
Study on the development and usage of a cardiopulmonary resuscitation time point recorder
2017-10-20 03:06LingZhouHuiLiHongyanWeiChunlinHuXiaoliJingHongZhanXiaoxingLiaoXinLi3FireCorpsMedicalDepartmentofHunanProvinceChangshaChina
Ling Zhou, Hui Li, Hong-yan Wei, Chun-lin Hu, Xiao-li Jing, Hong Zhan, Xiao-xing Liao, Xin Li3 Fire Corps Medical Department of Hunan Province, Changsha, China
2 Department of Emergency Medicine, The First Aff i liated Hospital, Sun Yat-sen University, Guangzhou, China
3 Department of Emergency Medicine, Department of Emergency and Critical Care medicine, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China
Study on the development and usage of a cardiopulmonary resuscitation time point recorder
Ling Zhou1, Hui Li2, Hong-yan Wei2, Chun-lin Hu2, Xiao-li Jing2, Hong Zhan2, Xiao-xing Liao2, Xin Li31Fire Corps Medical Department of Hunan Province, Changsha, China
2Department of Emergency Medicine, The First Aff i liated Hospital, Sun Yat-sen University, Guangzhou, China
3Department of Emergency Medicine, Department of Emergency and Critical Care medicine, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China
BACKGROUND: To invent a novel cardiopulmonary resuscitation (CPR) time point recorder to synchronously and automatically record the time and to identify its effectiveness in humans.
METHODS: A CPR time point recorder was invented after the doctors were familiar with the traditional Utstein recovery registration mode and mastered the registration time points required. The progress of CPR was simulated. The standard and correct times were recorded, and the doctors performing the recovery collected the data about the times using our CPR time point recorder or the memory registration mode.
RESULTS: The deviation times were 21.4±24.7 seconds for the memory group and 3.57±4.58 seconds for CPR time point recorder group. The deviation of times increased significantly depending on the increase of the operation items in the memory group. A similar phenomenon was found in the timer group but with a smaller difference (P<0.01).
CONCLUSION: A CPR time point recorder could reduce the deviation of operate-time,especially after a long-time operation, and for procedures with more operating items, compared with the memory mode. It was a more advantageous and accurate method for the Utstein registration.
Cardiopulmonary resuscitation; Time point recorder; Utstein registration
INTRODUCTION
In 1997, the in-hospital cardiopulmonary resuscitation Utstein registration mode was presented after the prehospital Utstein style was proposed in 1991.[1]In 2004,the simplified Utstein registration model was published and recommended the use of a "clock" in the Utstein registration, which could synchronize and datamate time recording during the CPR process. Thus, the standard practice of registration by memorization has changed.[2,3]The aim of this study is to develop a clock to record CPR time, name the CPR time point recorder, and to identify its effectiveness.
METHODS
Designing the registration time points
Based on the Utstein mode, we selected 13 time points for counting. These time points are the "time of unconscious", "call time", "departure time of the medical staff", "arrival time of the medical staff", "airway opening time", "artif i cial ventilation time", "the fi rst ECG recording time", "chest compression time", "def i brillation time", "medicine taking time", "intubation time", "time of return of spontaneous circulation (ROSC)", and "end time of resuscitation" (Figure 1A).
The research and development of the CPR time point recorder
The CPR time point recorder was designed with the cooperation of professional engineers.
Overall designation
In the process of CPR, the real-time relevant data was recorded and collected by the CPR time point recorder and then transferred to the computerized collecting system (the CPR data collection system in the Emergency Department of the First Aff i liated Hospital of Sun Yat-sen University)through a data converter. Finally, the outputs of relevant data were printed out (Figure 1B).
Designing the key modules of the CPR time point recorder
Beijing time was input as the time circuit module and the time can be automatically updated after the recorder is turned on. The CPR time point recorder could typically work under a power module powered not only by an alternating current but also by nickel hydride batteries. The input programs and data could be observed through the Liquid Crystal Display (LCD) module. Both real-time data collection and function selection could be carried out using the keyboard control module. The storage and output of the data are respectively carried out using both storage and communication interface modules(Figure 1C).
