
11 张婕,李小彤.骨性Ⅲ类错手术患者的前牙代偿特征分析.中华口腔医学杂志,2015,50:656-660.
12 王天虎,杨芳,张明烨,等.成人骨性Ⅱ类错不同垂直骨面型上气道三维分析研究.口腔医学,2014,34:192-196.
13 王宏伟,齐素青,闫明,等.正畸联合下颌升支矢状劈开截骨术治疗骨性Ⅲ类错对上气道影响的锥形束CT分析.中华口腔医学杂志,2015,50:615-618.
14 秦燕军,沈云娟,谷妍,等.骨性Ⅲ类畸形上颌前方牵引治疗的三维测量分析.上海口腔医学,2014,23:699-703.
EffectsofmaxillaryprotractioncombinedwithscrewexpansiononmaxillofacialstructureandupperairwayofchildrenwithclassⅢmalocclusioninmixeddentition
CHEXiaonan.
DepartmentofStomatology,Children’sHospitalofXuzhouCity,Jiangsu,Xuzhou221000,China
ObjectiveTo investigate the effects of maxillary protraction combined with screw expansion on maxillofacial structure and upper airway of children with class Ⅲ malocclusion in mixed dentition.MethodsForty children with class Ⅲ malocclusion in mixed dentition who were treated in our hospital were enrolled in the study,who were divided into observation group and control group,with 20 patients in each group.The patients in observation group were treated by maxillary protraction combined with screw expansion,however,the patients in control group were treated by maxillary protraction only.The changes of maxillofacial structure and upper airway were observed and compared between two groups.ResultsAfter treatment,the 17 patients with malocclusion in observation group was completely cured,in contrast to that, the 8 patients with malocclusion in control group was completely cured. There were significant differences in the levels of SNA,ANB,L1-MP,FH-MP,Ptm-A,SN-PP,ANS-Me,Wits in both groups before treatment and after treatment (P<0.05),moreover, the levels of ANB,FH-MP,SN-PP,ANS-Me,Wits in observation group were significantly higher than those in control group (P<0.05),however, the levels of U1-SN,L1-MP in observation group were significantly lower than those in control group (P<0.05). After treatment,PNS-R levels in both groups were significantly increased,as compared with those before treatment (P<0.05).The SPL levels in both groups were significantly decreased after treatment,as comapred with those before treatment, however, there were no significant differences between two groups (P>0.05).After treatment,the NP volume,NP area,NP sag.,NP cor value in both groups were significantly increased,as compared with those before treatment,moreover, the NP volume,NP area,NP sag and NP cor value in observation group were significantly higher than those in control group (P<0.05).ConclusionThe therapeutic effects of maxillary protraction combined with screw expansion in treatment of class Ⅲ malocclusion in mixed dentition are satisfactory,which can maintain the stablity of upper and lower jaws and teeth,decrease the relapse rate of malocclusion, moreover,which can expand upper airway gap and decrease lower airway gap to increase the upper airway volume and improve respiratory function.
maxillary protraction;screw expansion;mixed dentition;maxillofacial structure;upper airway
R 782.2
A
1002-7386(2017)21-3217-04
2017-04-18)
221000 江苏省徐州市儿童医院口腔科
猜你喜欢
口腔医学(2021年10期)2021-12-02 02:07:42
中华肩肘外科电子杂志(2020年1期)2020-08-24 07:04:10
中华老年口腔医学杂志(2019年6期)2019-12-27 03:46:34
反射疗法与康复医学(2017年7期)2017-01-16 01:11:42
中华老年口腔医学杂志(2016年2期)2017-01-15 14:24:52
中华老年口腔医学杂志(2016年2期)2017-01-15 14:24:48
中华老年口腔医学杂志(2016年1期)2017-01-15 14:24:43
中国卫生标准管理(2015年25期)2016-01-14 09:29:17
河北医药(2015年13期)2015-11-13 06:20:07
实用手外科杂志(2015年3期)2015-08-27 01:53:14