The interface of computerized collection in the CPR recovery timer
The CPR data collection system in the Emergency Department of the First Affiliated Hospital of Sun Yatsen University was made to improve the accuracy and efficiency of CPR data collection. The software could be operated after connecting to computers and the data could be easily collected, stored and transmitted(Figure 2).
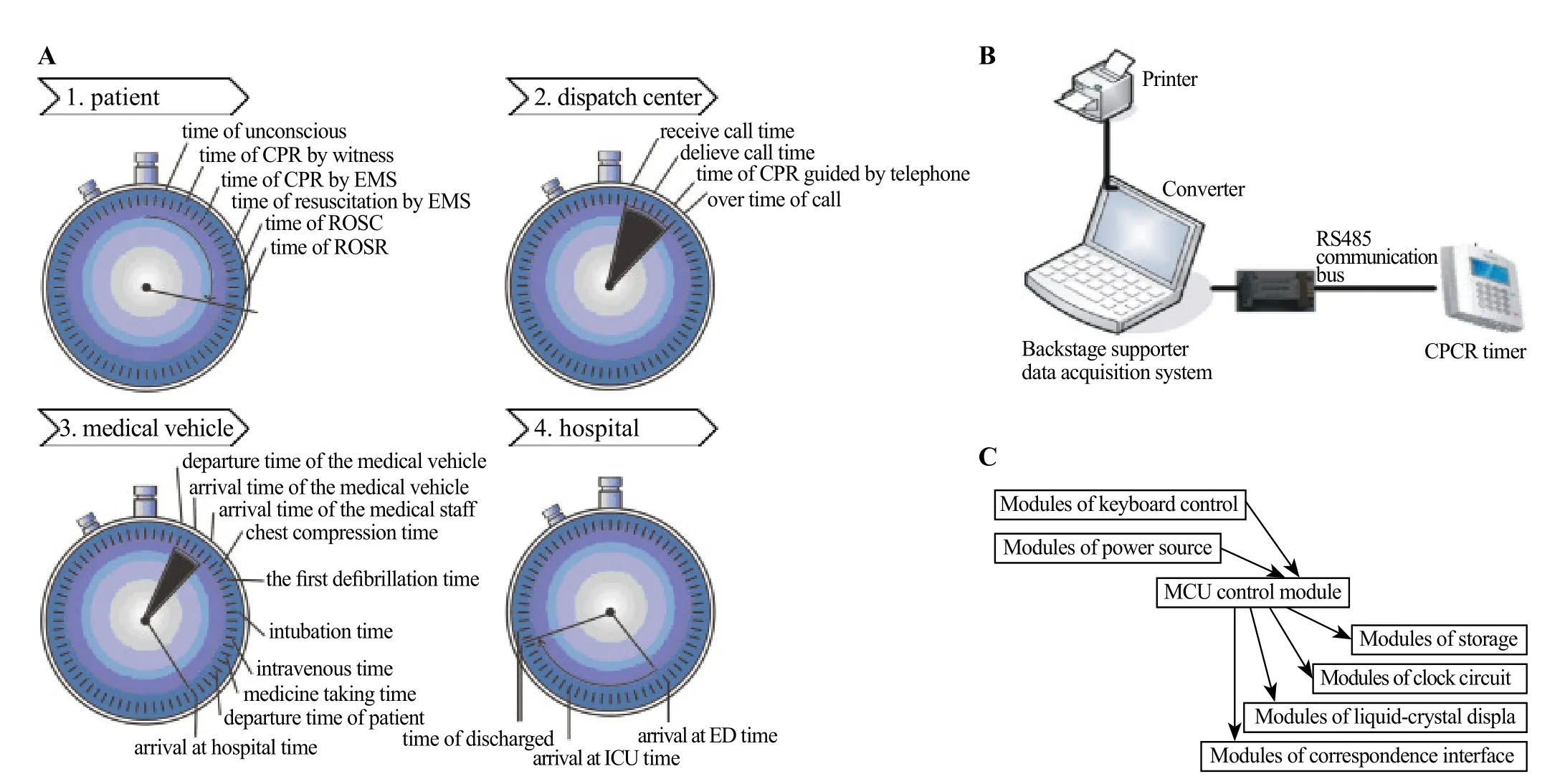
Figure 1. Design of CPR time point recorder. A: CPR recovery time registration points; B: The general design idea of the CPR time point recorder; C: The function modules of the CPR time point recorder.
Simulating CPR and detecting the efficacy of the CPR time point recorder
The recovery programs were randomly simulated at CPR scenes, including opening airway, intubation,respiratory sac assisted ventilation, chest compressions,defibrillation, administration, and so on. The subjects were divided into two groups: the CPR time point recorder group and the memory group. After the doctors in the two groups were familiar with the 13 time points, the experiments began. The CPR time point recorder group recorded time using the CPR time point recorder while the doctors performed the CPR operation. The relevant data were transmitted as the experimental data from the time recorders to the computers when the experiment was completed in the CPR time point recorder group. The doctors in the memory group filled in the recovery registration forms by watching the clock on the wall to collect the data after the CPR. During the process of CPR, the time points were counted by hand with a stopwatch(made in Shanghai diamond watch factory), which was considered the standard method of data collection. Any uncompleted data were excluded.
Statistical analysis
The SPSS 10.0 statistical software package was used for statistical analysis. All data are expressed as the mean±SD. For data with a normal distribution, the t test was used for the homogeneity of variance test and the t'test was used for the heterogeneity of variance test. The correlation of two random variables was assessed by the "Pearson correlation analysis", and linear regression was used for regression. A 2-tailed value of P<0.05 was considered statistically significant.
RESULTS
General information about the experiment
Fourteen doctors took part in the experiment; each experienced the CPR process twice and took a good rest during intervals between the CPR processes. For one time, the doctors collected the data via the CPR time point recorder; the other time, the doctors filled in the recovery registration forms with his memories at the end of the CPR process. Some other emergency medicine physicians and nurses provided on-scene medical rescue procedures, administered drugs and performed advanced procedures. In final, 14 sets of data were collected,including memory time, CPR time point recorder time and stopwatch time in one set of data.
The deviation between the memory group and the CPR time point recorder group
Deviation is obtained by subtracting stopwatch time from memory time or CPR timepoint recorder time. The absolute value of deviation of the memory group and the CPR timepoint recorder group were 21.4±24.7 seconds and 3.57±4.58 seconds, respectively. The former was significantly longer than the latter (P<0.01) (Figure 3).
The correlation between the deviation and operating time
In the memory group, the deviation was gradually increased in correspondence to a longer operating time.The correlation coefficient was r=0.548, the coefficient of determination was r2=0.2998, F=38.531 (P<0.001).The regression was valid and the regression equation was y=0.204x+8.357. In the CPR time point recorder group,the deviation of the timer group gradually increased with a long-time operation also. The correlation coeff i cient was r=0.288, the coefficient of determination was r2=0.084,F=4.06 (P=0.046). The regression was valid and the regression equation was y=0.011x+2.367 (Figure 4).
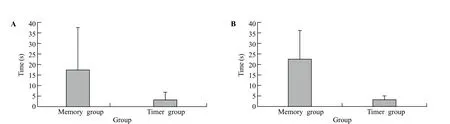
Figure 3. Comparisons between memory group and timer group. A: The general tolerance comparisons between memory group and timer group.In the memory group, the general tolerance was 21.4±24.7 seconds, while in the timer group was 3.5±1.6 seconds. There is statistical difference between the two groups (P=0.000). B: The mean tolerance comparison between memory group and timer group. In the memory group, the mean tolerance was 22.3±13.7 seconds, and in the timer group was 3.57±4.58 seconds. The former was significantly longer than the latter (P<0.01).
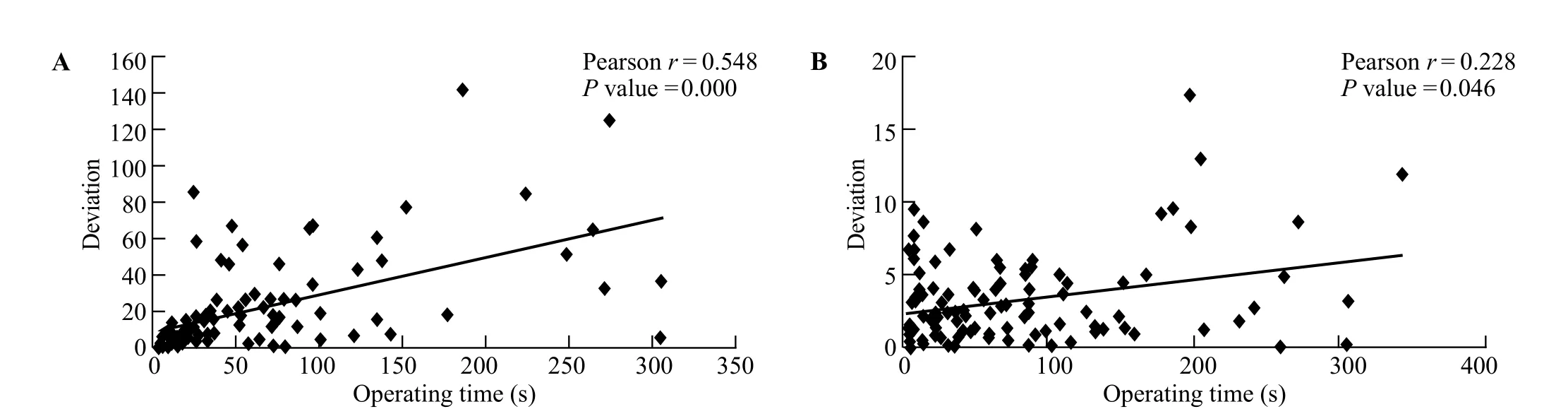
Figure 4. Relationship of deviation and operating time in the memory group and CPR time point recorder group. A: In memory group, analysis revealed a significant correlation between deviation and the operating time (Pearson r=0.548, P=0.000, 2-tailed t-test). B: In contrast to the memory group, the deviation of timer group is gradually increased with longer operating time in CPR time point recorder group (Pearson r=0.228,P=0.046, 2-tailed t-test).
The relationship between the deviation and operating items in the memory group
In the memory group, the deviation gradually increased with more operating items. The correlation coefficient was r=0.513, the coefficient of determination was r2=0.2663, F=35.38 (P=0.000). The regression was valid and the regression equation was y=0.204x+8.357. In the CPR time point recorder group, the deviation gradually increased with more operating items. The correlation coefficient was r=0.22, the coefficient of determination was r2=0.05, F=5.48 (P=0.02). The regression was valid and the regression equation was y=0.41x+1.68.
A comparison of the positive and negative bias between the memory group and the timer group
In the memory group, the negative bias was 44%(the recording time was earlier than the stopwatch time),yet the positive bias was 56% (the recording time was later than the stopwatch time). However, there were no significant differences between the positive and negative biases (P=0.862). In the CPR time point recorder group,the negative bias was 76%, yet the positive bias was 24%. However, there were no significant differences between the positive and negative biases (P=0.448).
DISCUSSION
The CPR time point recorder could reduce errors caused by memorization. Because the environment of CPR is very complex and the process of CPR involves many operations.[4,5]
The Utstein registration mode is commonly used for CPR data acquisition, and requires the recording of many times into tables, including the "Coma- The first ECG recording time", "Coma- The first compression time","Coma- The first defibrillation time". All of these time points are very important. However, it is difficult for the medical staff to record all of the time points accurately after the rescue process.
In 2005, researchers collected 10 689 Utstein registrations on pulseless electrical activity patients in 176 hospitals. They found that 10.9% of the data did not include the time. The numbers for the practical operating items and the register operating items were different. The tools for timing were not standardized: 21% of the form fillers consulted the clock in the emergency room, 30%of the form fi ller consulted their own watches, and 16%of them used stopwatches. In the absence of uniform standard recorders, the average time deviation was 2.83 minutes during the registration process of the recovery information.[6]
In this study, the staff was informed of the purpose and memorized the time points more consciously.Hence, the deviation of 2.83 minutes was less than the formal value. There were significant differences between the memory group and the CPR time point recorder group. Because the CPR time point recorder had manoeuvrability, synchronicity and accuracy advantages over mechanical memory, the CPR time point recorder group reduced more errors than the memory group. In the experimental group, the medical staffs were only required to press a button on the CPR time point recorder as soon as the relevant medical operation was finished.The data was much easier to access and were more accurate. Alternatively, the medical staffs in the control group needed to watch the clock while preforming the relevant operations, which caused a variety of interfering factors, including the accuracy of time recorded for the operating position, forgetting to observe the time and data disorientation. Therefore, the use of the CPR time point recorder was optimal compared to mechanical memory with the human brain. The errors caused by multiple operating-items and prolonged operation time were reduced by the CPR time point recorder. Ebbinghaus discovered the law of memory: the capacity of memory is close to 100%, yet it descends to 58.2%, 44.2%, and 33.7% after 20 minutes, 1 hour, and 24 hours, respectively. Only 21% of memory capacity is retained after 1 month.
In our study, the medical staff in the memory group collected relevant data using their memories. The medical staffs might notice and remember the specif i c time point/time interval at the beginning. Prolonged operating procedures brought more unexpected situations.However, the accuracy of memory decreased as the memory content gradually increased, which is consistent with the human memory law. The data collected by the CPR time point recorder could avoid some interference.Nevertheless, the concept of real-time recording could delay the recording time points as operate-time and operating items increasing. However, the deviation was relatively reduced compared with the memory group.
This study implied that the correlation coefficients between the deviation and operating time and items were more than 0.5 in the memory group, but the correlation coefficients were less than 0.30 in the CPR time point recorder group. Many operating items were included in the CPR process and many data were required by the Utstein registration mode. With the research and development of the CPR recovery timer, we could avoid interference during CPR and the data could be intuitively recorded.
CONCLUSION
Our study demonstrates that a CPR time point recorder could reduce the deviation of operate-time compared with the memory mode. However, there were only 14 sets of data assessed in this research. Therefore, the effectiveness of the CPR time point recorder deserves further investigation.
Funding: This study was supported by funding from the NSFC(81671882, 81471832), the Natural Science Foundation of Guangdong Province of China (2016A030311039), the Science and Technology Foundation of Guangzhou City of China (201605110853481). The funders had no role in the study design, data collection, analysis,decision to publish or the preparation of the manuscript.
Ethical approval: Not needed.
Conflicts of interest: The authors have no competing interests relevant to the present study.
Contributors: Zhou L and Li H contributed equally to this work.All authors read and approved the final version of the manuscript.
1 American Heart Association; International Liaison Committee on Resuscitation (ILCOR). Proceedings of the Guidelines 2000 Conference for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: An International Consensus on Science.Ann Emerg Med. 200,37(4 Suppl):S1–200.
2 International Liaison Committee on Resuscitation. 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 4: Advanced life support.Resuscitation. 2005,67(2–3):213–47.
3 Ornato JP, Doctor ML, Harbour LF, Peberdy MA, Overton J,Racht EM, et al. Synchronization of timepieces to the atomic clock in an urban emergency medical services system. Ann Emerg Med. 1998, 31(4):483–7.
4 Nambiar M, Nedungalaparambil NM, Aslesh OP. Is current training in basic and advanced cardiac life support (BLS &ACLS) effective? A study of BLS & ACLS knowledge amongst healthcare professionals of North-Kerala. World J Emerg Med. 2016;7(4):263–9.
5 Kobras M, Langewand S, Murr C, Neu C, Schmid J. Short lessons in basic life support improve self-assurance in performing cardiopulmonary resuscitation. World J Emerg Med. 2016;7(4):255–62.
6 Kaye W, Mancini ME, Truitt TL. When minutes count–the fallacy of accurate time documentation during in-hospital resuscitation. Resuscitation, 2005,65:285–90.
Accepted after revision May 3, 2017
Xin Li, Email: xlidoct@qq.com
World J Emerg Med 2017;8(3):195–199
10.5847/wjem.j.1920–8642.2017.03.006
December 10, 2016
 World journal of emergency medicine2017年3期
World journal of emergency medicine2017年3期
- World journal of emergency medicine的其它文章
- Emergency department procedural sedation for primary electrical cardioversion — a comparison with procedural sedations for other reasons
- The presenting and prescribing patterns of migraine in an Australian emergency department: A descriptive exploratory study
- Comparison of ultrasound-measured properties of the common carotid artery to tobacco smoke exposure in a cohort of Indonesian patients
- Validating a point of care lactate meter in adult patients with sepsis presenting to the emergency department of a tertiary care hospital of a low- to middle-income country
- Can patients with non-convulsive seizure be identif i ed in the emergency department?
- Out of hospital cardiac arrest resuscitation outcome in North India — CARO study